Embed Size (px)
Citation preview

For educational purposes only
Neuro-imaging ���in Emergency Conditions
Rathachai Kaewlai, MD Division of Emergency Radiology Department of Radiology, Ramathibodi Hospital, Bangkok Annual Scientific Meeting of the Neurological Society of Thailand 15 Nov 2015, Dor-shada Resort by the Sea, Chonburi
Ramathibodi Emergency Radiology
For educational purposes only
Outline
CT vs. MRI for brain disorders
Radiation and IV contrast issues Systematic interpretation of emergency brain CT Cases demonstrating pearls and pitfalls in interpretation

For educational purposes only
Neuro CT vs. MRI
It’s like comparing a phone camera and an SLR
Inexpensive, fast, convenient Expensive, slow, inconvenient
but clearer pictures

For educational purposes only
CT: Pros and Cons
Good for “serious, life-threatening” problems
Good for hemorrhage and bones Good “enough” Clinically relevant findings in most emergent situations
Cons: Diseases in early stages, non-hemorrhagic lesions
Radiation exposure Contrast: Acute kidney injury, hypersensitivity

For educational purposes only
CT Radiation Exposure
Medical radiation IS a major source of radiation exposure in human – NCRP#160 (year 2009; National Council on Radiation Protection & Measurements)
37%
36%
12% 2% 0%
5% 3% 5%
Medical procedures
Natural sources

For educational purposes only
CT Radiation Exposure
Medical radiation errors are EXPOSED – more public attention

For educational purposes only
Tissue Sensitivity
Most sensitive
Least sensitive
Bone marrow (red), colon, lung, stomach, breast, lens Gonads Bladder, esophagus, liver, thyroid Bone surface, brain, salivary glands, skin
Ref: ICRP 2007
Tissue Sensitivity ! ~ rate of cell proliferation ! Inversely ~ to age ! Inversely ~ to degree of cell
differentiation ! Higher dose = more damage ! Young = more damage

For educational purposes only
Diagnostic x-ray Risk Procedures Effective Dose
(mSv) Risks
CXR (PA), extremity XR <0.1 Negligible
Abdomen XR, LS spine XR 0.1-1 Extremely low “death from flying 7200 km”
Brain CT, single-phase abdomen CT
(1-3) 1-10
Very low “death from driving 3200 km”
Multiphase CT 10-100 Low
Interventions, repeated CT >100 Moderate

For educational purposes only
What You Can Do
Be aware of radiation risk from CT
Use the right test with the right indication Be specific when requesting studies Ensure your radiologists have focused protocols for
specific indication, age and patient size Check estimated dose of your patients

For educational purposes only
Checking Estimated CT Doses of Your Patients
CT Dose Report (last series on PACS)
Generally acceptable standard CTDIvol <75 DLP <1000 per phase

For educational purposes only
Ramathibodi ER Experience Prior to
2011 2012 –
present Median dose
reduction P value
CTDIvol 109 52 -53% <0.01
Total DLP 2232 943 -57% <0.01
Effective dose 4.7 2.0 -57% <0.01
Sulagaesuan C, et al. J Med Imaging Radiat Oncol 2015 in press
Generally acceptable standard CTDIvol <75 DLP <1000 per phase Ref: ACR, European Commission
Rama ER (now)
Rama ER (2011)

For educational purposes only
Neuro CT with IV Contrast
Quite common, sometimes emergently needed
Should we wait for serum creatinine before administering IV contrast???
Suggested indications for obtaining creatinine before contrast Age older than 60 years History of kidney disease as an adult,
including tumor and transplant Family history of kidney failure Diabetes Rx with insulin or other
medications
Hypertension Paraproteinemia syndromes or diseases Current use of nephrotoxic medications

For educational purposes only
How Much Should We Concern?
Post-contrast acute kidney injury (PC-AKI) “correlative diagnosis” Creatinine change in 48 hours (due to various etiologies) after CM use
Contrast-induced nephropathy (CIN) “causative diagnosis” AKI secondary to contrast, subset of PC-AKI Rare occurrence

For educational purposes only
Contrast-induced Nephropathy���Controversies
Lack of clear definition of AKI
Lack of clear risk thresholds Serum Cr vs. eGFR? Old data from intra-arterial
(not intravenous) injection No control group in most
published literature
Unclear acceptable interval btw baseline renal function and IV contrast use

For educational purposes only
Acute Kidney Injury ���from IV Contrast
Frequency and magnitude of sCr change was similar in patients receiving contrast and those not receiving it
>50% of 30,000 patients having non-contrast CT showed change in sCr
>40% showed change of at least 0.4 mg/dL
Newhouse JH, et al. AJR Am J Roentgenol 2008;191:376-382.

