Embed Size (px)
Citation preview

ParamyxoviridiaeDr.T.V.Rao MD

Myxovirus
• Classified into
1 Influenza virus 2 Parainluenza virus
A Mumps virus
B Parainluenza virus
C Measles virus
D Rspiratory syncitical virus
Paramyxoviridiae• Looks similar to Orthomyxoviruses,• Larger in size, More pleomorphic.• Spherical in shape 100 to 300 nm• Some times appear as filamentous,Gaint forms
are present.• But contains only single stranded RNA.• Do not contain segmented RNA like
Orthomyxoviruses, Antigenic variation absent.• Reassrtment like Influenzae viruses – ABSENT.
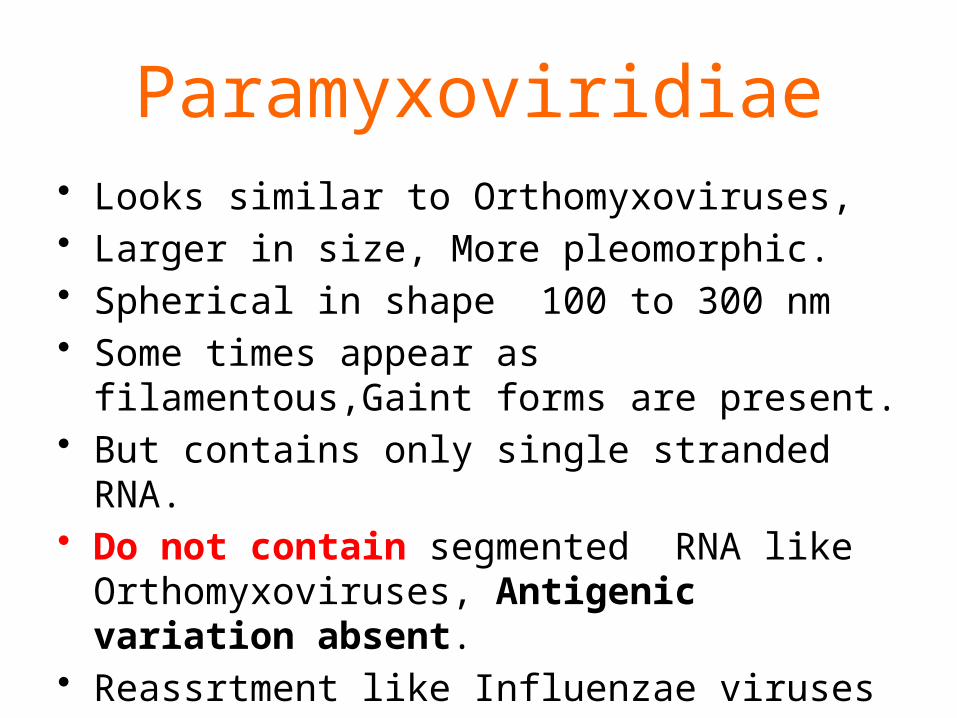
ORTHOMYXO / PARAMYXOViruses
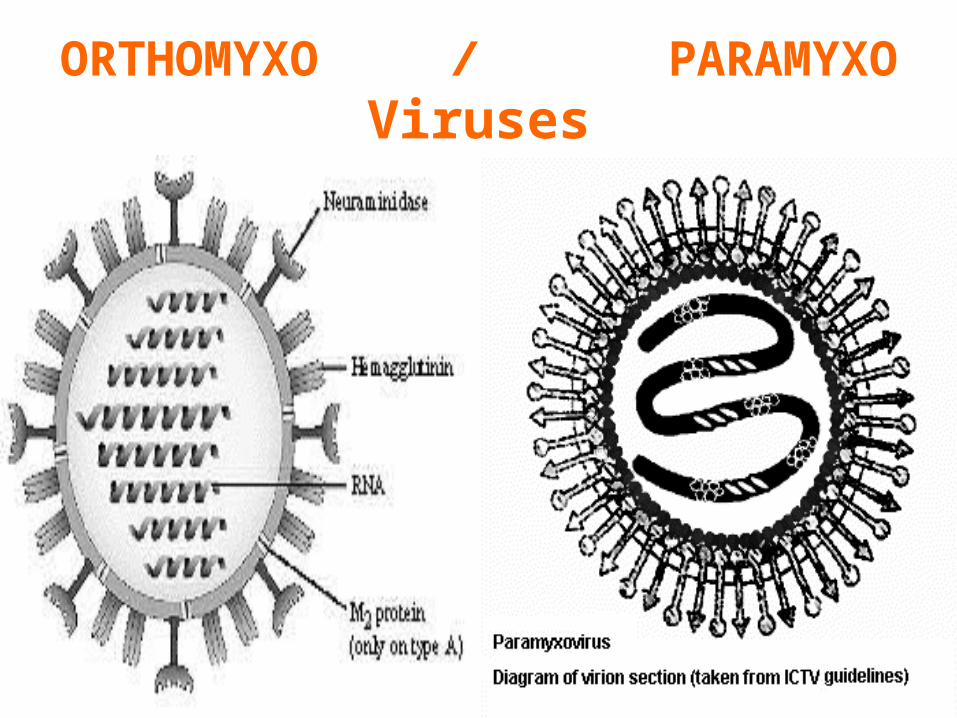
Paramyxovirus
Most Important Diseases.
1 Measles,
2 Mumps,
3 Respiratory Syncytial viruses.
4 Parainluenza viruses.

