Embed Size (px)
Citation preview

9/9/2014
Pharmacoepidemiology
PRESENTATION BY:
AISHA SIDDIQUI
M.PHARM. 1ST Yr.
Dept. of pharmacology

Contents
Definitions.
Introduction.
Evolution of PE.
Types of epidemiology.
Observational VS Experimental studies.
Purpose of descriptive PE.
PE study designs.
Drug utilization study.
Special application of PE.
Reports.

Definitions
“The study of the use and effects of medications in large numbers of people”
Strom

“The application of epidemiologic knowledge, methods, and reasoning to the study of the effects (beneficial and adverse) and use of drugs in human populations.”
Porta and Hartzema

“The study of drugs as determinants of health and disease in the general unselected population.”
Spitzer

What Is Pharmacoepidemiology?
• All drugs have adverse effects. Pharmacoepidemiology will never succeed in preventing them. It can only detect them, hopefully early, and thereby educate health care providers and public, which will lead to better medication use.

• The net results of increased activity in Pharmacoepidemiology will be better for industry and Academia but most importantly, for public’s health.
• Pharmacoepidemilogy can minimize its adverse public health impact by detecting it early. At the same time, it can improve the use of drugs that have genuine role, protecting against the loss of useful drugs.

Introduction
• In recent decades, modern medicine has been blessed with a pharmaceutical armamentarium that is much more powerful than it had before. Although this has given health care providers the ability to provide better medical care for their patients, it has also resulted in the ability to do much greater harm.

• It has also generated an enormous number of product liability suits against pharmaceutical manufacturers, some appropriate and others inappropriate..
• In fact, the history of drug regulation parallels the history of major adverse drug reaction “disasters”. Each change in pharmaceutical law was a political reaction to an epidemic of adverse drug reactions.
Evolution of pharmacoepidemiology.
Recent data indicate that 100000 Americans die each
year from Adverse Drug Reactions, and 1.5 million US
hospitalizations each year result from Adverse Drug
Reactions; yet, 20-70% of Adverse Drug Reactions may
be preventable. The harm that drugs can cause has led
to the development of the field of
pharmacoepidemiology.

Clinical pharmacology
Pharmacoepidemiology
Epidemiology

The joining of the fields of clinical pharmacology and epidemiology has resulted in the development of a new field:
pharmacoepidemiology, the study of the use of and the effects of drugs in large numbers of people.

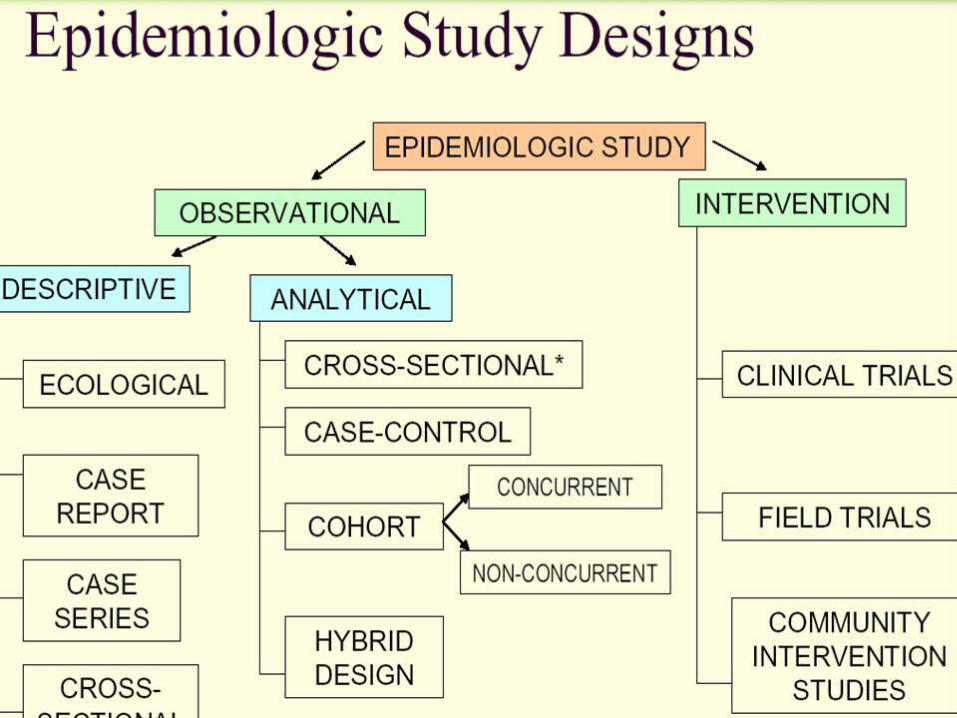
Types:
Epidemiology is defined as the study of the
distribution and resulting determinants of
diseases on populations.
Epidemiological studies can be divided into two
main types:
1. Observational Study
2. Intervention Study
Observational VS Experimental studies
•Observational studies , Allow nature to take
its cause; the investigator measures but does
not intervene.
•Descriptive study: focuses on the description
of the occurrence of a disease in a
population.
•Analytical study analyses relationships between health status and other variables.

