Embed Size (px)
Citation preview
Guidance When You Need It Most
Genesis Healthcare Consultants is an Authorised FSP No.: 825
Impact of NHI on
Employees,
Employers, and
Medical Aid Schemes
Presented by: Clayton Samsodien
Managing Director
Contents
Global Coverage
Local Challenges
Implications for Employees
Impact on Medical Schemes From the eyes of Healthcare Consultants!
NHI or No – NHI
NHI…More Tax?
What would be the primary funder of NHI?
Payroll tax or increased VAT?
Will this be a similar e-toll debacle?
First broad description of the ANC proposal for NHI contained in an
issue of ANC Today.
(See http://www.anc.org.za/elections/2009/manifesto/manifesto.pdf )

As U.S. argues over health care, nations
embrace global coverage!
WASHINGTON — Even as Americans debate whether President Obama's healthcare law and its
promise of guaranteed health coverage should be scrapped, many far less affluent nations are
moving in the opposite direction to provide medical insurance to all citizens.
Many political leaders around the world also have concluded that creating a system of universal
health care is crucial to remaining competitive and sustaining economic growth.
Source: The SeattleTimes (13 May 2012)
Global Coverage

May, 7 2012
Long waiting times for operations, shortages of medical equipment, rationed resources…. “Canadian taxpayers not getting value for
money… Govt. should consider private insurance options!”
NHI / SHI : Global Challenges
May, 7 2012 USA, New Jersey,
Tom Dwyer. Chief Executive of new
non - profit health insurance company that will be governed by its
members.
May, 17 2012 Former Health Minister,
Yaung Chih-liang, warned that Taiwan's national health
insurance program would collapse if bold steps are not taken to improve finances!
May, 17 2012 Average Swiss Citizen spends US$7,141per annum
Health Care Spend - % of GDP
Switzerland = 11.4 % US 17.4 % UK 9.8 %
Local Challenges
1. Long queues, shortages of equipment and supplies.
2. Staff shortages: nurses, doctors, facilities.
3. Quality of health care services.
4. Infrastructure & resources.
5. Cash strapped provincial governments.
NHI Timelines
1. 1945 - Gluckman Commission proposed full tax funded National Health Service (NHS).
2. Four decades of silence!
3. 1980’s – Debate arose as government support grew for privatisation of health services.
4. 1994 – Health Care Finance Committee – Private insurers could be intermediaries for Social Health Insurance (SHI).
5. 2002 – Taylor Committee of Inquiry – Mandatory contribution for formal sector employees earning above tax threshold.
6. 2011 (August) – Health Minister launches NHI Green Paper.
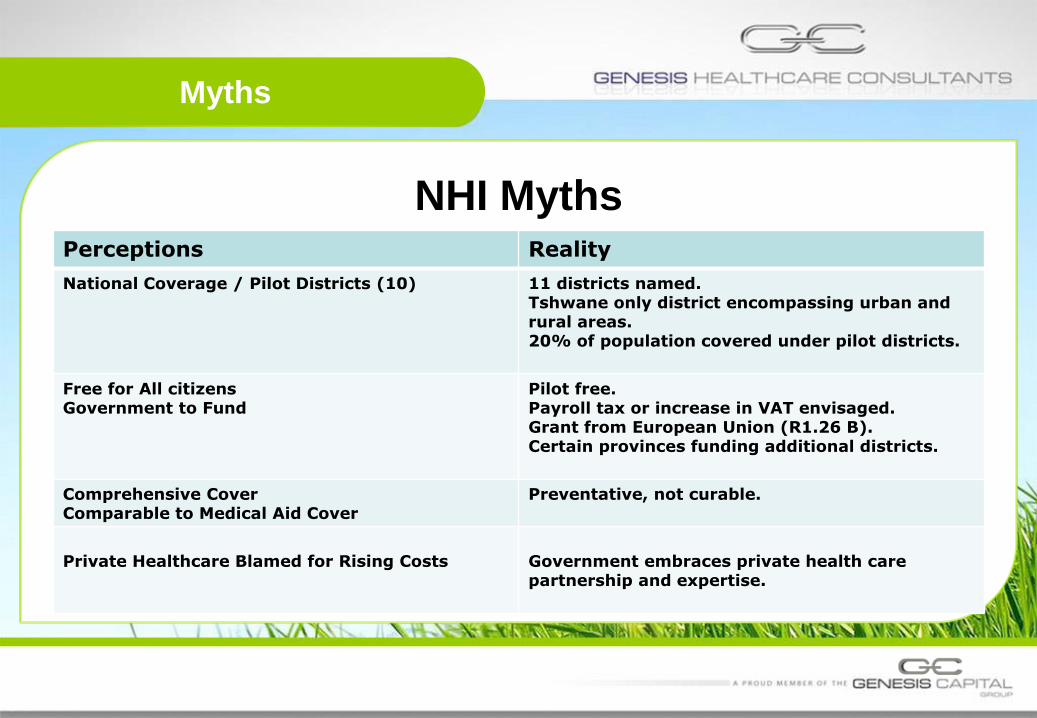
Myths
NHI Myths
Perceptions Reality
National Coverage / Pilot Districts (10) 11 districts named. Tshwane only district encompassing urban and rural areas. 20% of population covered under pilot districts.