How Differs from Orthomyxoviruses
• Do not undergo Gentic Recombination, and Antigenic Variation.
All are Antigenically STABLE

Family – Paramyxoviridae.
Divided into – Rubella Virus.
Para InfluenzaVirus.
Morbilli virus.
Pneumo virus.
MUMPS• Mumps is an acute viral infection
of the paramyxoviruses family. As its alternative name (infectious parotits) suggests, the infection is characterized by swelling more commonly bilateral than unilateral of the parotid salivary glands.
Mumps belongs to Parmyxoviridae
• Viruses in the family Parmyxoviridae are classified in two subfamilies, Paramyxovirinae and Pneumovirinae. The latter subfamily contains two genera, Pneumovirus and Metapneumovirus.
MUMPS HIPPOCRATES 5th
Century BC
A Disease of Children,
Non Suppurative Enlargement of Parotid Gland.
1934 – Good Pasture/ Johnson
Incubation Period
• The incubation period is 14-21 days and is communicable from 6 days before to 9 days after facial swelling is apparent. It can lead to brain inflammation, deafness or sterility
Mumps belongs to Parmyxoviridae
• Looks similar to Orthomyxovirus,• Larger in size, More Plemomorphic.• Spherical in shape 100 to 300 nm• Some times appear as filamentous,Gaint forms
are present.• But contains only single stranded RNA.• Do not contain segmented RNA like
Orthomyxoviruses,Antigenic variation absent.• Reassortments like Influenzae viruses –
ABSENT.
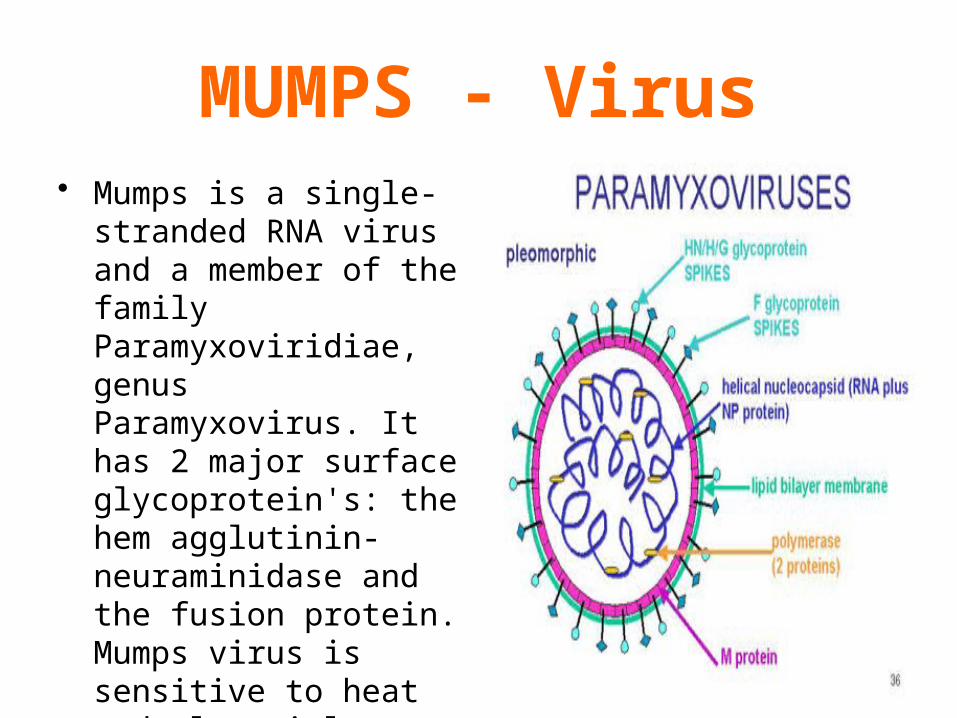
MUMPS - Virus• Mumps is a single-
stranded RNA virus and a member of the family Paramyxoviridiae, genus Paramyxovirus. It has 2 major surface glycoprotein's: the hem agglutinin-neuraminidase and the fusion protein. Mumps virus is sensitive to heat and ultraviolet light

Properties of MUMPS virus.
• Posses HN and F properties.
• Growth in Chick Embryos, in the Amniotic cavity, Adopts in allantoic cavity,
• Cell cultures – Primary Monkey kidney,
• Typical Paramyxoviruses,
produce cytopathic effects.

