Embed Size (px)
Citation preview

Pharmacotherapy of
Heart Failure
Nidhi MaheshwariPharmacology

BASIC PHYSIOLOGY
MAP = CO X SVR
HR SV
ANS
PRELOAD
CONTRACTILITY
AFTERLOAD
ATRIAL CONTRACTION
VENOUS RETURN
LV VOLUME LV THICKNESS
AORTIC PRESSURE
SVRBLOOD VOLUME AT EJECTION

Questions covered
1) Describe recent advances in drug therapy of CCF/HF
2) Describe the present status of drugs used in management of CHF
3) Current and recent advances in treatment of CHF
SAQ
1) Role of beta blockers in HF & individual drugs

Background & incidence• Incidence- 1.0-5.0 / 1000/ annum.
• Only cardiovascular disease : increasing in incidence and prevalence.
• Over 1 million patients hospitalized annually
• 50,000 deaths annually
• 5 yr mortality- 50%

DefinitionHeart failure
• complex clinical syndrome
• from structural or functional cardiac disorder
• impairs the ventricular ability to fill with or eject blood sufficiently required to meet body’s metabolic demands
Clinical manifestations
dyspnea (pulmonary congestion) and fatigue (reduced exercise tolerance)



Compensatory responses…Myocardial disease(decreased contractility)(decreased stroke volume)
Decreased renal perfusion
RAAS activation
VasoconstrictionIncreased afterload
Sympathetic activation
Increased heart ratevasoconstriction
Increased after loadO2 demand
Cardiac dilatationCardiac hypertrophy
Increased cardiac contractility
Increased cardiac O2 demand & work

• Maintain Cardiac Output by compensatory mechanisms
• In long term, increase work load and worsens cardiac performance
• Compensatory mechanisms become exhausted and ineffective after a long time
• TPR and after load increases-> decreasing the ejection fraction
• Preload is increased due to increased blood volume and venous tone
• When adaptive mechanisms fail to maintain Cardiac Output-decompensated heart failure
Signs and symptoms of decompensated HF : dyspnoea with cyanosis, hepatomegaly, cardiomegaly, reflex tachycardia(?), decreased urine formation, decreased exercise tolerance and muscle fatigue

Syndrome( multiple causes)
• MI/Angina• HT• Ventricular Tachycardia
• Hyperthyroidism• Anaemia• Berry-berry
Low CO
High CO
Medications
Treat Cause

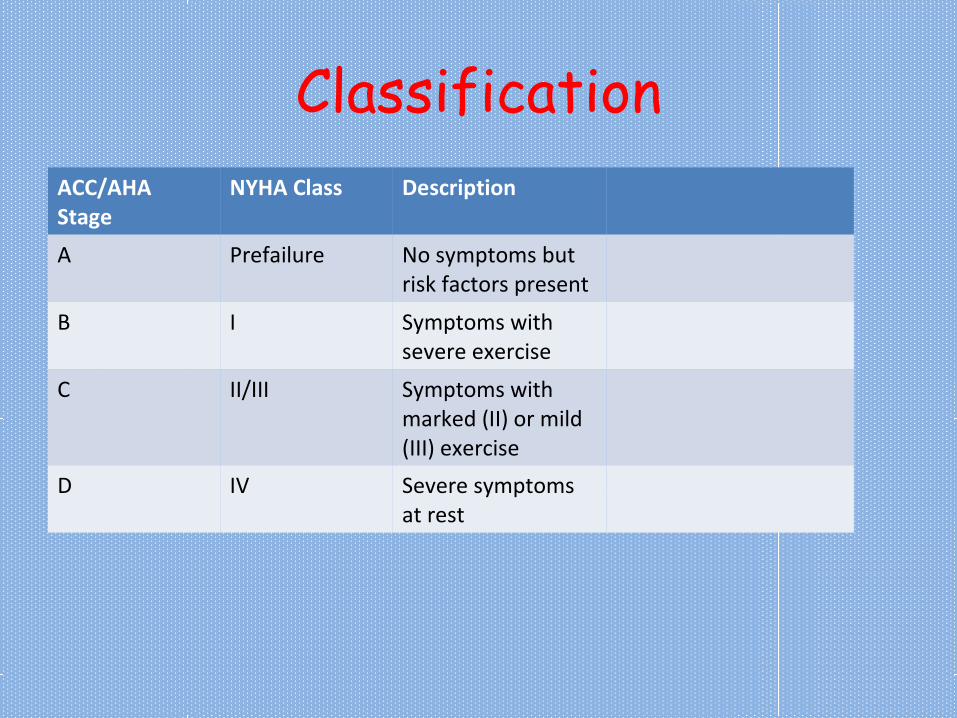
ClassificationACC/AHA Stage
NYHA Class Description
A Prefailure No symptoms but risk factors present
B I Symptoms with severe exercise
C II/III Symptoms with marked (II) or mild (III) exercise
D IV Severe symptoms at rest