For educational purposes only
IV Contrast: ??? Cause of AKI, Dialysis or Mortality
21346 patients undergone CT, half received IV contrast 1:1 matched on propensity score yielding similar demographics and comorbidities
Radiology December 2014

For educational purposes only
IV Contrast in Stroke Patients Without Knowing sCr: Is It Safe? Several reports in both ischemic/hemorrhagic stroke
patients indicate very low incidence of CIN Oleinik A, et al. Stroke 2009;40:2393
Study with control group, 539 patients No increased rate of CIN with CTA CIN found in 6% of CTA group, 10% of no CTA group “Hospital-acquired nephropathy” ~8%

For educational purposes only
Brief Approach to CT Interpretation
Clinical question first ! look for pathology suspected
Then ! systematic review of images Blood Can Be Very Bad
Check blind spots: sella, skull base, orbits, upper C

For educational purposes only
Reading Emergency Brain CT:���“Blood Can Be Very Bad” Blood Evaluate for hemorrhage (bright white on CT)
Blood isodense around 1-2 weeks Hypodense by 2-3 weeks EDH, SDH, IPH, IVH, SAH and extracranial hemorrhage
Cisterns Four key cisterns examined for blood, asymmetry and effacement: • Perimesencephalic • Suprasellar • Quadrigeminal plate • Sylvian
Brain Look for symmetry, gray-white differentiation, shifting, hyper- or hypodensity
Ventricles Hydrocephalus (first evident in dilation of temporal horns) Compression/shift of ventricular system
Bone Fractures increase suspicion for intracranial injury
Perron AD. Emergency Medicine. Philadelphia, London: Saunders; 2008

For educational purposes only
Brief Approach to CT Interpretation
Anatomical localization Intra- vs. extra-axial Extra-axial: skull/scalp/dura, subarachnoid, ventricles
Intra-axial: grey, white, or both
Vessels
Lesion characterization Density Pattern of edema Contrast enhancement
Mass effect
For educational purposes only
BLOOD
Evaluate for hemorrhage (bright white on CT) Blood isodense around 1-2 weeks
Hypodense by 2-3 weeks
EDH, SDH, IPH, IVH, SAH and extracranial hemorrhage
For educational purposes only
Blood on CT
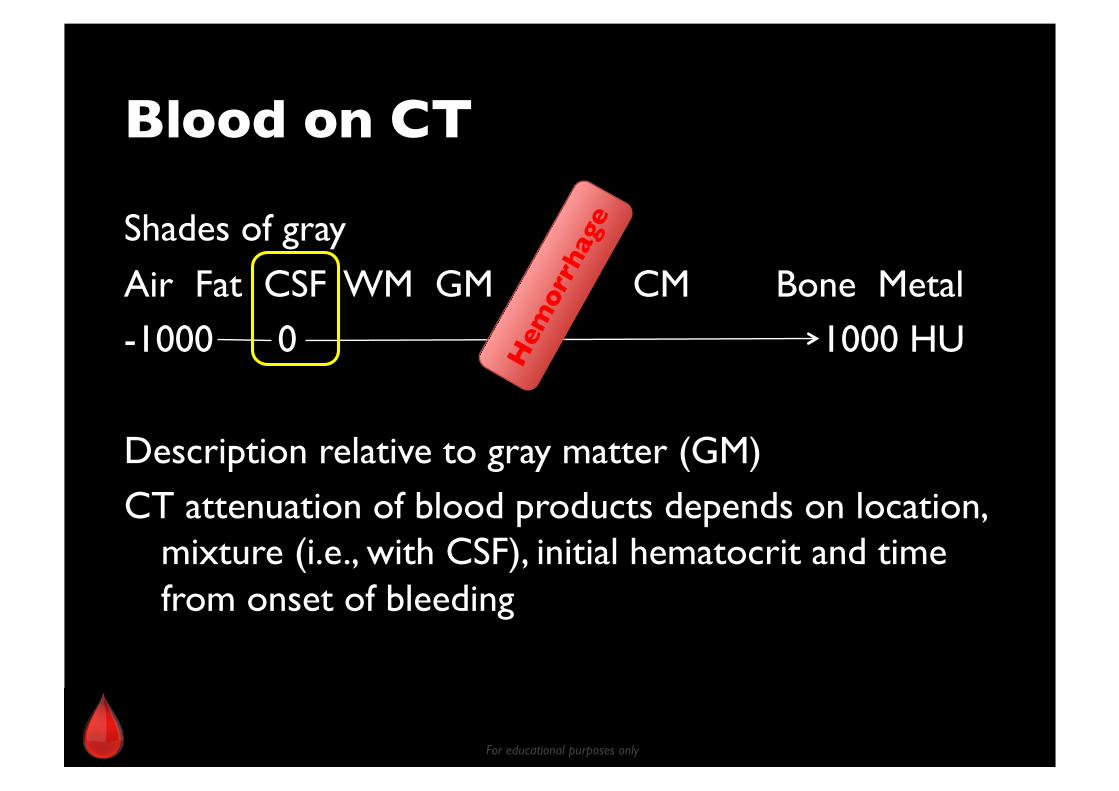
Shades of gray
Air Fat CSF WM GM CM Bone Metal -1000 0 1000 HU
Description relative to gray matter (GM) CT attenuation of blood products depends on location,
mixture (i.e., with CSF), initial hematocrit and time from onset of bleeding

