Embed Size (px)
Citation preview

Orthopaedics, usual and unusual
Thirty years of experience
Dr L.Prakash M.S., M.Ch (orth) Liverpool

My life as an orthopaedic surgeon went through three phases
1985 to 2001:
The Surgeon

My life as an orthopaedic surgeon went through three phases
2002 to 2015 April:
The learner

My life as an orthopaedic surgeon went through three phases
May 2015 to present:
The teacher and practitioner

First Phase Routine beginnings. M.S.,
MCh etc,
Training under greats like Freeman, Muller, Goodfellow, Monk, Wroblowski, Boyle, Klenerman, Owen, Taylor etc.
Career as a Trauma and Joint replacement surgeon.

During this phase, I was: A prolific surgeon, Innovator, and wrote four books and
conducted 80 workshops.

During this phase, I operated in 106 operation theaters across the country and
abroad, demonstrating surgical techniques and was the Secretary and Vice President of Indian Orthopaedic Association.

During this phase,
VERY OCCASIONALLY TREATED A FRACTURE CONSERVATIVELY

Second Phase:
Dramatic change in my life.
From an orthopaedic surgeon, I became a life convict prisoner in the dreaded Chennai Central Prison.

Life convict in Central prison Chennai
Accused of grave charges and convicted of offences that I would never even imagine committing, I was sentenced to numerous terms of imprisonment including life imprisonment.

13 YEARS IN PRISON
DESPITE BEING TOTALLY INNOCENT

I spent 13 years as a prisoner, eight as an under trial and seven as a life convict, under difficult, desperate
and depressing circumstances.

This is my experience of practicing orthopaedics in those times, with limited
or no facilities, treating desperate patients who had nowhere else to go.

You are not allowed to carry X-Rays out of the prison, and so I have no pictures of fractures, but I maintained meticulous records, on which this paper is based

I also traced the X-Rays that I could lay hands on and the pencil drawings are shown
herewith.

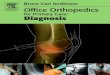
Period spent in the prison 4831 days
Total number of patients seen 11,248
Patients0
500
1000
1500
2000
2500
3000
2171
702 648
3
2670
1121
87
Treatments
Conservative treatment including skeletal tractionManipulations with or without seda-tionSuturing and minor surgeryImplant removal under local anes-thesiaIntra-articular injectionsLocal steroid injectionReferral to other centers

Orthopaedic treatments
Conservative treatment including
skeletal traction 2171
Manipulations with or without sedation 702
Suturing and minor surgery 648
Implant removal under local anesthesia 3 Intra-articular injections 2670
Local steroid injection 1121
Referral to other centers 87

Surgeries inside the prison:
Suturing
Abscess drainage
Removal of thorns
and foreign bodies
Skeletal traction
Implant removal

UNIQUENESS ABOUT PRACTICING ORTHOPAEDICS IN PRISON
No X-ray machine in prison hospital
No POP bandages or traction items
No Lignocaine or local anesthesia
No anesthetic drugs
No sedatives or tranquilizers
Limited suture material
No other facilities.

UNIQUENESS ABOUT PRACTICING ORTHOPAEDICS IN PRISON
If I was taken out of my cell, I
had to treat the patients
through the bars.
If warders during night
rounds wanted
consultations, I would be on
this side of the bars

Doing a blood sugar through prison bars is easy.

Taking BP a little tricky.

Injections are almost a circus or yoga for both doctor and patient

NOW JUST IMAGINE REDUCING A DISLOCATED SHOULDER THROUGH THE PRISON BARS!!
IT IS INDEED UNFORTUNATE THAT I SIMPLY COULD NOT HAVE TAKEN ANY PICTURES!!

INTERESTING PROBLEMS
The torn ear

Using thin nylon sutures, he was operated under local anesthesia on the jailor’s office table

Shoulder dislocations
Total 89
Anterior
83
Posterior 6
Associated with
fractures 9Anter
ior d
isloca
tions
Posterio
r disl
ocatio
ns
Associa
ted w
ith fr
actu
res
83
6 9
PatientsPatients

This my modified Kocher’s method. No huffing and puffing. Only precise application of biomechanics.
Patient needs to be relaxed with or without tranquilizers.