Treatment of Chronic HF patients 4
ACC/AHA Stage
NYHA Class Description Management
A Prefailure No symptoms but risk factors present
Treat obesity, HT, Diabetes, Hyperlipidemia
B I Symptoms with severe exercise
ACEI/ARBΒ blockersdiuretics
C II/III Symptoms with marked (II) or mild (III) exercise
AddAldosterone antagonists, Digoxin, CRT, Hydralazine/nitrate
D IV Severe symptoms at rest
TransplantLVADCRT: cardiac resynchronization therapy; LVAD: left ventricular assisted device


Management of acute heart failure4
1) IV furosemide
2) IV Dopamine/Dobutamine: in HF + severe hypotension
3) IV levosimendan (alternative to β agonist)
4) Vasodilators- IV nitroprusside, nitroglycerine, nesiritide
5) Vasopressin antagonists- Conivaptan, Tolvaptan: in HF with hypovolemia( ? Is it hypervolemia)

Pharmacotherapy & Pharmacology

Positive Inotropic Agent
a) Cardiac Glycosides: Digoxin
b) Bipyridines or PDE inhibitors: Inamrinone, Milrinone, Levosimendan, Enoximone
χ) β Adrenergic Agonists: Dopamine, Dobutamine, Dopexamine

Without Inotropic effects
a) Diuretics: Furosemide, Bumetanide, Hydroclorothiazide, Metolazone, Spironolactone, Eplerenone
b) ACEI: Enalapril, Lisinopril, Ramipril
c) AT1 receptor anatgonists: Losartan, Valsartan
d) Β blockers: Carvedilol, Bisoprolol, Metoprolol
e) Vasodilators: Hydralazine, Sodium nitroprusside, Isosorbide di nitrate, Nesiritide
f) Vasopressin Receptor Antagonists: Conivaptan, Tolvaptan

ACE inhibitors• First line agents in asymptomatic ventricular dysfunction
• Combination with diuretics make first line therapy in HF
Enalapril 2.5 mg BD ( max 10 mg BD)
Lisinopril 2.5-5 mg OD ( max 20 mg OD)
Ramipril 2.5 mg OD ( max 10 mg OD)

• Slow : progress of ventricular dilatation
• Prolong survival : prevent pathological remodeling : heart & blood vessels
• Beneficial in MI (stroke, arrhythmia)
• Use : asymptomatic to severe HF
• Side effects: hypotension, hyperkalaemia, cough, urticaria, angioedema, altered taste, fetopathic
• Aldosterone escape is prevented by adding Spironolactone with ACEI. combination also reduces mortality.

ARBs: (AT1 receptor blockers)
• Beneficial hemodynamic effects similar to ACEI
• Used when ACEI are Cx (excessive cough or angioedema) or not tolerated
• Side effects of ARBs : hypotension,hyperkalaemia, headache, dizziness, fetopathic
Losartan:Most common ARB s in CHF T1/2: 2 hrsB.A.: 33%Dose: 50 mg OD/BDLess first dose hypotension
Valsartan:T1/2 : 6-9 hrsB.A.: 23%Dose: 80-160 mg OD