Observational VS Experimental studies
•Experimental or interventional studies: involve
an active attempt to change a disease
determinant(e.g an exposure or a behaviour) or
the progress of a disaese (through treatment)
•The studies are based on a group which has had
the experience compared with control group
which has not had the experience.

Purpose of descriptive epidemiology
•To generate hypothesis
•To permit evaluation of trends in health &
disease and comparisons among countries and
subgroups within countries.
•To provide a basis for planning, provision and
evaluation of health services
•To identify problems to be studied by
analytical methods and to suggest areas that
may be fruitful for investigation.
Case studies(Case series)
•Case reports:documents unusual medical occurrence
and can represent the first clues to the formulation of
hypothesis, generally report a new or unique findings and previous undescribed disease.
Eg; Zappacosta presented a case report of a patient
treated with minoxidil that was discovered to
stimulate the hair growth. Subsequently a topical
formulation of minoxidil was developed to take
advantage of that effect
Case series: collection of individual case reports which may occur within a fairly short time, and experience of a group of patients with similar diagnosis.
Eg: Krishnamoorthy and king reported on the adverse effects associated with the use of olanzapine in 5 children with severe behavioural problems.Adverse events includes: wt. gain(3/5 children)sedation(2/5 children) and akathisia( 2/5 children).

Case Series
AdvantagesUseful for hypothesis generation
Informative for very rare disease with few
established risk factors
Usually of short duration.
DisadvantagesCannot study cause and effect
relationships
Cannot assess disease frequency
Cross-sectional study• It is also called epidemiologic study or prevalence
study.
• It analyses (describes)data collected on a group of subjects at one point in time rather than over a period of time. i.e. they survey exposure and disease at a single point in time.
• Both exposure and outcome variables are been evaluated at the same point in time(without any inbuilt directionality).
• Most sophisticated descriptive study.
• It answers the question “WHAT IS HAPPENING RIGHT NOW?”

Question: “what is happening?”no direction of inquiry
subjectsWith outcome
Without outcome
endonset time
Cross-sectional studies
• Eg: cross-sectional studies was published by Dua and colleagues, who examined inappropriate sale of antibiotic use in pharmacies in Nagpur.
Such studies can identify problem areas and suggest where remedial action should be directed.

Cross-sectional studies
ADV
• Best for determining the status
(prevalence)
• Quick
• Relatively inexpensive
DISADV
• Only a snapshot at a time leading to a misinformation
• Response rate may be low ,with result not representative of the population

Correlational study designs
• A study comparing incidence/prevalence of one event against another on a global scale
• Measures that represent characteristics of entire populations are used to describe the disease in relation to some factor of interest (such as age, calendar time, food consumption, drug use and utilization of health services)

Correlational study designs
ADV
• Compares events among nations.
DISADV
• Doesn’t compare individuals, so it might lead to overgeneralization.