For educational purposes only
Hematocrit Effect
35-45 HU
Whole blood = cells + plasma
55-65% Plasma
Erythrocytes 35-45%
Leukocytes And platelets
0-10 HU
60-90 HU

For educational purposes only
Hypertensive Hemorrhage
50% of primary non-traumatic ICH
Elderly with systemic HTN
Predilection for areas supplied by penetrating branches of MCA and basilar arteries
Putamen and ext capsule 60-65%
Thalamus 15-20% Pons, cerebellum10% Lobar 5-15%
Hypertensive hemorrhage of the right putamen with mild surrounding edema
For educational purposes only
Hypertensive Hemorrhage
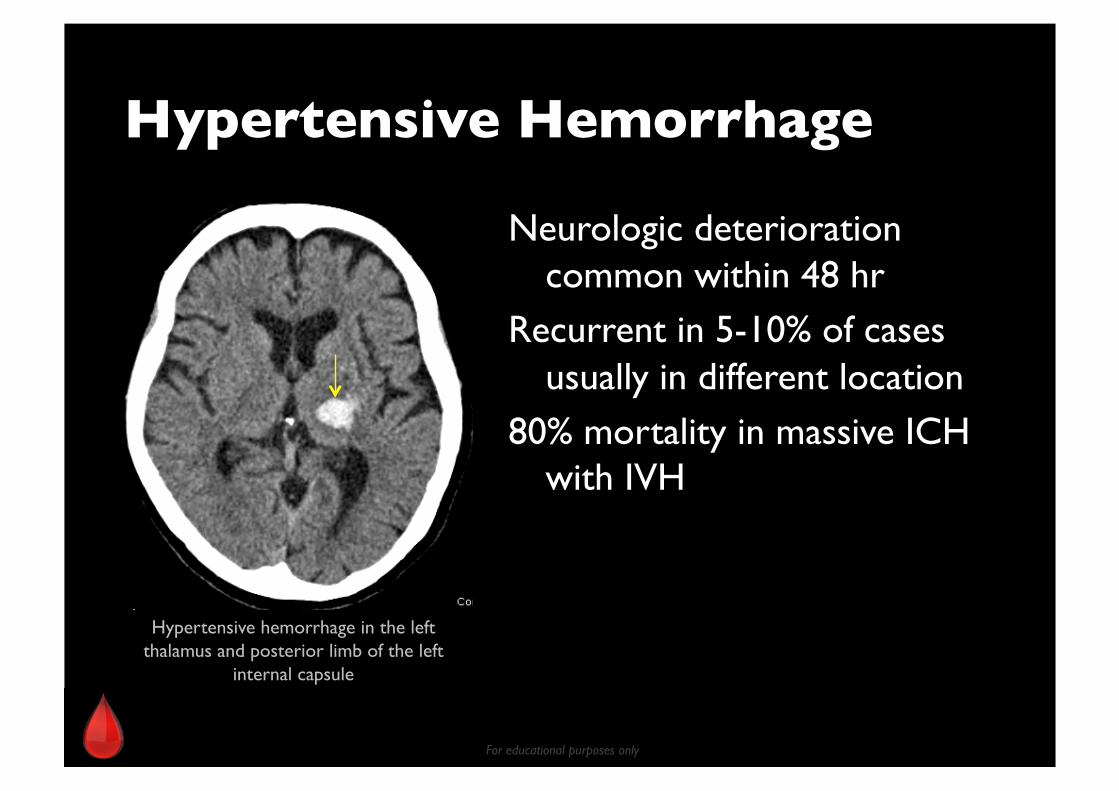
Neurologic deterioration common within 48 hr
Recurrent in 5-10% of cases usually in different location
80% mortality in massive ICH with IVH
Hypertensive hemorrhage in the left thalamus and posterior limb of the left
internal capsule