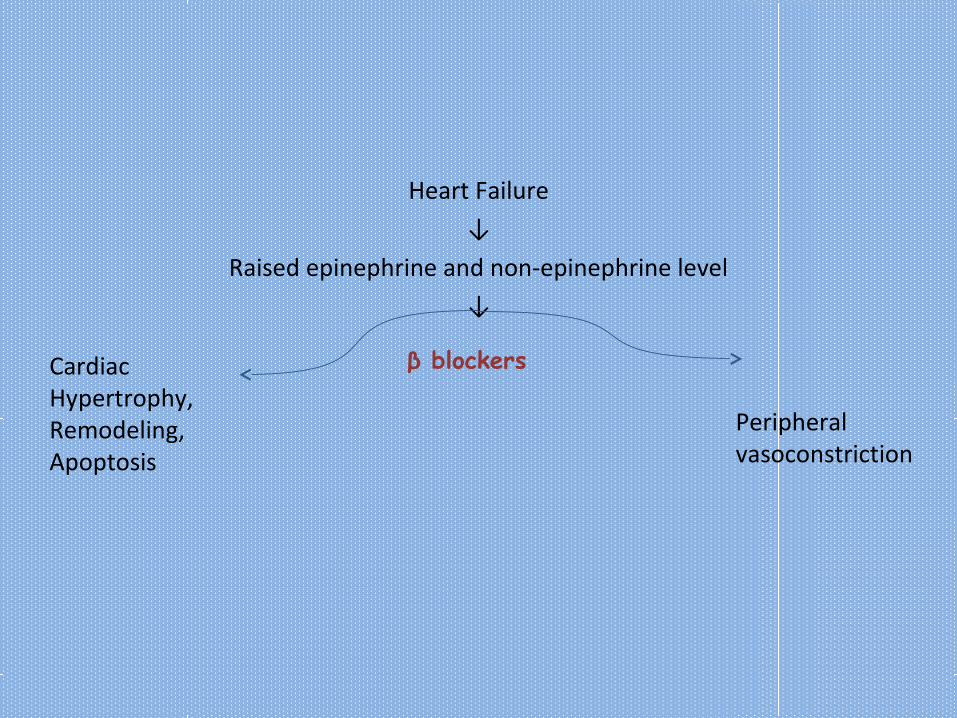
Heart Failure
↓
Raised epinephrine and non-epinephrine level
↓
Cardiac Hypertrophy, Remodeling, Apoptosis
Peripheral vasoconstriction
Heart Failure
↓
Raised epinephrine and non-epinephrine level
↓
Cardiac Hypertrophy, Remodeling, Apoptosis
Peripheral vasoconstriction
β blockers

Carvedilol
• α1 + β1 + β2 antagonist
• T1/2- 6-8 hrs
• Dose: 3.125 mg BD for 2 weeks, if well tolerated gradual ↑ to max 25 mg BD( max)
• Inhibits free radical induced lipid peroxidation, inhibits vascular smooth muscle mitogenesis and also block L type voltage gated channels-> cardioprotective in CHF
β blockers

Metoprolol• T1/2: 3-6 hrs• Dose: 100 -200 mg (max)
Bisoprolol• T1/2: 9-12 hrs• OD is enough• Dose: 2.5 -10 mg (max)
Nebivolol• Also NO donor-vasodilatation and improve endothelial function• Dose: 5mg OD• Effective in systolic & diastolic function

• Use in mild-moderate (NYHA II/III) systolic dysfunction with cardiomyopathy
• Benefit seen in symptomatic
• Initiate at low doses and up titrate to max dose
• 2-4 months therapy is required for clinical benefits
• Do not start in decompensated HF
• Sustained released metoprolol or 2-3 times daily dosing should be preferred
• Clinical improvements are slight rise in ejection fraction, reduction in HR, reduction in symptoms
• Long term effect: maintain hemodynamic benefits and reduction in morbidity/mortality

Side effects:
• Accentuation of MI, CHF, edema (if started at high dose)
• Bradycardia
• Asthma/COPD precipitation
• Altered carbohydrate tolerance and lipid profile
• Rebound hypertension on withdrawal
• fluid retention
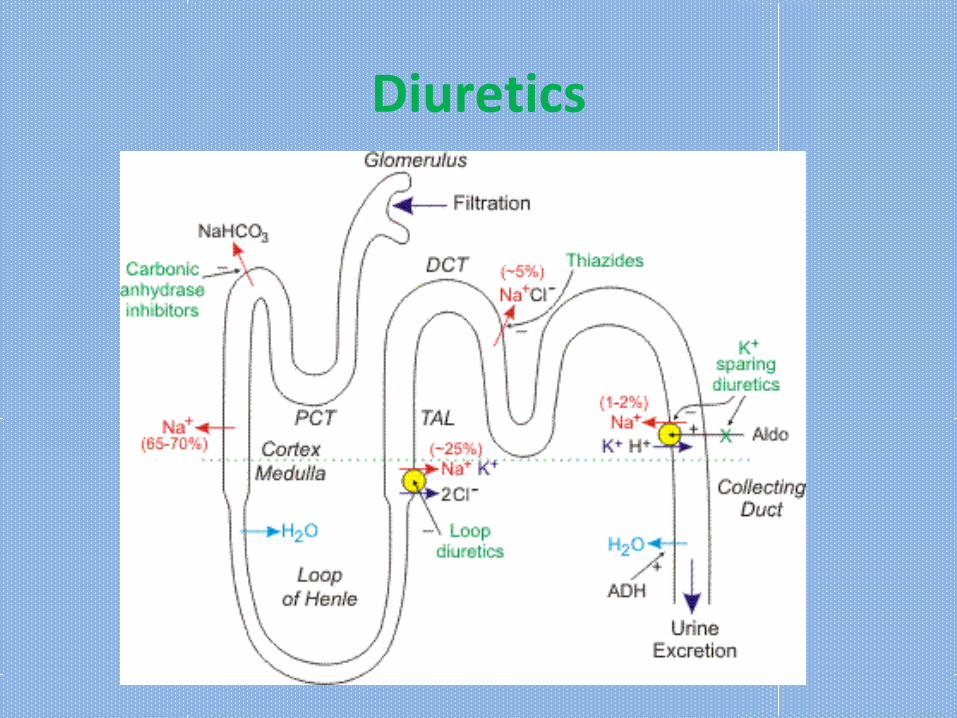
Diuretics