Analytical studies
Two basic designs:
• Case – control or retrospective study
• Cohort or prospective
• NOTE
• There must be a comparison group
• No control No conclusion(NCNC)
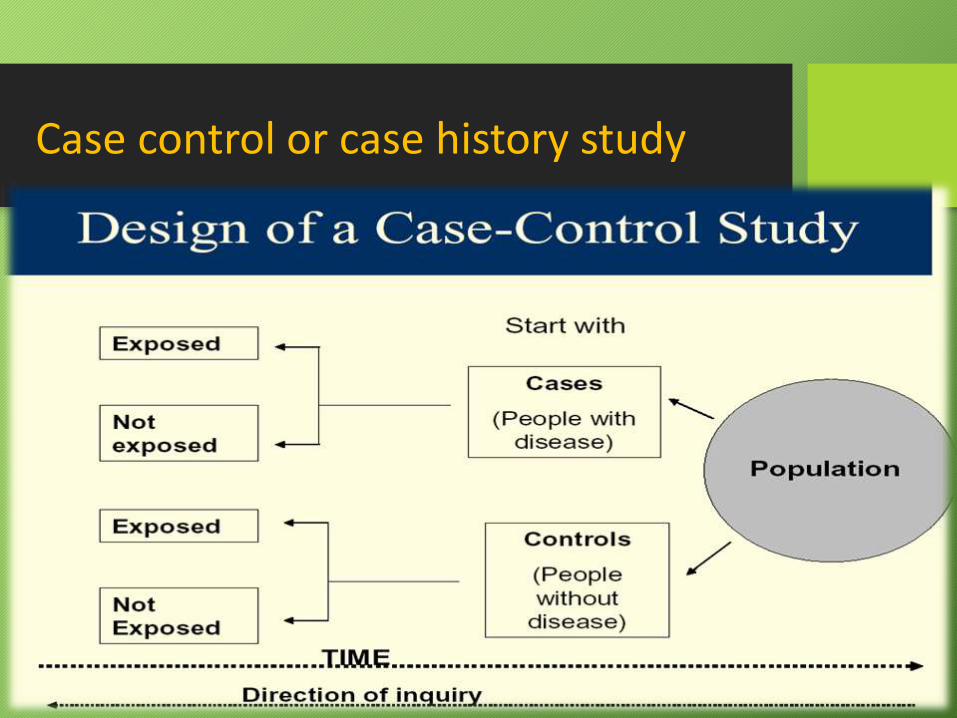
Case control or case history study

Advantages of case control
• It is relatively easy to carry out.
• It is also rapid and inexpensive.
• It requires comparatively few subjects.
• It can assist one in studying different etiological factors.
• One does not need an ethical clearance.
• There is no risk to the subject .
Disadvantages of case control
• It introduces bias
• To select an appropriate control could be difficult
• It may be difficult to distinguish between the cause of a disease and an associated factor