Wait for three minutes by the clock (this is the most important step)

Adduction slowly and gently.

Slow internal rotation to touch the hand to the opposite shoulder. (most often there are no clicks or sounds. Only the dramatic smile on the patient’s face tells you about the reduction.

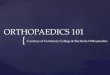
Fractures of the femoral shaft
I had a wonderful opportunity for a study.
Total femoral fractures treated in twelve years 70
Closed fractures 54 Open fractures 11 Fractures infected after fixation
who came to prison subsequently 5
77%
16%7%
Closed fractures
Open fractures
Fractures infected after fixation who came to prison subsequently

Typical femoral shaft fractures seen in prison
Of these; 65 cases happened inside the prison.
Most open fractures were compound from within out.
Most happened after a fall from tree, building watch tower etc

In 2002, a patient named Karuppuswamy climbed up a tree and threatened to jump down.
He slipped, fell and broke his right femur. With a splint, he was sent to the Government hospital, where as a first aid, he was immobilized in a Thomas’s splint.
He was posted for surgery in a few days.

He was in the general ward. And on both his sides were patients with old fractured femurs. Discharging sinuses, foul smell, exposed metal, and heart wrenching stories of months or years of misery.
Karuppuswamy was petrified. He did not allow any surgeon to touch him and was brought back to the prison in a Thomas’s splint

When I was summoned to see him his initial X-Ray looked something liked this.

I thought about it for a day and then asked my assistant outside to get me an Ilizarov half ring, couple of olive wires, couple of wire fixation bolts, and a length of clothesline.

I used double olive wires on upper tibia under local anesthesia

The prison authorities allowed me to use traction on him and I gave an upper tibial traction somewhat like a Fisk traction using fan hooks and locally designed pullies.
The prison plumber and electrician helped.
Traction was provided by three concrete bricks each about four kilos.

Fisk Traction

The Karuppuswamy story Traction was provided by
three concrete bricks each about four kilos.
I would measure the femoral length daily, and ensure that there was no rotation.
Knee was kept flexed most of the time over pillows to traction level.

He was sitting up in a week and moving in the bed in two. He was out of the bed by the fifth week, walking with a six feet bamboo cane.
In three months he was walking and by fourth month back to playing football.
No locking plates, no flexible nails, no rigid locking nails, no protruding stubs, no scars, full function, three degree valgus and half an inch shortening

The fourth month X-ray was somewhat like this

Femoral fractures
From that time on no convict would get his femur operated.
I managed eleven open (punctured wounds from inside) and 54 closed femoral fractures all with excellent results.
The scientific data is being analyzed for publication. It is a real pity that the circumstances and situations did not allow me to get or copy the radiographs.

Dislocated hips 11 cases in thirteen years. Three associated with
acetabular fractures. All treated by closed
reduction Excellent results in all but
one who developed OA after four years. He is coming to me shortly for a hip replacement.

PROBLEMS TREATED
Low back ache
Knee arthritis
Knee injuries
Frozen shoulders
Fracture both bones forearm
Fracture tibia/fibula

PROBLEMS TREATED
Colle’s and Smiths fractures Fracture clavicle Fracture neck of humerus Fracture neck of femur Intertrochanteric fractures Fracture shaft of femur Calcaneal fractures Metacarpals and Meta tarsals

THE BACKACHE STUDY
By luck, I had an opportunity to monitor and study a group of 67 patients with CT or MRI proven Prolapsed intervertebral discs treated by various means and could study them for periods up to 13 years, with a mean follow-up of 10 years.