Mumps Virus
• Paramyxoviruses
• RNA virus
• One antigenic type
• Rapidly inactivated by chemical agents, heat and ultraviolet light
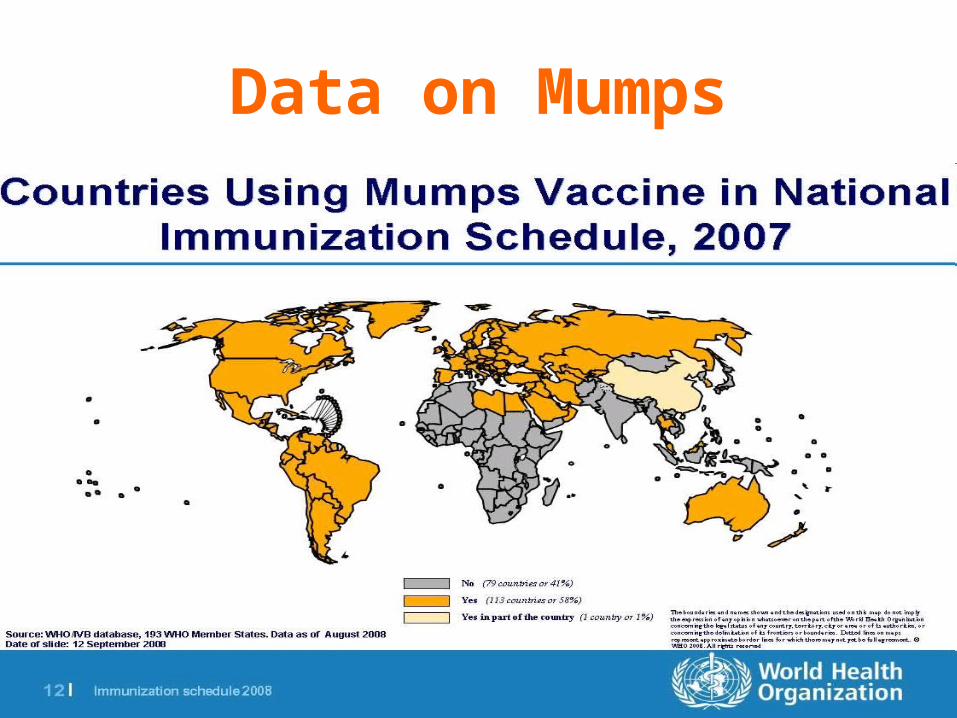
Data on Mumps
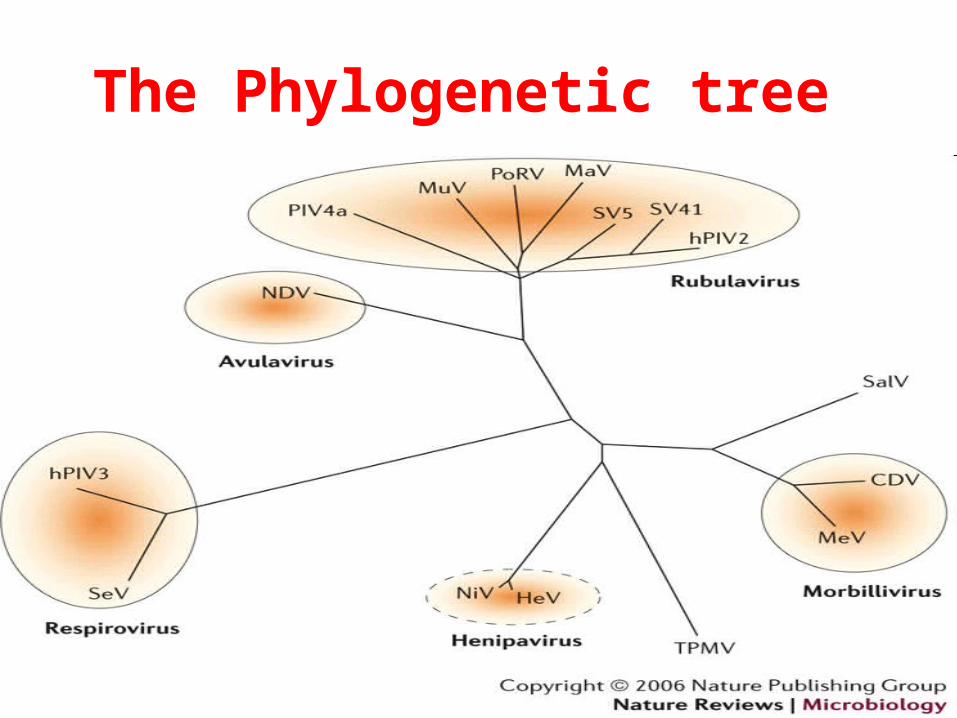
The Phylogenetic tree
Properties of MUMPS virus.
• Typical Paramyxovirus,• Posses HN and F properties.• Growth in Chick Embryos, in the Amniotic
cavity,Adopts in allantoic cavity,• Cell cultures – Primary Monkey kidney,
Produce cytopathic effects.
Mumps
• Mumps or epidemic parotitis is a viral disease of the human species, caused by the mumps virus. Prior to the development of vaccination and the introduction of a vaccine, it was a common childhood disease worldwide, and is still a significant threat to health in the Developing World

Mumps Virus• Paramyxoviruses
• RNA virus
• One antigenic type
• Rapidly inactivated by chemical agents, heat and ultraviolet light

Involvement of Salivary Glands
• Painful swelling of the salivary glands (classically the parotid gland is the most typical presentation) Painful testicular swelling (orchitis) and rash may also occur