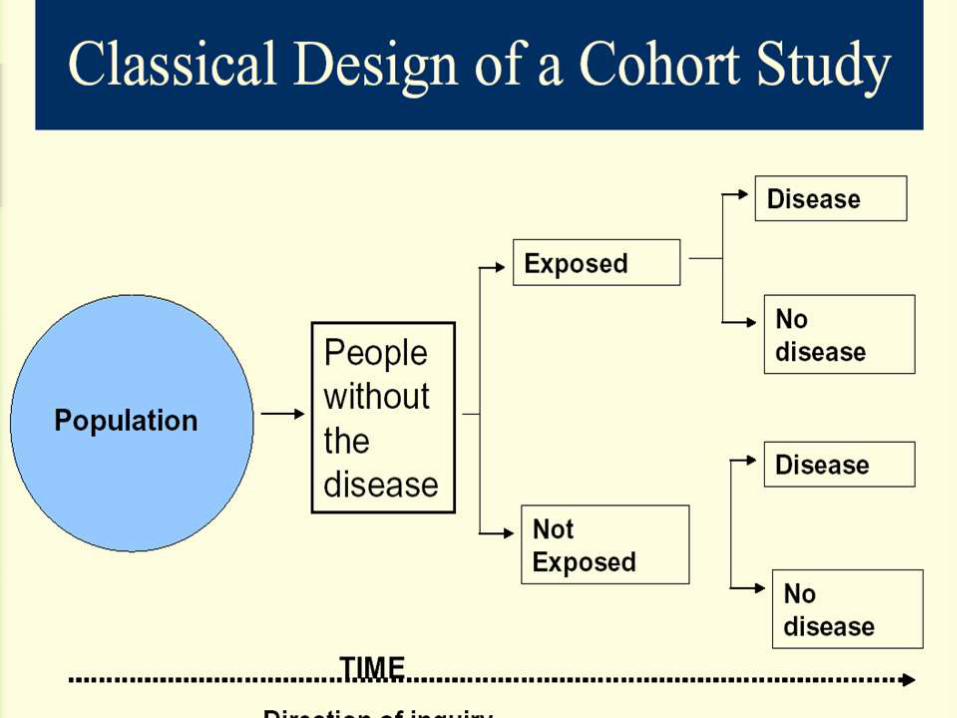
Cohort study
• A cohort is a group of people who have something in common and remain part of a group over an extended time
• A group of people exposed to a suspected etiological agent are compared with a matched control who have not been similarly exposed. Subject selected on the basis of exposure [a etiological factor; cigarette smoking]
• Follow-up over a period to compare the outcome
• Also a longitudinal study or prospective study

Advantages Of cohort study
• There is no bias
• The risk can be calculated bcos the incidence can be calculated
• It is effective for studying rare exposures
• It allows the study of the natural history of the disease
• It assists in determining the temporal relationship between the etiological factor & the disease
Disadvantages of cohort study
• It takes a long time
• It is expensive
• Large no of subjects are needed
• There could be changes in the standard methods or diagnostic criteria

Experimental studies
• Studies in which 1 group is deliberately subjected to an experience compared with a control group with no similar experience
• The gold standard in medicine because it proves causality
• Can be controlled or uncontrolled
Uncontrolled experimental studies
• Intervention is not compared with a control
• The aim is to confirm that the Intervention made a difference
Controlled experimental studies
• In this study, a drug or procedure is compared to:
1. Another drug
2. Procedure
3. Placebo
4. Previously accepted tx
• The aim is to prove the difference due to tx
Controlled experimental studies
• Control could be:
• Blind trial-single or double
A. METHODOLOGY
1. Concurrent or parallel: randomized or non-randomized(quasi)
2. Sequential control: self controlled or cross over
3. External control

Study population
1. Clinical trials
2. Field trials
3. Community trials

Experimental studies
ADV
• Best study type
• Greatest proove of causality
• Gold standard for other design
• Least bias
• Proves best tx or procedure efficacy
DISADV
• Greatest expense
• Long duration
• Unproven facts adopted by community can hinder study acceptance
Drug utilization study:
• Drug utilization studies aim to evaluate factors related to the prescribing, dispensing, administering and taking of medication, and its associated events (either beneficial or adverse).
• Since the early 1960’s the interest in Drug Utilization Studies has been increasing, first with market-only purposes, then for evaluating the quality of medical prescription and comparing patterns of use of specific drugs.