For educational purposes only
CTA Spot Sign
Suggesting hematoma expansion
Findings Appearance Serpiginous
Spot-like
Location Within margin of IPH No connection to outside vessel
Size >1.5 mm diameter in maximal axial dimension
Density At least double the density (HU) compared to background hematoma
Lesion number Multiple Single
Thompson AL, Kosior JC, Gladstone DJ, et al. Can J Neurol 2009; 36:456.
*
For educational purposes only
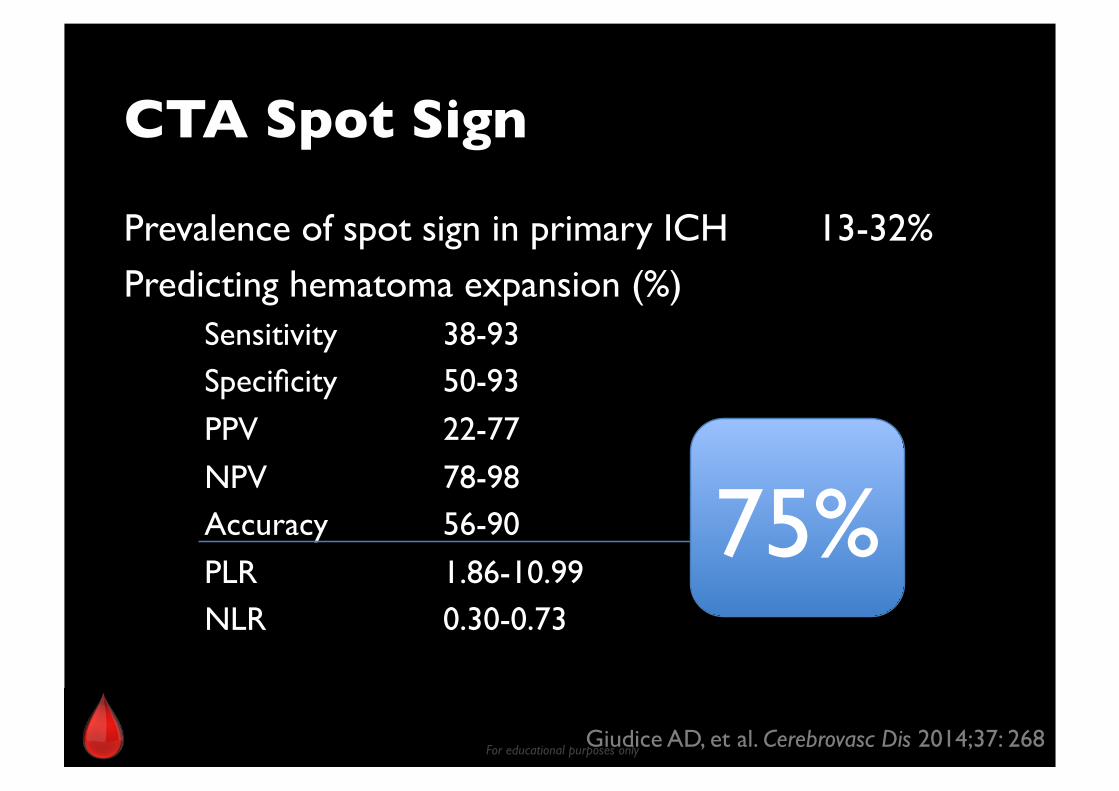
CTA Spot Sign
Prevalence of spot sign in primary ICH 13-32%
Predicting hematoma expansion (%) Sensitivity 38-93 Specificity 50-93
PPV 22-77
NPV 78-98 Accuracy 56-90
PLR 1.86-10.99 NLR 0.30-0.73
Giudice AD, et al. Cerebrovasc Dis 2014;37: 268
75%

For educational purposes only
“CTA spot sign”
1 day – expanding hematoma 2 days later – craniectomy performed
CTA Post
*
* *
For educational purposes only
CTA Spot Sign: Imaging Marker
Hematoma expansion
Active bleeding during surgery Postoperative rebleeding In-hospital death
90-day mortality
May help selecting patients with pICH for specific therapy (medical, surgical hemostasis)
Brouwers HB, et al. Neurology 2014;83: 883 Brouwers HB, et al. Stroke 2015;46: 2498