Involvement of Parotid Gland a Major Manifestation
• Swelling of the salivary glands follows these symptoms. Swelling of the glands near the jaw line below the ears may give you "chipmunk cheeks
Mumbling speech - Mumps
• Name "mumps" comes from an old word for "lump" or an old word for "mumble."
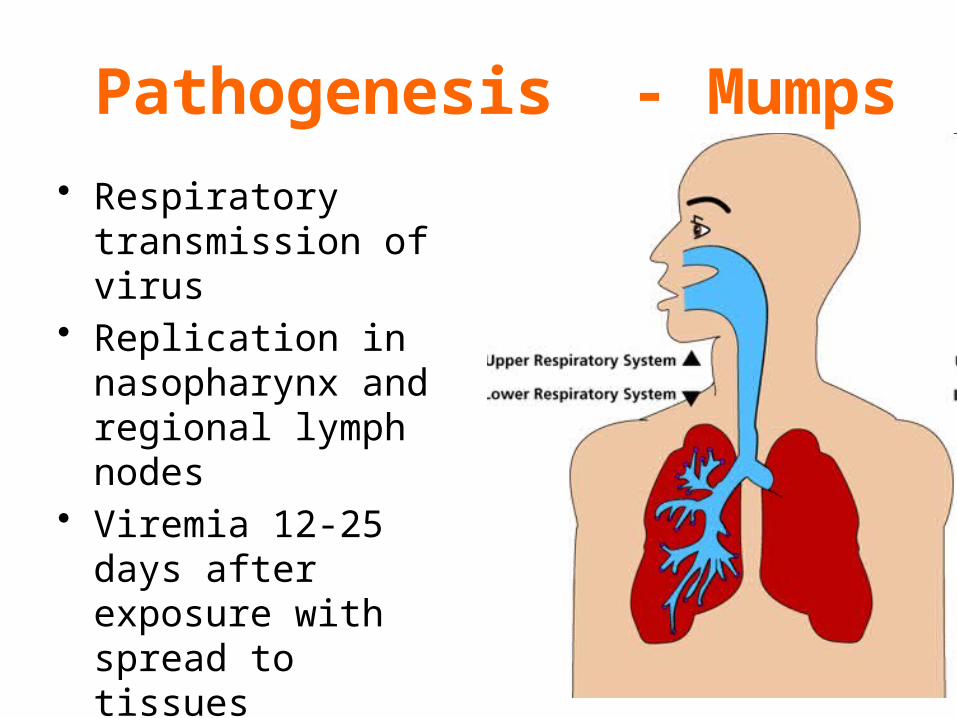
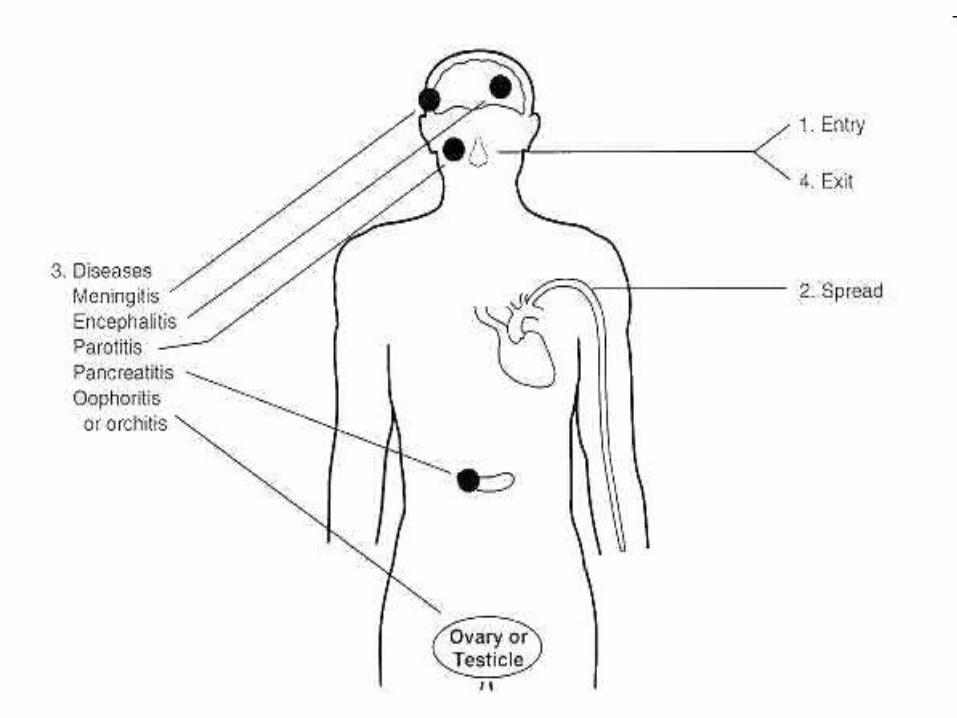
Pathogenesis - Mumps
• Respiratory transmission of virus
• Replication in nasopharynx and regional lymph nodes
• Viremia 12-25 days after exposure with spread to tissues
• Multiple tissues infected during viremia
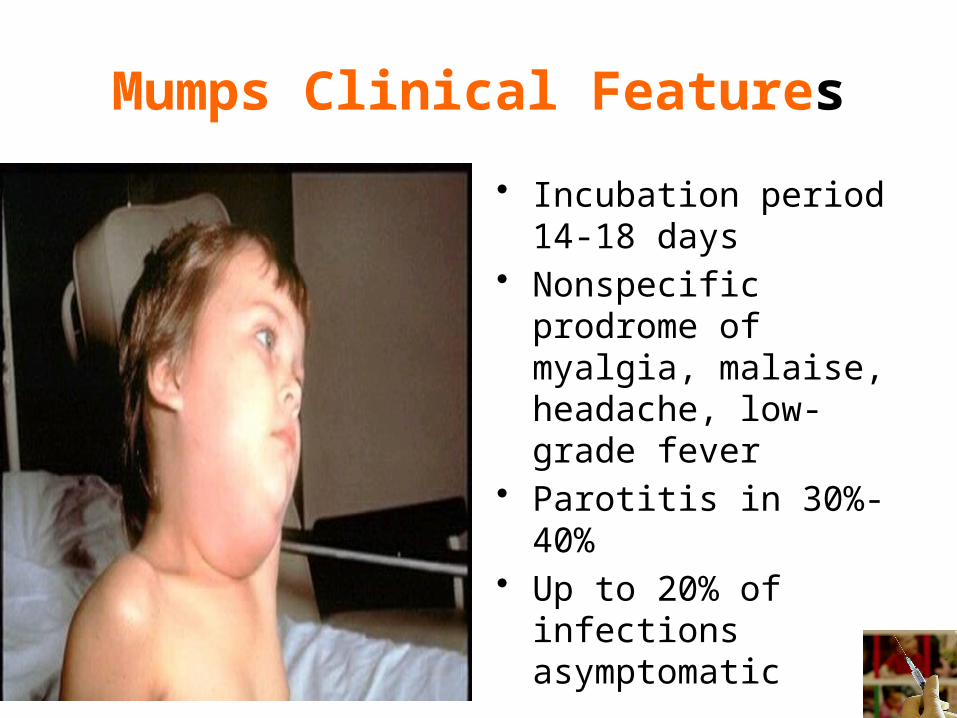
Mumps Clinical Features
• Incubation period 14-18 days
• Nonspecific prodrome of myalgia, malaise, headache, low-grade fever
• Parotitis in 30%-40%• Up to 20% of infections
asymptomatic
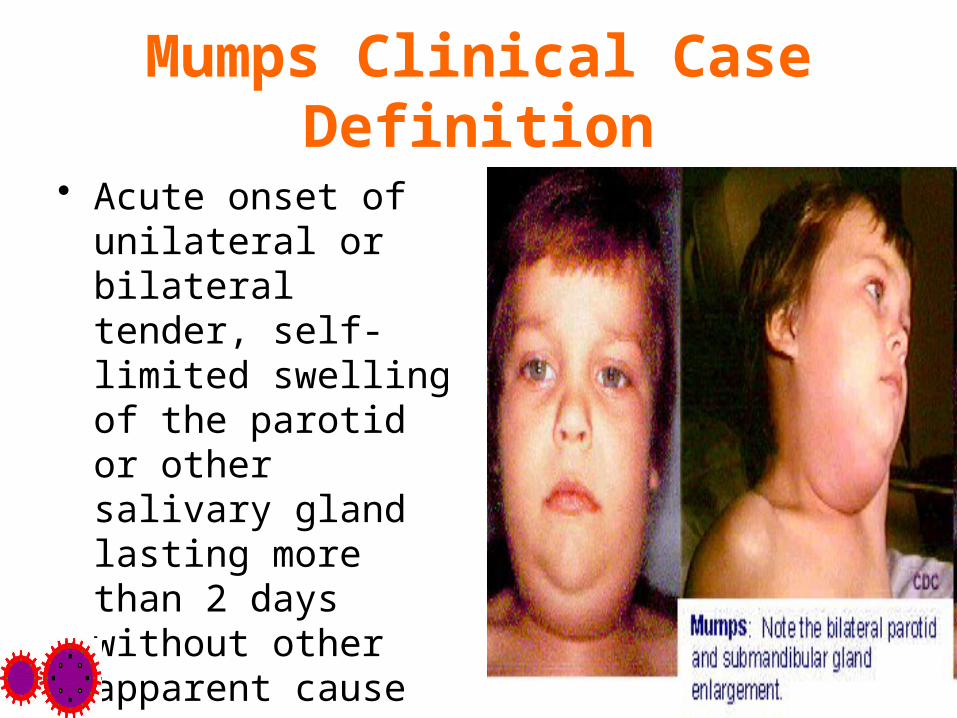
Mumps Clinical Case Definition
• Acute onset of unilateral or bilateral tender, self-limited swelling of the parotid or other salivary gland lasting more than 2 days without other apparent cause
Clinical Features MUMPS• Inhalation / Conjunctiva.• Replicates in URT Cervical Lymphnodes.• Blood stream to other organs• Incubation period 12- 25 days.• Manifest with Parotid swelling Unilateral or Bilateral.Fever , Local pain at parotid region and
Tenderness.Subsides In a Week.