• The increasing importance of drug utilization studies as a valuable investigation resource in pharmacoepidemiology has been bridging it with other health related areas, such as public health, pharmacovigilance, pharmacoeconomics, eco-pharmacovigilance or pharmacogenetics.
• Drug utilization research is thus an essential part of pharmacoepidemiology as it describes the extent, nature and determinants of drug exposure. In common use, the distinction between these two terms has become less sharp, and they are sometimes used interchangeably.
Drug utilization research and pharmacoepidemiology may provide insights into the following aspects of drug use and drug prescribing:
• Pattern of use: extent and profiles of drug use and trends in drug use and costs over time.
• Quality of use: audits comparing actual use to national and regional prescription guidelines or local drug formularies. Quality indices of drug use may include the choice of drug (compliance to recommended assortment), drug cost (compliance to budgetary recommendations), drug dosage (awareness of inter-individual variations in dose requirements and age dependence), drug interaction awareness, ADR awareness, proportion of patients being aware of/unaware of the cost/benefit of the treatment, etc.
• Determinants of use: user characteristics (e.g. socio-demographic parameters, attitude towards drugs), prescriber characteristics (e.g. specialty, education and factors influencing therapeutic decisions), and drug characteristics (e.g. therapeutic properties, affordability)
• Outcomes of use: health outcomes (benefits and adverse effects) and economic consequences.

Special applications of Pharmacoepidemiology
• Studies of Drug Utilization
•Evaluating and improving physician prescribing
•Drug Utilization Review
• Special methodologic issues in PE studies of Vaccine Study
•PE studies of Devices
• Studies of Drug induced birth defects
•PE and Risk management
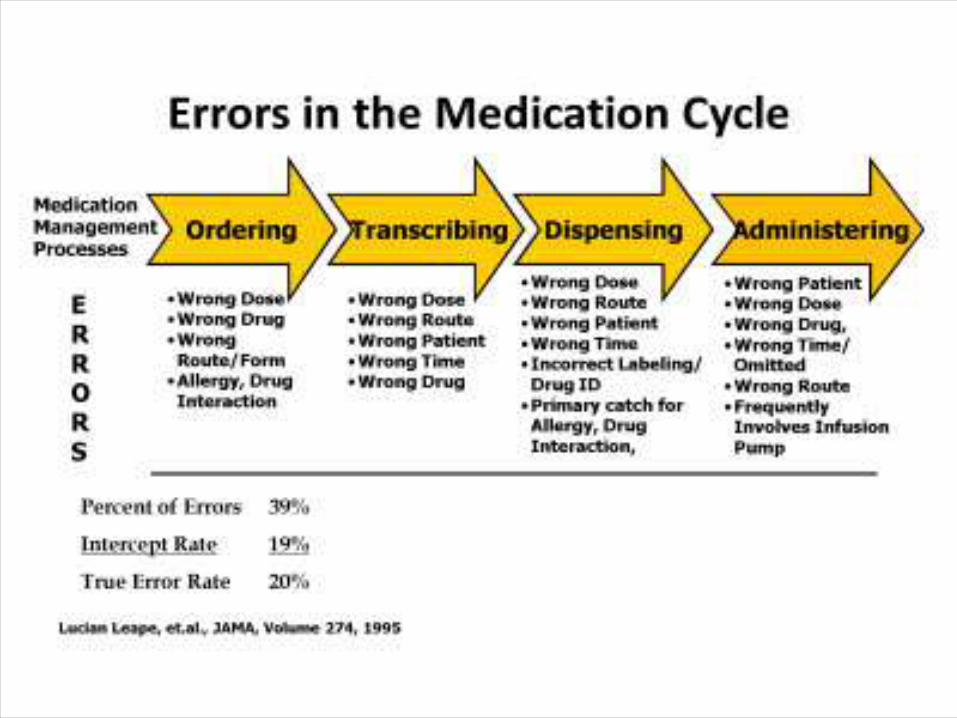
•Use of PE to study Medication Errors
•Hospital PE.