For educational purposes only
Lobar Hemorrhage: DDx
Vascular malformation, aneurysm
Tumor Amyloid angiopathy Hemorrhagic venous infarct
Hemorrhagic transformation of ischemic infarct
Hypertensive hemorrhage

For educational purposes only
* *
Lobar hemorrhage due to amyloid angiopathy Large lobar hemorrhage of the left temporal lobe without abnormal vessels or
enhancement. Susceptibility MRI showing several other microhemorrhages
Normotensive demented patient with lobar hemorrhage of different stages
*

For educational purposes only
Multicompartmental Hemorrhages: DDx
Trauma Coagulopathy
SAH-IVH Extension of large parenchymal hematoma to other spaces
Coagulopathic ICH: IVH, IPH and SAH

For educational purposes only
Nontraumatic ICH: ���Workup Scheme IPH – Classic hypertensive ! No further W/U
IPH – Lobar ! administer IV contrast (CTA, CTV or post-contrast CT) or MRI/MRA
SAH – CTA to rule out aneurysm rupture SDH, EDH – think trauma first Multicompartment – check coag profile

For educational purposes only
What Else May Appear Similar To Acute Blood on CT?
Pus (i.e., in subarachnoid space, ventricles)
Dense, packed cells
Faint calcification Administered contrast
Post intra-arterial thrombolysis – contrast leakage Differentiation from hemorrhagic transformation of infarct is difficult on first day. In general, contrast leakage decreases attenuation over time

For educational purposes only
CT Hyperdensity: ���Blood or Other Things? Differentiation relies on clinical setting, presence of
surrounding edema, Hct effect, comparison with previous studies
New CT technology may be helpful (dual-energy CT)

For educational purposes only
CISTERNS
Suprasellar Sylvian
Perimesencephalic
Quadrigeminal *Median, unpaired cisterns
Quadrigeminal*
Lamina terminalis cistern*
Interpeduncular cistern
Sylvian cistern
Crural cistern
Perimesencephalic
Suprasellar*
Sylvian

For educational purposes only
Subarachnoid Hemorrhage: Nontraumatic
Ruptured right PcoA aneurysm with SAH 80% of non-traumatic SAH is due to ruptured aneurysm
Commonly cisternal/deep SAH

For educational purposes only
* *
Ruptured right MCA aneurysm with SAH NCCT is 98-100% sensitive during the first 12 hours of onset.
Sensitivity drops to 93% at 24 hours, 57-85% at 6 days after onset

For educational purposes only
Nonaneurysmal perimesencephalic SAH 10% of nontraumatic SAH. Small amount, limited to interpeduncular cistern.
Presumed venous etiology with low recurrence
Images ©Neuroradiology on the Net @blogspot
The other 10% of SAH etiologies: brain AVM, spinal AVM, DAVF, venous infarct, tumor