Immunity• Antibodies are
produced against the S and V surface antigens..
• Mumps rare before 6 months of age.

Definition of Mumps Immunity
• Documentation of adequate vaccination
• Serologic evidence of mumps immunity
• Birth before 1957• Documentation of physician-
diagnosed mumps in the past

Complication with MUMPS.
• Orchitis. This inflammatory condition causes swelling of one or both testicles. Orchitis is painful.
• Pancreatitis.. • Encephalitis. A viral infection, such as
mumps, can lead to inflammation of the brain (encephalitis). Although it's serious, encephalitis is a rare complication of mumps.
Meingoencephalitis,
• In clinically diagnosed Meingoencephalitis, a CSF mononuclear pleocytosis occurs, as does normal glucose, although hypoglycorrhachia has been reported. The mumps virus may be isolated from CSF early in the illness. Mumps Meingoencephalitis carries a good prognosis and is usually associated with an uneventful recovery.
Complication with MUMPS.
• Meningitis. Meningitis is infection and inflammation of the membranes and fluid surrounding your brain and spinal cord.
• Inflammation of the ovaries. Pain in the lower abdomen in women may be a symptom of this problem. Fertility doesn't seem to be affected.
• Hearing loss.• Miscarriages.
Laboratory Diagnosis• No Laboratory confirmation needed.• Atypical infection needs laboratory Diagnosis.• Virus isolated from Saliva Urine CSF.Culturing in Human amnion, He la cells.Immunoflorecence Methods. Isolation in Chick
Embryos ELISA, Complement fixation tests,

Mumps Laboratory Diagnosis
• Isolation of mumps virus• Detection of mumps antigen by
PCR• Serologic testing
–positive IgM antibody–significant increase in IgG antibody
between acute and convalescent specimens
CDC recommends• CDC recommends
that a blood specimen and buccal /oral swab be collected from all patients with clinical features compatible with mumps.
• Recommendations stands mainly for epidemiological surveys

Vaccination• Live attenuated
vaccine
Jernyl Lynn Strain
Grown in chick embryo fibroblasts
Vaccine as MMR vaccine
A single dose protects for 10 years.

Mumps (MMR) Vaccine Indications
• One dose (as MMR) for preschool-age children 12 months of age and older and persons born during or after 1957 not at high risk of mumps exposure
Need for second dose• Second dose (as MMR) for school-age
children and adults at high risk of mumps exposure (i.e., healthcare personnel, international travelers and students at post-high school educational institutions
Passive immunization against mumps
– Immune globulin ineffective for post exposure prophylaxis• does not prevent disease or reduce
complications
–Transplacental maternal antibody appears to protect infants for first year of life

Epidemiology• Endemic – Prevalence all over the world• Immunization . Reduced the incidence.• Epidemics in children between 5-15.• No carriers.• Spread by Direct Contact• Saliva and urine are infective.• One Attack produces life time Immunity.
MMR VaccineContraindications and Precautions
• Severe allergic reaction to vaccine component or following a prior dose
• Pregnancy• Immunosuppression• Moderate or severe acute illness
of other etiologies

MMR Vaccine and Autism• There is no scientific evidence that the
risk of autism is higher among children who receive measles or MMR vaccine than among unvaccinated children
“The evidence favors a rejection of a causal relationship at the population level between MMR vaccine and autism spectrum disorders (ASD).”
- Institute of Medicine, April 2001

MMR combined vaccine is beneficial than separate component vaccines
• Separate administration of measles, mumps, and rubella vaccines to children provides no benefit over administration of the combination MMR vaccine and could result in delays in immunization.
Paediatricians need to work with families to ensure that children are protected early in the second year of life from these preventable diseases.