Inclusion Criteria
Patients with persistent symptoms, pain and some neurological deficit
SLR below 40 degrees
Patients who were convict prisoners and could be closely followed up for at least 7 years or more

Age distribution
20 to 30 16
31 to 40 18
41 to 50 20
51 and above 13
No Of Patients0
2
4
6
8
10
12
14
16
18
2016
18
20
13
20 to 30 31 to 40 41 to 50 51 & above

Type of treatments Laminectomy
/ Discectomy 19
Epidural injection 14
Pain killers, physio, exercises 34
28%
21%51%
Patients
Laminectomy/diskectomy
Epidural
painkillers, physio

All operative cases were operated by orthopods or neuro surgeons outside the prison.

All epidural injections were administered inside the Prison Campus by me
Conservative group treated either by me or have taken no treatment

Though this is a prospective study, it is neither double blind nor controlled. I had no control over patients falling into a particular group. Situations determined the group into which the patient fell.

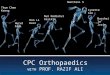
Final evaluation was done by Visual Rating
Scale
Visual analogue scale
Oswestry disability index
No Treatment Injection Operation0
5
10
15
20
25
30
35
40
1 1.3
3.8
1.4 2.1
4.6
11
18
40
Visual Rating Scale Visual analogue scaleOswestry disability index

Conclusions:
No difference between Epidural injection and No
treatment

Conclusions: Surgery gave the worst results
with permanent complications in 19% of the patients

Moral of the story:
Never operate on any prolapsed
disc.
Even those with neurological
deficit or bladder problems get
well after some time.

Principal indications for disc surgery: Holiday for the surgeon and spouse
College admission for surgeon’s son
A new car or holiday home
Or possibly even a speed boat if he operates every back!!

Dr Prakash’s SC index or B/B Ratio
Scrotum/cerebrum×100 Balls over brains ratio While our testosterone urges us to rush into
surgery, cerebral serotonin urges caution We must make our choices wisely

INVALUABLE LESSONS LEARNT Don’t operate in
1, Fracture clavicles 2, Fracture calcaneum 3, Fractures in Children
below ten 4, Prolapsed
intervertebral disc
There are a few exceptions however

How I tackled the knee design of an Indian Knee??
Many questions had intrigued me for a long time.
Now was the time to search for answers.

Question?Are Indian knees Narrower front to back, than their Caucasian counterparts?

Question?Does Squatting since childhood alter the condylar shape?

Question?What is the normal orientation of the femoral condyles in relation to the femoral head? What is the Varus/valgus spread in average population?

Question?Is there a normal Tibial Varus?

Question? Are Indian upper tibias wider from side to side, but narrower from front to back?

Question?
What is the tilt of the tibial articular surface vis a vis the ankle joint in the anterio-posterior direction?

Question? Can anthropometric or Radiological measurements predict the age of onset of OA knees?

Question? Relation between the severity of OA and the state of ligaments in and around the knee?

Methodology employed
Measurement of actual bones 640
Anthropometric measurements 8400 knees (4200 patients)
Radiological measurement of 1300 Radiographs
Total knee joints measured 10340
640
8400
1300
Data
OsteologyRadiographyClinical

At one stage my bedroom had more bones than the Anatomy department

Measurements takenFEMORAL CONDYLE Mediolateral dimensions
Anterioposterior dimension of medial condyle
Anterioposterior dimension of lateral condyle
Femoral valgus/varus

Measurements takenUPPER TIBIA
Mediolateral dimension
Medial anterioposterior dimension
Lateral Anterioposterior dimension
Tibial varus/valgus

Dr Prakash’s modified Galton anthropometric calliper

Conclusions of the above study
LOWER FEMORAL DIMENSIONS WITH SPREAD
Mediolateral 64.5 to 91.2
So Femoral component should be available in 53mm, 56mm 59mm 62mm 64mm 67mm 70mm and 75mm medio-lateral dimensions.
14181
121161201241
0 10 20 30 40 50 60 70 80 90 100
MediolateralNumbers