Loop Diuretics
Furosemide, Bumetanide• preferred in HF (symptomatic esp:edema)
• Effective diuresis-> ↓ ECF -> ↓ venous return -> ↓ preload
a) ↓ edema b) ↓ cardiac size(↑ CO)• Do not influence primary disease process
• s/e: Hypokalaemia: precipitate digitalis toxicity & arrhythmia
• T1/2 : furosemide: 1-2 hr, bumetanide: 60 mins
• Dose: furosemide: 20-80 mg OD, Bumetanide: 1-5 mg OD


Aldosterone antagonists
Spironolactone
• Dose: 12.5-25 mg/day
• Add on with ACEI & others in moderate-severe CHF
• Retard disease progression (Aldosterone: fibroblast proliferation and fibrotic changes in myocardium)
• Slow response
• Cx in renal failure (precipitate hyperkalemia)
• Eplerenone shows no gynaecomastia

Eplerenone
Search abt it

• With diuretcis. Reason a) Hypokalemia prevented
b) improve refractoriness of chronic diuretic use
c) also improves survival
• s/e: hyperkalemia, gynaecomastia
• In severe CHF: ACEI+ spironolactone+ digitalis: improves survival
Thiazides: Hydrochlorothiazide: used less frequently

Cardiac GlycosidesDigoxin• Source: Digitalis Lanata• Ix: Low output heart failure due to HT, IHD & arrhythmias
Dose:Oral route is preferred: 0.125-0.5mg/day.
1) Slow loading with 0.125-0.25 mg/day2) Rapid method with 0.5-0.75 mg every 8hrs for 1 day followed by 0.125-0.25
mg/day( rare)3) IV is seldom required
• Both are equally effective
• Given when ACEI & Diuretics fail to control symptoms
• Better results in HF with Atrial fibrillation

MOA• Raises free cytoplasmic Ca2+ -> ↑FOC -> ↑ C.O. &↓ Cardiac systole
• Opposes compensatory sympathetic activity and vagal stimulation: ↓ H.R.
Effects• No change or ↓ in oxygen requirement, ↓ heart size
• Protection of ventricles from atrial flutter or fibrillation
• ↓ in after load and preload
• Diuresis
• Bradycardia, improved myocardial circulation and sense of well being
Subside pulmonary congestion and edema

Raised free cytosolic Ca2+ is due to
1) Main: Reversible inhibition of Na+/K+ ATPase
2) Increase in Ca2+ permeability through voltage sensitive L type Ca2+ channels during plateau phase
3) Release of more Ca2+ from SR & mitochondria by activating Ryr (ryanodine) receptors
4) Inhibits SR- Ca2+ ATPase (reuptake channel)


DIGOXIN
Oral absorption(%)
75-90
Administration
Oral, iv
aVd (L/kg) 6-7
Protein binding
30
Plasma T1/2 38-40 hrs
Onset of action
½ hr
Metabolized (%)
20(liver)
Excretion Urine (unchanged)
• Small mortality benefit at plasma levels <1 ng/ml
• Preferred in conditions with dilated heart (helpful in restoring cardiac compensation?)
• Reduces hospitalization and deaths from progressive HF but increase in sudden death4
• Shows cumulative effects: full therapeutic effects after 4 x t ½: 6-7 days
• No effect on BP