REPORT 1-Novel anticoagulants given to 60% of newly diagnosed AF patients.
Novel oral anticoagulants introduced since October 2010 have been adopted into clinical practice rapidly, and within 2.5 years were prescribed for more than 60% of patients with newly diagnosed atrial fibrillation, according to a report published online May 20 in the American Journal of Medicine. the new drugs are being prescribed for a different patient population from that indicated by the clinical trials on which Food and Drug Administration (FDA) approval was based. Specifically, dabigatran, rivaroxaban, and apixaban are selectively prescribed for younger, healthier men who have high

incomes and reside in wealthier communities, reported Dr. Nihar R. Desai of the division of pharmacoepidemiology and pharmacoeconomics, Brigham and Women’s Hospital and Harvard Medical School, Boston, and his associates. In what they described as the first study to evaluate real-world use of all novel anticoagulants, researchers found that the rapid uptake of the drugs as first-line therapy for atrial fibrillation (AF) was accompanied by a marked decline in the use of warfarin. The difference in total costs between the generic warfarin and the proprietary dabigatran, rivaroxaban, or apixaban totaled $900 per patient during the first 6 months alone, which "translates into billions of dollars at the national level."

The researchers analyzed nationwide medical and prescription claims data for 6,893 adults covered by Aetna who had newly diagnosed nonvalvular AF and were prescribed an oral anticoagulant between October 2010 and June 2013. The direct thrombin inhibitor dabigatran was approved in October 2010, and the factor Xa inhibitors rivaroxaban and apixaban were approved in November 2011 and December 2012During the study period, these patients filled 45,472 prescriptions for oral anticoagulants: 57.7% for warfarin, 32.8% for dabigatran, 9.3% for rivaroxaban, and 0.1% for apixaban. Within 1 year of appearing on the market, dabigatran was equally likely to be prescribed as warfarin was for new AF patients. Its use as a first-line therapy..
REPORT 2- A case-control study design was used. A new prescription of an antidiabetic medication was used to identify new cases of diabetes mellitus.
Odds ratios were calculated for exposure to second-generation antipsychotics (clozapine, risperidone, olanzapine, quetiapine, and multiple second-generation antipsychotics) compared with exposure to first-generation antipsychotics. Cases and controls were identified by using a database that contained drug prescription information from the inpatient facilities that were operated by the New York State Office of Mental Health. Data from January 1, 2000, to December 31, 2002, were examined. Among 13,611 unique patients who received antipsychotics, 8,461 met entry criteria of being hospitalized for at least 60 days and not having an antidiabetic medication prescribed in the past. A total of 181 of these inpatients received prescriptions for an antidiabetic

medication at least 30 days after their admission. Eight controls (N=1,448) for each case (N=181) were matched by calendar year, length of observation period, race, age group, and diagnosis, giving a total sample of 1,629 patients.RESULTS: Statistically significant elevations in risk were seen among patients who received more than one second-generation antipsychotic or clozapine or quetiapine, compared with patients who received first-generation antipsychotics alone. Although not statistically significant, odds ratios for olanzapine and risperidone were also elevated.Conditional logistic regression adjusting for gender and age did not change the results.

Crude odds ratios (ORs) for receiving a new prescription of an antidiabetic agent were calculated, and 95 percent confidence intervals (CIs) were determined

Conclusion:
Exposure to multiple second-generation antipsychotics or clozapine or quetiapine significantly increased the risk of treatment-emergent diabetes mellitus.

References
1-Parthasarthi, “A Textbook Of Clinical Pharmacy Practice”, Edition-2001, page no-466-482.
2-Edward Ralph, Santoso Budiono, J.Van Boxtel Chris, “Drugs Benefits And Risks:International Textbook of Clinical Pharmacology” Edition-2008, publishers-John Wiley & sons, LTD.
3-Koller E, Schneider B, Bennett K, et al: Clozapine-associated diabetes. American Journal of Medicine 111:716—723, 2001
4-http://ps.psychiatryonline.org/article.aspx?articleid=89028






