Mumps Vaccine and HIV Infection
• MMR recommended for persons with asymptomatic and mildly symptomatic HIV infection
• NOT recommended for those with evidence of severe immuno- suppression
• HIV testing before vaccination is not recommended

Mumps control:• Mumps control: The control of mumps can be
achieved through high routine coverage with an effective mumps-containing vaccine administered at 12–18 months of age. Children immunized with most mumps vaccines at the age of 12 months or older have excellent serological response rates. Programmes should aim at infant coverage of more than 90%. Low immunization coverage may reduce the number of cases in infants but fails to interrupt circulation of the mumps virus in the community.
Parainluenza virus

Parainluenza virus causes Respiratory infection in young
• They are the second most common cause of lower respiratory tract infection in younger children. Together, the Parainfluenza viruses cause ~75% of the cases of Croup.
• Repeated infection throughout the life of the host is not uncommon. Symptoms of later breakouts include upper respiratory tract illness as in a cold and sore throat. The incubation period of all four serotypes is 1 to 7 days.
Virus Properties.• 150-300 nm in size.• Envelop Two Glycoprotein • G protein attaches to cell surfaces,• F protein causes cell to cell fusion.• No Hemagglutinins or Neuraminidase
activity.• Grows in Human cell cultures He la and
He p2.

Para Influenza Viruses types
• Four Types are present.
• Type 1 Sendai Virus • Type 2 Acute Laryngo
tracheo bronchitis.• Type 3 Respiratory
infection in children• Type 4 Respiratory
infection.
ETIOLOGY:
• Parainfluenza viruses are enveloped RNA viruses classified as paramyxoviruses. Four antigenically distinct types—1, 2, 3, and 4 (with 2 subtypes, 4A and 4B)—have
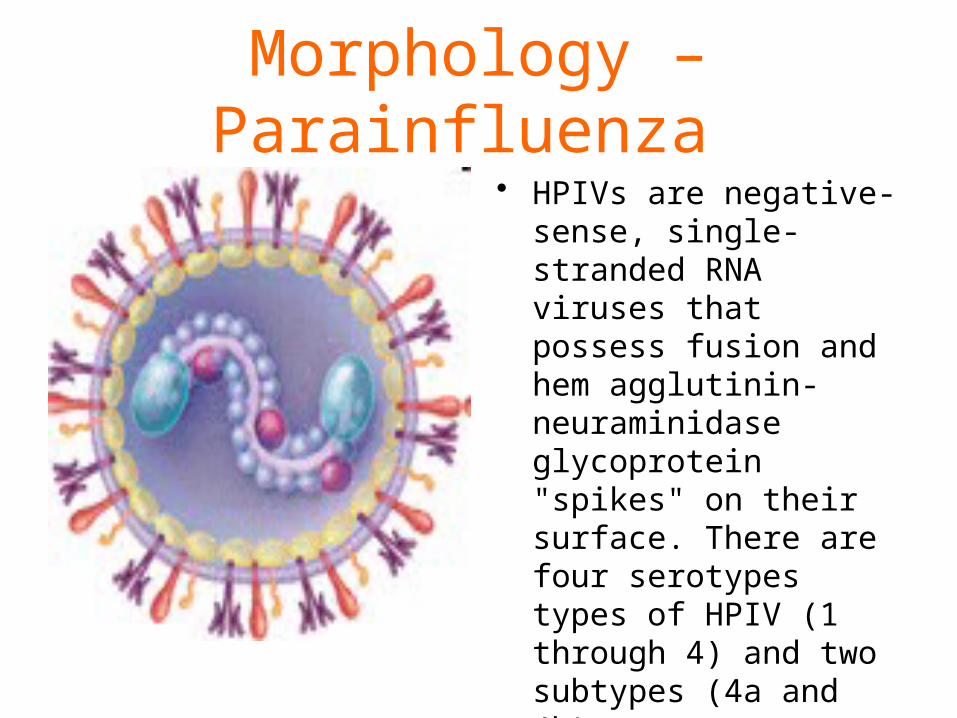
Morphology – Parainfluenza • HPIVs are negative-
sense, single-stranded RNA viruses that possess fusion and hem agglutinin-neuraminidase glycoprotein "spikes" on their surface. There are four serotypes types of HPIV (1 through 4) and two subtypes (4a and 4b).

Virion• The Virion varies in
size (average diameter between 150 and 300 nm) and shape, is unstable in the environment (surviving a few hours on environmental surfaces), and is readily inactivated with soap and water.
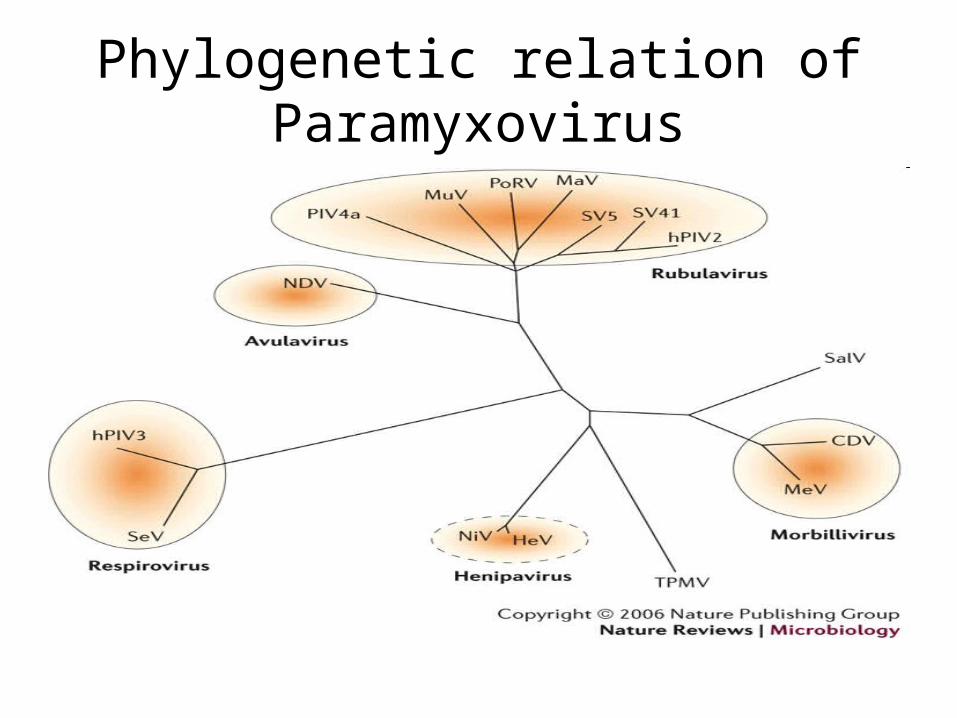
Phylogenetic relation of Paramyxovirus