For educational purposes only
CT-negative, then?
LP more sensitive than CT Negative NCCT but still suspicious of SAH – still need LP (MRI is problematic at perimesencephalic cistern due to
CSF flow artifact)
Medscape.com
For educational purposes only
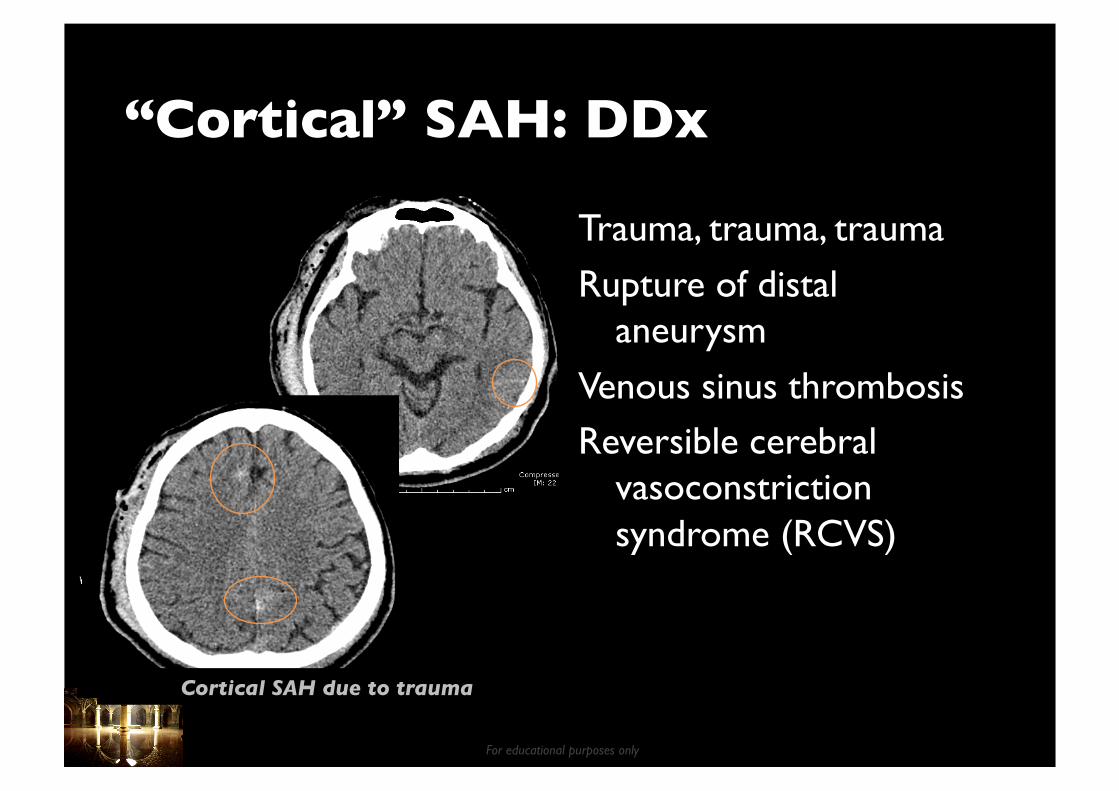
“Cortical” SAH: DDx
Trauma, trauma, trauma
Rupture of distal aneurysm
Venous sinus thrombosis Reversible cerebral
vasoconstriction syndrome (RCVS)
Cortical SAH due to trauma
For educational purposes only
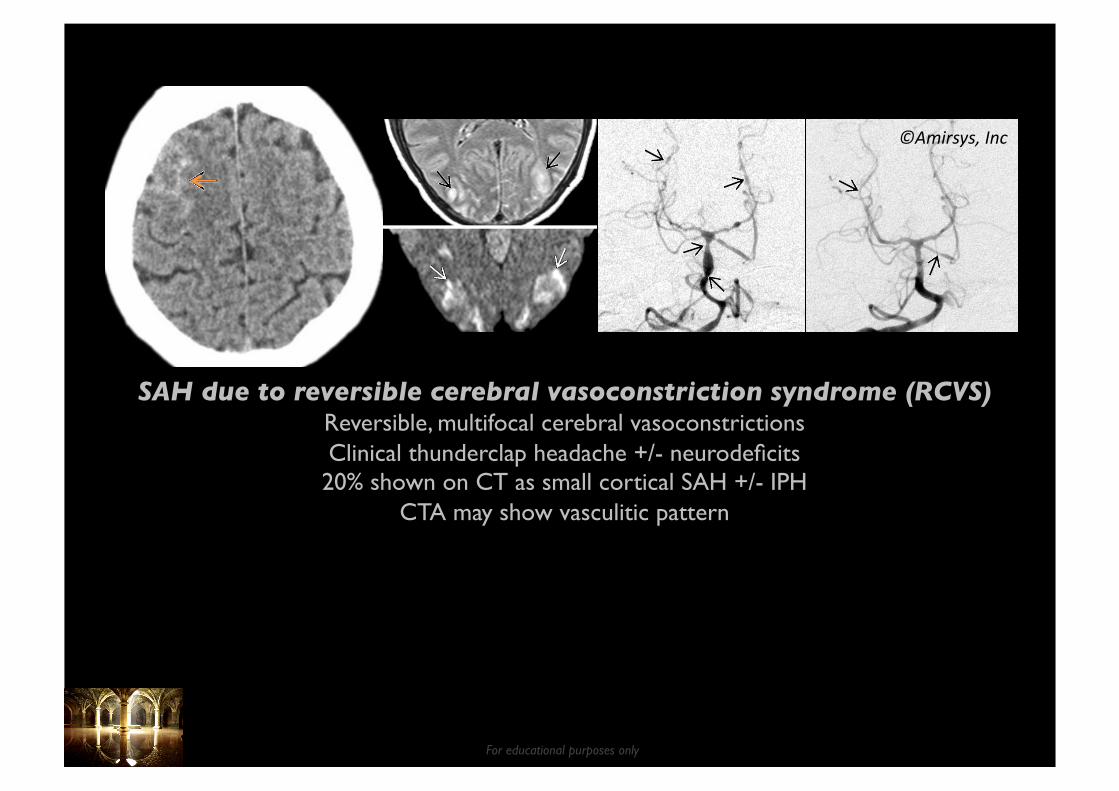
©Amirsys, Inc
SAH due to reversible cerebral vasoconstriction syndrome (RCVS) Reversible, multifocal cerebral vasoconstrictions Clinical thunderclap headache +/- neurodeficits 20% shown on CT as small cortical SAH +/- IPH
CTA may show vasculitic pattern