Adverse effects from govind garg page 139
• Bradycardia, heart blocks. At toxic doses: extra systoles, pulsus bigeminus, ventricular fibrillation & fatal arrhythmia
• Monitor serum level: digoxin & K+ and ECG
• In severe toxicity- temporary cardiac pacemaker catheter +digoxin immune fab
• Use of DIGIBIND Fab fragment: 40 mg neutralizes 0.6 mg digoxin
• Others: GI upset, blurred vision & loss of color perception, hyperkalemia, gynaecomastiareduce dose
• Cx: Hypokalemia, children<10 yrs, elderly with renal or hepatic disease, MI, hypothyroidism, WPW syndrome and myocarditis, hypercalcaemia, hypomagnesemia, A-V block, renal failure, hypo-hyper thyroidism

A pt on chronic digoxin Rx develops ventricular arrhythmia.
Steps:• Withdraw digoxin• Add oral K supplements slowly & cautiously• Treat with lidocaine/B blocker• DOC: iv digibind ovine antidigoxin Fab fragments; No
immunological reaction due to lack of Fc.

Drug Interactions
ENHNACED digitalis toxicity
1)Loop diuretics, steroids
2) Amiodarone, quinidine, verapamil, tetracyclines, erythromycin
3) Catecholamine, Sch
DECREASED digitalis effects
1) Antacids, Sucralfate, Neomycin
2)Enzyme inducers
3) Hyperthyroidism
4) Cholestyramine

• ACEI -> raised digitalis toxicity• B blockers-> reduce av conduction• Verapamil-> raised toxicity• Nifedipine- safe• Diuretics ( hypokalemia)-> raised toxicity• Quinidine, amiodarone-> toxicity

• Cardiac-extracardiac se

Mx of side effects

Treatment of digitalis toxicity

Explain drug interaction
• Amiodarone/verapamil with digoxin

Vasodilators


Combination
• Given when ACEI are not tolerated or contraindicated
• Long term use can reduce damaging remodelling of the heart and prolong survival ( less than ACEI)

β agonists

Dobutamine
• β1 selective
• T1/2: 2 min. Steady state concentration achieved in 10 mins
• IV 5-10 μg/kg/min
Uses:• Short term management: acute HF• HF with MI or cardiac surgery
Adverse effects
• Precipitation of angina/MI (as it increases myocardial O2 demand)
• Tolerance due to repeated use
• Caution in atrial fibrillation (↑AV conduction) and hypertensives(↑ BP)

Dopamine
• In acute HF• HF with hypotension• Low C.O. heart failure with compromised renal function
Effects• ↑C.O. (β1 agonist)
• Renal & splanchanic vasodilatation (D1 agonist)
• Dose: 5-10 μg/kg/min
• Monitor BP, HR, urinary output

PDE Inhibitors
• Benefits is mostly from vasodilatation than positive inotropic effects
Inamrinone and Milrinone-PDE3 inhibitors
• Use in acute heart failure or severe exacerbations of chronic

Inamrinone
• T1/2- 2-4 hrs
• Action starts in 5 min and lasts for 2-3 hrs
• Dose: 0.5 mg/kg bolus full. by 5-10 μg/kg/min infusion
• s/e: thrombocytopenia, nausea, vomiting, arrhythmia, liver enzyme changes: withdrawn in some countries
Milrinone
• T1/2- 40-80 min
• 10 times more potent than inamrinone. Preferred
• Dose: 50ug/kg iv bolus foll by 0.4-1.0 ug/kg/min
• s/e: less thrombocytopenia and liver effect. Same arrhytmogenic potential, headache, tremors

Enoximone
• Congener of inamrinone• IV in acute heart failure• Better tolerated and improves physical quality of life (central stimulatory
effect of ↑c AMP)

Levosimendan
• Sensitizes troponin system to calcium & inhibits PDE• May be useful in HF• acutely decompensated congestive heart failure

Istaroxime4
• Investigational steroid derivative
MOA:
• Increases contractility by inhibiting Na+/K+ ATPase• Facilitates sequestration of Ca2+ by saroplasmic reticulum (may render
drug less arrhythmogenic than digoxin)
• In phase 2 clinical trial