Free for All citizens Government to Fund
Pilot free. Payroll tax or increase in VAT envisaged. Grant from European Union (R1.26 B). Certain provinces funding additional districts.
Comprehensive Cover Comparable to Medical Aid Cover
Preventative, not curable.
Private Healthcare Blamed for Rising Costs
Government embraces private health care partnership and expertise.

Progress
NHI Progress
Features Progress
Office of Health Standard Compliance 20 Inspectors trained and appointed.
Hospital Management Reform Posts for Hospital CEO advertised February 2012.
Public Health Facility Audit 3 370 facilities audited. 4 Improvement teams appointed to 4 provinces.
Appointment of District Clinical Specialists 3000 applications received (450 doctors).
Primary Health Care Agents 4500 PHC trained by November 2011.
Appointment of PHC Teams 143 teams trained for Pilot districts January 2012.
Public Hospital Infrastructure 1 967 projects at different stages. 49 nursing colleges infrastructures underway.
Source: Presentation on NHI: Minister of Health: Dr Aaron Motsoaledi, MP (22 March 2012)
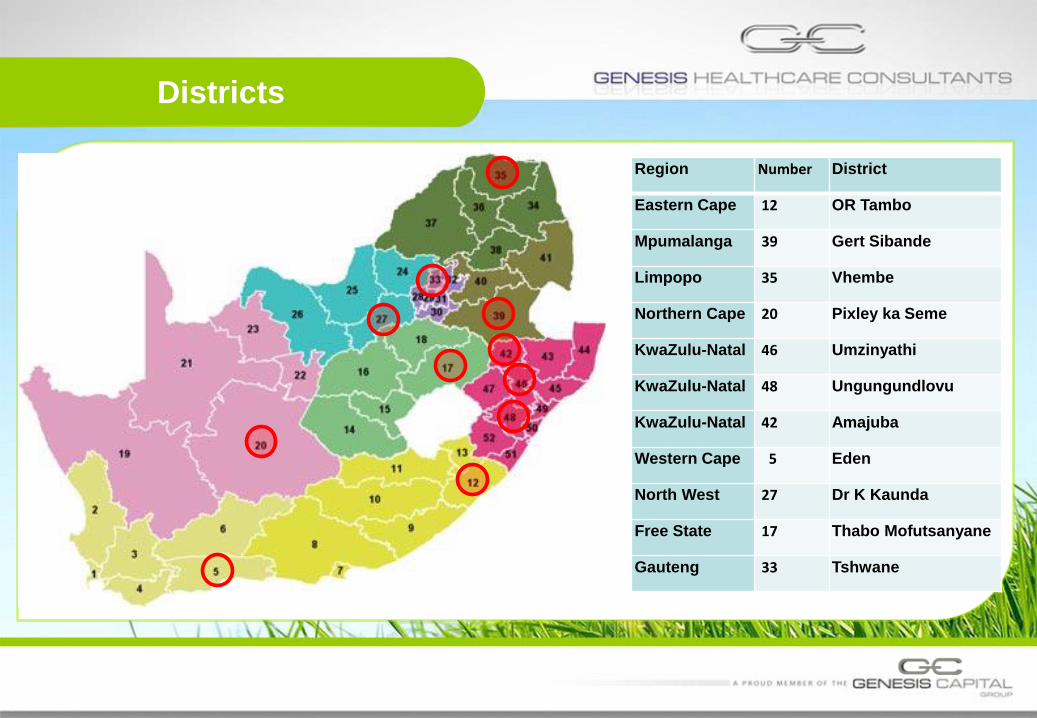
Districts
Region Number District
Eastern Cape 12 OR Tambo
Mpumalanga 39 Gert Sibande
Limpopo 35 Vhembe
Northern Cape 20 Pixley ka Seme
KwaZulu-Natal 46 Umzinyathi
KwaZulu-Natal 48 Ungungundlovu
KwaZulu-Natal 42 Amajuba
Western Cape 5 Eden
North West 27 Dr K Kaunda
Free State 17 Thabo Mofutsanyane
Gauteng 33 Tshwane
Expectations