For educational purposes only
Mimics of SAH
Pseudo-SAH from diffuse cerebral hypodensity
Intrathecal contrast medium Pus
Pseudo-SAH from severe brain edema ©Neurology 2012; 78:e54.

For educational purposes only
BRAIN
Shifting Gray-white differentiation
Symmetry
Hyper- or hypodensity
For educational purposes only
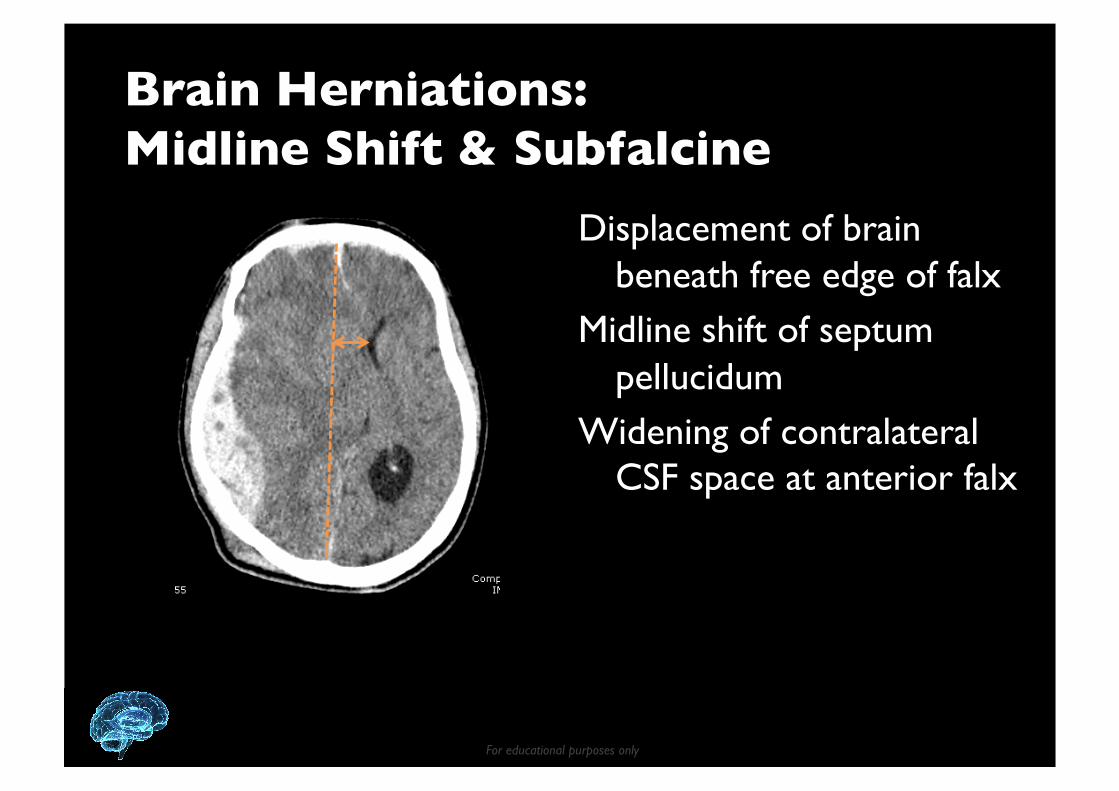
Brain Herniations: ���Midline Shift & Subfalcine
Displacement of brain beneath free edge of falx
Midline shift of septum pellucidum
Widening of contralateral CSF space at anterior falx

For educational purposes only
Brain Herniations: ���Transtentorial
Uncus moves downward across tentorium compressing brainstem
Unilateral or bilateral Obliteration of suprasellar
cistern
Effaced perimesencephalic cistern
Displaced midbrain