LOWER FEMORAL DIMENSIONS WITH SPREADAnterioposterior 63.1mm to 86.4mm
So Femoral component should be available in 50mm, 53mm, 56mm 58mm 59mm 63mm 66mm and 70mm AP dimensions.
1 24 47 70 93 1161391621852082312540
20
40
60
80
100
Femur AP
NumbersAnterioposterior
in m
m

Conclusions of the above studyUPPER TIBIAL DIMENSIONS WITH SPREAD
Mediolateral 54.2 to 81.2mm and thus the tibial trays should be available in 55mm, 60mm, 63mm, 66mm, 71mm, 75mm and 81mm
1 21 41 61 81 1011211411611812012212412610
20
40
60
80
100
Tibial dimensions
M-L
dim
ensi
on

UPPER TIBIAL DIMENSIONS WITH SPREAD
Anterioposterior 38.1 to 55.4So tibial trays should come in AP dimensions of 38, 40, 43, 45, 47, 51 and 55mm
1 18 35 52 69 86 103120137154171188205222239256
0
10
20
30
40
50
60
70
80
NumbersAnterioposterior

These dimensional studies helped me to design my knee joint

Artificial hand, and foot prosthesis I used my learnings in the fields of sculpting and rubber
mouding to make hand prosthesis ( cosmetic) for two below elbow amputee convict prisoners. I also developed a method of silicon rubber feet

The steps: Plaster mould

Latex rubber pouring, hand casting, painting


Other things besides orthopaedics 106 books, 25 million hand written words.
Fiction, non fiction, mythological, adventure stories, legal thrillers, sensuous, and detective novels.

Twenty five million words look like this

Twenty five million words look like this as books

Twenty five million words look like this as books

I was then bit by the art bug and started doing water colours

More water colors

Water colors When the selfie bug hit the world, I
was in a small cell without even proper electricity

And so I drew my own selfies

Water color selfies

Water color selfies

I progressed in art to acrylic colors

Acrylic paintings

Charcol Skeches

Caricatures



Charcoal and oil painting

Nest stage was sculpting

Dr L.Prakash’s Hundred sculpture project
Clay,Plaster of Paris, Resins, Acrylic, Marble,
Granite, Epoxy, PMMA, BronzeAluminium, Dental
cement, Gypsum.
I experimented with all materials.

Bronze sculpture work

My experience in metallurgy helped me to cast my TKR prototypes.

I also did a lot of Material research

Masking fluid

Invented PRAKLAY, an air drying polymer clay with numerous applications

Praklay creations

Creations with Praklay

Latex moulding compound

Latex and silicone masks and cinema special efects

And then at last I won!!
I was acquitted in all cases that were foisted on me

When I reached home I was really surprisedFive patients were waiting for me!!

Patients were awaiting my return
The newspapers and televisions had buggered up my reputation
But these patients cared a dam
The next day of my release, I had begun operating

Nature was kind on me, my experiences in art and sculpting had probably made my fingers more accurate

The surgery went off brilliantly
To my luck, I attracted only complex and unusual cases.
And nature has helped me so far, as I have now learnt to respect nature


My Colleagues
I also received a wholehearted welcome from my orthopaedic colleagues and the Indian Orthopaedic Association

In The last nine months I began my practice again and now specialize in complex
and referral cases only. Presently I do revision joints and Ilizarov surgeries.

Designed Ultralite Rings

Designed a Total knee for Indian patient

Wrote three books

Got an ISO 9001-2008 for my clinic

Began an ambitious painting project:
PRAKASH’S ATLAS OF ORTHOPAEDIC EXPOSURES

Conclusions
It is not where you are that matters.
What matters is what you do!!

Conclusions They can take away
your liberty, only you can take away your freedom.
They can imprison your body, only you can imprison your mind

Conclusions
A physician is never off duty. He is there 24/7/365
A scientist finds research material wherever he is; even in a prison

Conclusions Keep meticulous records, you don’t
know when they will be useful

Conclusions Keep smiling, for no trouble lasts for
ever. The rainbow is out there.

Thank You