There are four serotypes in Paramyxoviridiae
• HPIV-1 (most common cause of croup; also other upper and lower respiratory tract illnesses typical)
• HPIV-2 (causes croup and other upper and lower respiratory tract illnesses)
• HPIV-3 (associated with bronchiolitis and pneumonia)
• HPIV-4 (includes subtypes 4a and 4b)
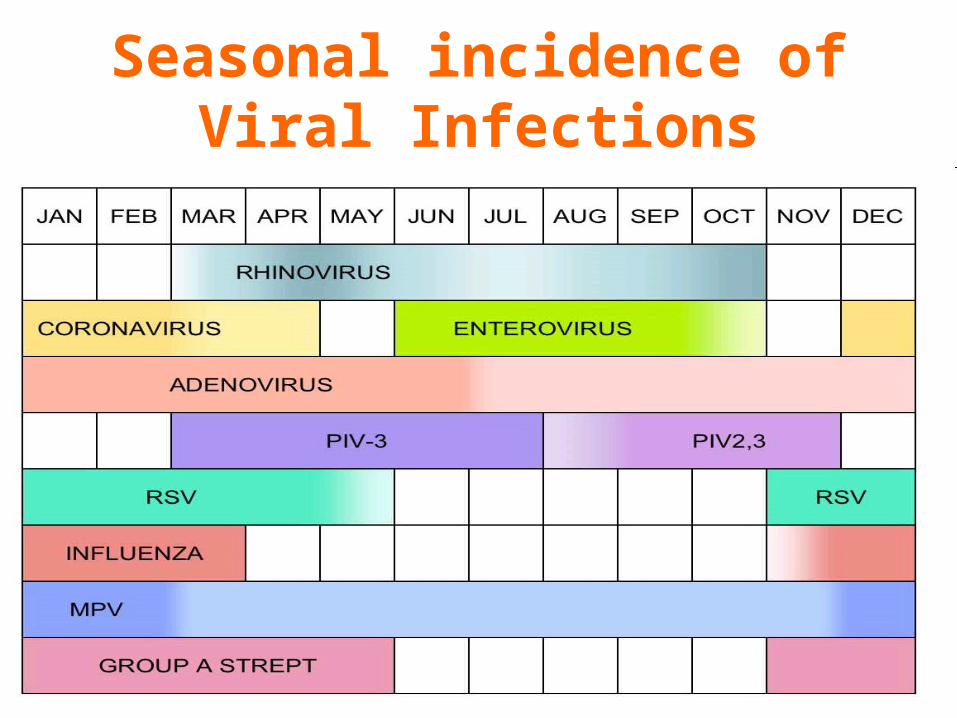
Seasonal incidence of Viral Infections
Present with Respiratory illness
• The most distinctive clinical feature of HPIV-1 and HPIV-2 is croup (i.e., laryngotracheobronchitis); HPIV-1 is the leading cause of croup in children, whereas HPIV-2 is less frequently detected. Both HPIV-1 and -2 can cause other upper and lower respiratory tract illnesses.

Viral entry and Pathogenesis
Parainfluenza infections spread through respiratory tract
• HPIV infection is acquired through inhalation of infected droplet nuclei or indirectly through contact with infected secretions. The incubation period is generally 2-6 days. See

Mechanisms of pathogenesis in Paramyxoviridiae
• HPIV infection in the respiratory tract leads to secretion of high levels of inflammatory cytokines such as interferon (IFN)–alpha, interleukin (IL)–2, IL-6, and tumor necrosis factor (TNF)–alpha. The peak duration of secretion is 7-10 days after initial exposure.
Mechanisms of pathogenesis in Paramyxoviridiae
• Increasing levels of certain chemokines such as RANTES (regulated upon activation, normal T-cell expressed and secreted), macrophage inflammatory protein (MIP)–K are detected in the nasal secretion of paediatric patients
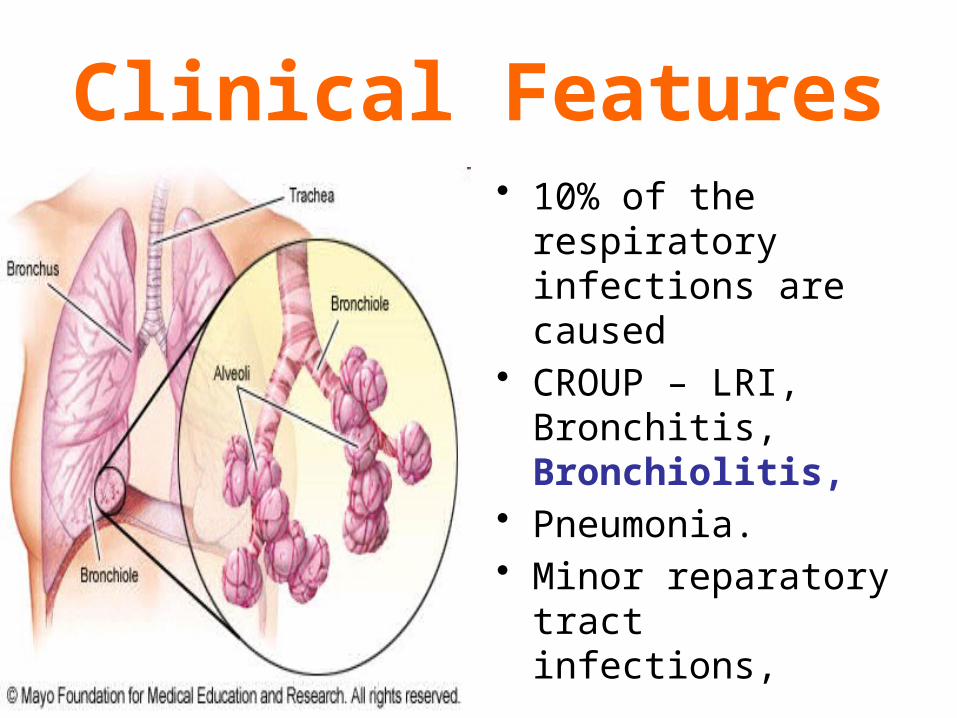
Clinical Features• 10% of the respiratory
infections are caused • CROUP – LRI,
Bronchitis, Bronchiolitis,
• Pneumonia.• Minor reparatory tract
infections,
Children present with Respiratory infections
• A broad range of findings is observed and may include fever, nasal congestion, pharyngeal erythema, non-productive to minimally productive cough, inspiratory stridor, rhonchi, rales, and wheezing.