1. NHI to be implemented over 14 years in 3 phases.
2. What to expect in the first 5 years?
2.1. Strengthening of the health system.
2.2. Improving service delivery platform.
2.3. Policy and legislative reform.
3. Affordability? (media statement – August 2011)
3.1. You will be required by law to contribute if you are earning above a
certain income.
3.2. If you choose to use a provider not accredited by NHI, you will need to
have private healthcare or pay cash for services.
What will be provided?
SUMMARY OF NON-NEGOTIABLES
1. Infection Control Services.
2. Medicines and Medical Supplies, including Dry Dispensary.
3. Essential Equipment and Maintenance of Equipment.
4. Blood Supply and Services: South African National Blood Services.
(SANBS) or Western Province Blood Transfusion Services (WPBTS).
5. Vaccines (Pharmaceutical, Manufacturing).
6. Child Health Services (Including Neonatal and Perinatal).
7. Maternal and Reproductive Health Services.
8. School Health (Quintile 1 and Quintile 2 Schools).
9. HIV & AIDS.
10.TB.
Medical Tax Credit System
Why a Credit System?
1. Signals the permanent acceptance of private healthcare!
2. Equality between high, middle and low income earners.
3. Encourage employees earning above tax threshold to take-up private
healthcare thereby reducing burden on the state.
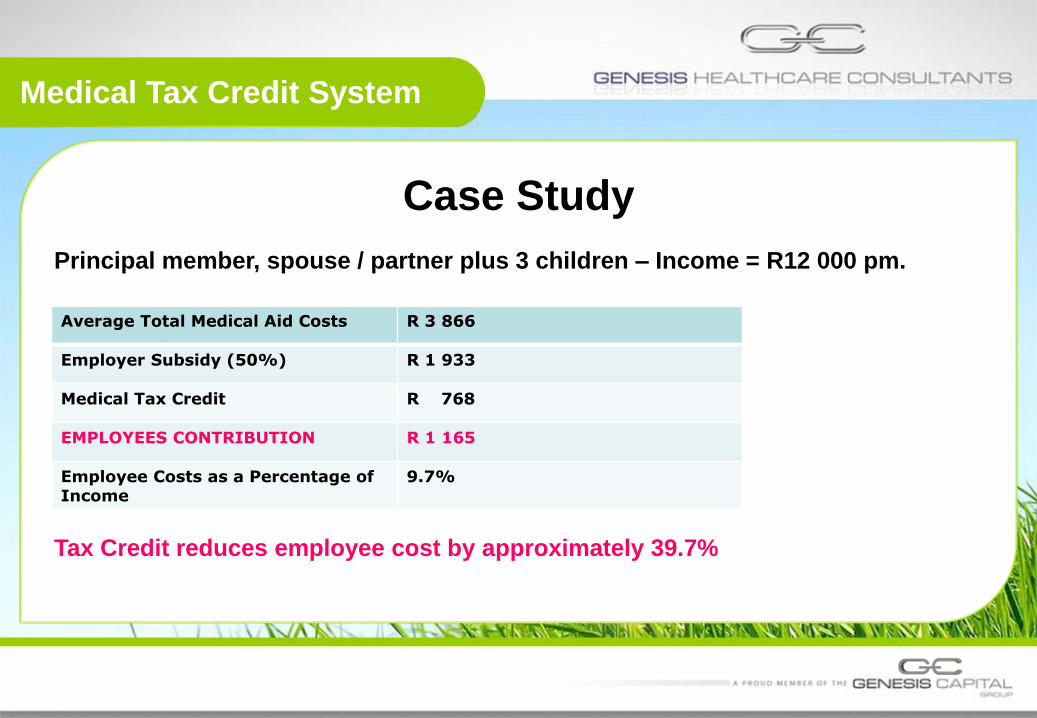
Medical Tax Credit System
Case Study
Principal member, spouse / partner plus 3 children – Income = R12 000 pm.