NON-Inotropic agents

Vasoactive Peptides
• ↑BNP (Brain Natriuretic Peptide): diagnostic and prognostic marker in heart failure
• Rapid Measurement BNP →emergency diagnosis of heart failure
• released from the cardiac ventricles (response to increased wall tension)


Nesiritide
• Recombinant form of human BNP
• APPROVED for acute decompensated HF
MOA• ↓ arteriolar and venous tone (↑ cGMP in smooth muscle cells --
smooth muscle relaxation)
• Natriuresis (Inhibits Na+ absorption in collecting duct)

• Dose: 2μg/kg bolus followed by continuous IV infusion of 0.01-0.03 μg/kg/min
• T1/2- 18 min
• s/e- excessive hypotension, renal damage
• No dose adjustment in renal insufficiency
(?)
C/I: syst BP< 70

he short- and long-term morbidity and mortality in acute heart failure is still unacceptably high. There is an unmet need for new therapy options with new drugs with a new mode of action
Ularitide
• Recombinant peptide mimics activity of urodilatin
• Route of administration- IV
• Under Ix for acute heart failure
• Improve Cardiovascular parameter & promote diuresis without↓ creatinine clearance
• In phase 3

Vasopeptidase Inhibitors
MOA• ↑ANP & ↑BNP inhibition of neutral endopeptidases (enzyme
metabolizing natriuretic peptides)
• ↓Ang II- inhibition of ACE
Effects
Vasodilatation and Na+ & water excretion
↓
↓total peripheral resistance and BP
E.g.: Omapatrilat, Sampatrilat, Fasidopatrilat

Omapatrilat
• Orally active long acting inhibitor of NEP
Studies suggest:
• ↓BP in Hypertensive animal models and in patients
• ↑ cardiac functions in heart failure patients
Side effects: angioedema (3 times more than ACEI), cough, dizziness
Clinical status: in phase 3 trials
Ecadotril:

Vasopressin AntagonistsV1a : vasoconstrictionV2: antidiuretic
• Conivaptan
• V1a & V2 antagonist
• APPROVED for hyponatremia (SIADH)
• Potential use in heart failure: as ↓ peripheral resistance and ↓ dilutional hyponatremia
• T1/2: 5-12 hrs
• Dose: 20 mg loading IV over 30 min followed by 20 mg IV over 24 hrs
• Drug interactions present (CYP3A4 metabolism)
• s/e: infusion site reaction, headache, hypotension, pyrexia

Tolvaptan
• V2 antagonist
• Oral: 15-45 mg/day
• T1/2: 6-8 hrs
• APPROVED to treat hyponatremia (SIADH)
• Multiple drug interactions ( substrate and inhibitor of p-glycoprotein and CYP3 metabolism)
• Can cause rapid Na+ reduction & may prove fatal1)Start only in hospital setting2)Monitor sodium level

In heart failure clinical trials (patients of CHF with low ejection fraction)
Short term results:↓ body wt & ↓ dyspnoea
Long term results: ↓ body wt ( ↓edema)&↑Na+ conc (normalize Na+)
No effect on mortality & hospitalization
s/e: g I effects, hyperglycaemia, pyrexia, DVT, DIC, hemorrhage
Selective V1a antagonists
potential for raised TPR state like HT and HF

Renin inhibitor
Aliskiren• Recently approved for HT
• In clinical trial for HF: may be efficacy similar to ACEI
• Exerts beneficial effect on myocardial remodeling by ↓ left ventricular mass in HT patients--Showing salutary effects on CVS--- Trial done on CHF patients
• In a trial 3 Aliskiren with β antagonist and ACEI in CHF did show no hyperkalemia and hypotension and ↓ plasma BNP levels
↓
May improve symptoms and functional capacity in CHF

Endothelin antagonists
Bosentan• Oral, non –selective • Approved for use in pts with pulmonary hypertension.• Not shown efficacy in heart failure• Failed to show benefit in mortality and morbidity
Tezosentan • nonselective ET receptor antagonist
Darunsentan

Adrenomedullin
• Potent vasodilator peptide
• Experimental therapeutic intervention in rats by transfer of the AM gene or of recombinant AM inhibit the progression of cardiac hypertrophy and remodeling
• Promotes maintenance or improvement in renal function
• Counter the activation or actions of vasoconstricting and sodium-retaining
hormone systems
• Potential therapeutic agents for Heart failure.

Steroids in HF

Statins

Allopurinol

Superscripts..
1- sharma& sharma
2-Tripathi
3-G&G
4-katzung






