Clinical Features• Respiratory illness,• Febrile Rhino rhea,• Tracheo Bronchitis,
• Pneumonia.• Immune deficient
High Mortality.• Otitis Media • Sudden Death
Syndrome.
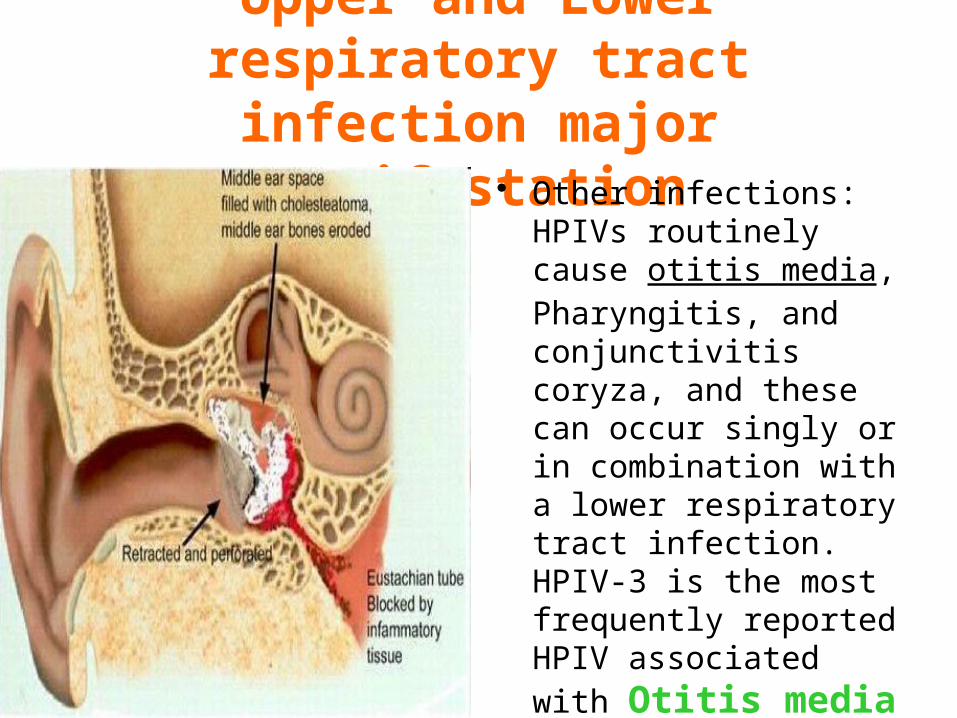
Upper and Lower respiratory tract infection major
manifestation• Other infections: HPIVs
routinely cause otitis media, Pharyngitis, and conjunctivitis coryza, and these can occur singly or in combination with a lower respiratory tract infection. HPIV-3 is the most frequently reported HPIV associated with Otitis media
Parainluenza infection in Immunosupressed
Immunosuppresed people, such as transplant patients, Parainfluenza virus infections can cause severe pneumonia, which is often fatal
Epidemiology• Common between 6
weeks to 6 months.• Close contacts.• Contaminated fingers,• Fomites,• IgA A important in
Immunity.

Reinfections in Para influenza
• Parainfluenza infections do not confer complete protective immunity; therefore, Reinfections can occur with all serotypes and at any age, but Reinfections usually cause a mild illness limited to the upper respiratory tract.
Laboratory Diagnosis
• Nasopharyngeal Swabs
• Nasal washings
• IMF techniques,
• ELISA CF.
Infection with HPIVs can be confirmed with ..
• 1) by isolation and identification of the virus in cell culture or by direct detection of the virus in respiratory secretions (usually, collected within one week of onset of symptoms) using immunofluorescence, enzyme immunoassay, or polymerase chin reaction assay,

Infection with HPIVs can be confirmed with serology
• 2) by demonstration of a significant rise in specific IgG antibodies between appropriately collected paired serum specimens or specific IgM antibodies in a single serum specimen.
Laboratory Diagnosis
• Throat and Nasal Swabs
• Cultured in ,
Monkey kidney and cell lines.
• ELISA, CF,HI
Maternal antibodies protect first few months
• Passively acquired maternal antibodies may play a role in protection from HPIV types 1 and 2 in the first few months of life, highlighting the importance of breast-feeding..

Hand Washing in reduce the infection rates
• Frequent hand washing and not sharing items such as cups, glasses, and utensils with an infected person should decrease the spread of virus to others.

Treatment and Prophylaxis.
• Treatment with Ribavirin
• No Vaccine to date.
• Program created by Dr.T.V.Rao MD for Medical and Paramedical
Students in the Emerging world• Email