Tax Credit reduces employee cost by approximately 39.7%
Average Total Medical Aid Costs R 3 866
Employer Subsidy (50%) R 1 933
Medical Tax Credit R 768
EMPLOYEES CONTRIBUTION R 1 165
Employee Costs as a Percentage of Income
9.7%
Summary of Implications
1. NHI is not a medical aid.
2. Primary benefits will be provided in 11 districts, covering 20% of the
population.
3. It will provide preventative, not curable treatment.
4. Major benefits limited to maternal & reproductive services, HIV and TB.
5. Citizens could have dual cover, NHI & private healthcare! And contribute to
both!
6. At most, private healthcare / medical aid, will become top-up cover, similar to
the UK.
Private healthcare and medical schemes will remain in its current form for at
least another decade! Products and benefits will evolve as NHI does!
Advice to Employers
1. Awareness, education and participation of the benefits provided by the pilot in
the relevant districts.
2. Employees in these districts to understand benefits of NHI Pilot.
3. Continue to subsidise employees considering contributions to NHI.
4. Cap subsidies to prevent over-insurance (study revealed that 30% are over-
insured).
5. Cost savings can be used to fund the uncovered?
6. Develop healthcare strategies and collective needs analysis.
Impact on Medical Aids
1. Proposals are that NHI will be done through a government owned entity that is
publically administered, National Health Insurance Fund (NHIF).
2. South African healthcare providers historically do not have much confidence,
or had positive experiences, with government owned / administered entities.
(Road Accident Fund).
3. However, expertise does exist in the private sector with regards to
administration and management of insurance and medical scheme funds.
4. Examples hereof is the administration of Government Employees Medical
Scheme (GEMS) by Metropolitan / Momentum Health.
5. SARS will obviously collect the revenue and distribute the funds for
reimbursement to health fund administrators.
Impact on Medical Aids
1. Medical tax credit reinforces future of medical aid schemes and membership.
2. Demarcation debate launched by Treasury in 2012 (Medical Schemes vs.
Medical Insurance Products) considered to protect the business of a medical
aid.
3. Confidently assume that medical schemes are here to stay. Products may
evolve to provide top-up to NHI.
4. Public Private partnership inevitable for success of the SA healthcare system.
All stakeholders agree.
5. Medical schemes will continue to consolidate / merge, this trend will affect
medical scheme administrators (Momentum and Metropolitan).
The Good News
1. Government recognises social responsibility and finally implementing a
rational long term plan to implement universal coverage.
2. Upgrading of public facilities and accreditation a milestone. Will not only
benefit citizens in the nominated districts (Office of Health Standards
Compliance).
3. Tax credit for employees earning above the tax threshold.
4. Private healthcare to be retained.
5. Public Private Partnership.
6. Substantial progress made since 2011 w.r.t. building blocks for NHI.
The Swiss Experience
What can we learn?
1. The 1994 Act sought “perfect managed competition with full coverage in
basic health insurance”.
2. Substantial minimum benefits for all, but encourages competition between
insurers.
3. Elements of co-pay and excesses give incentives to patients to economise,
similar to some benefit structures in R.S.A.
4. No discrimination against the ill, open enrolment and community rated
contributions, as in R.S.A.
5. The Swiss spends 11.4% of GDP on health, R.S.A spends 8.5% on health,
realistic plan to raise the tax base spend another 3% of GDP on health.
6. Outcomes can only be the same with similar efficiencies.
THANK YOU
Questions
Contact Details
Mobile: 072 55 464 75
Office: 011 731 5111
Email: [email protected]