For educational purposes only
Brain Herniations: ���Tonsillar
Effacement of CSF cisterns around medulla
Inferior descent of cerebellar tonsils below foramen magnum
For educational purposes only
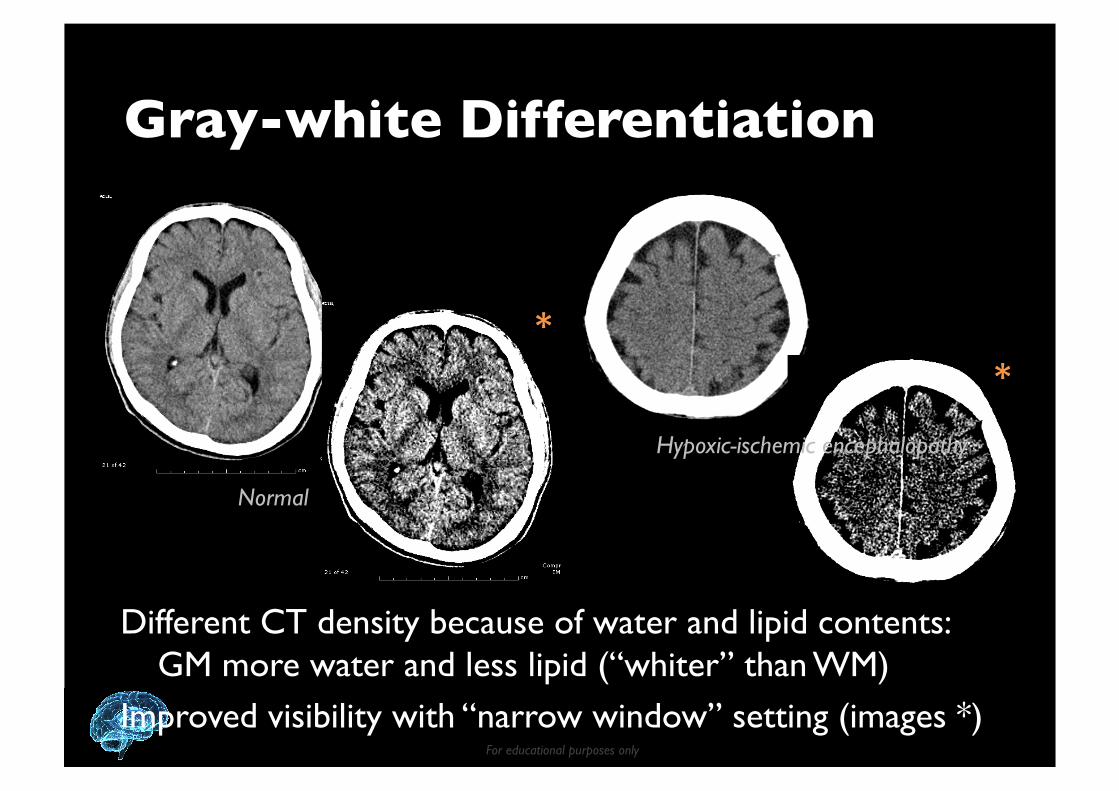
Gray-white Differentiation
Normal
Hypoxic-ischemic encephalopathy
* *
Different CT density because of water and lipid contents: GM more water and less lipid (“whiter” than WM)
Improved visibility with “narrow window” setting (images *)

For educational purposes only
ASPECTS���(Alberta Stroke Program Early CT Score) Assessing early ischemic changes in MCA territory
10 regions assigned a binary score of 0 or 1 depending on presence/absence of hypodensity
Normal CT’s ASPECTS = 10 points
www.AspectInStroke.com Ganglionic level Supraganglionic level

For educational purposes only
ASPECTS���(Alberta Stroke Program Early CT Score) ASPECTS of 7 or less – substantially increased risk of
thrombolysis-related parenchymal hemorrhage Poorer outcomes
Less likely to benefit from IV tPA Score >8 good candidates for IA, <5 typically not
M4
M5
M1
I
M2

For educational purposes only
Vasogenic edema 2/2 metastatic osteosarcoma
Increased GW Differentiation
White matter infarcts 2/2 CADASIL Images from JJ Downer et al. Clin Radiol 2009; 64:298
CADASIL = cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy. “Subcortical infarcts
with diffuse WM ischemica in anterior temporal pole and external capsule in YOUNG individuals”

For educational purposes only
Brain Symmetry
Normal
Bilateral lesions Midline lesion Absence of a normal midline feature
Bilateral absence of normal features
For educational purposes only
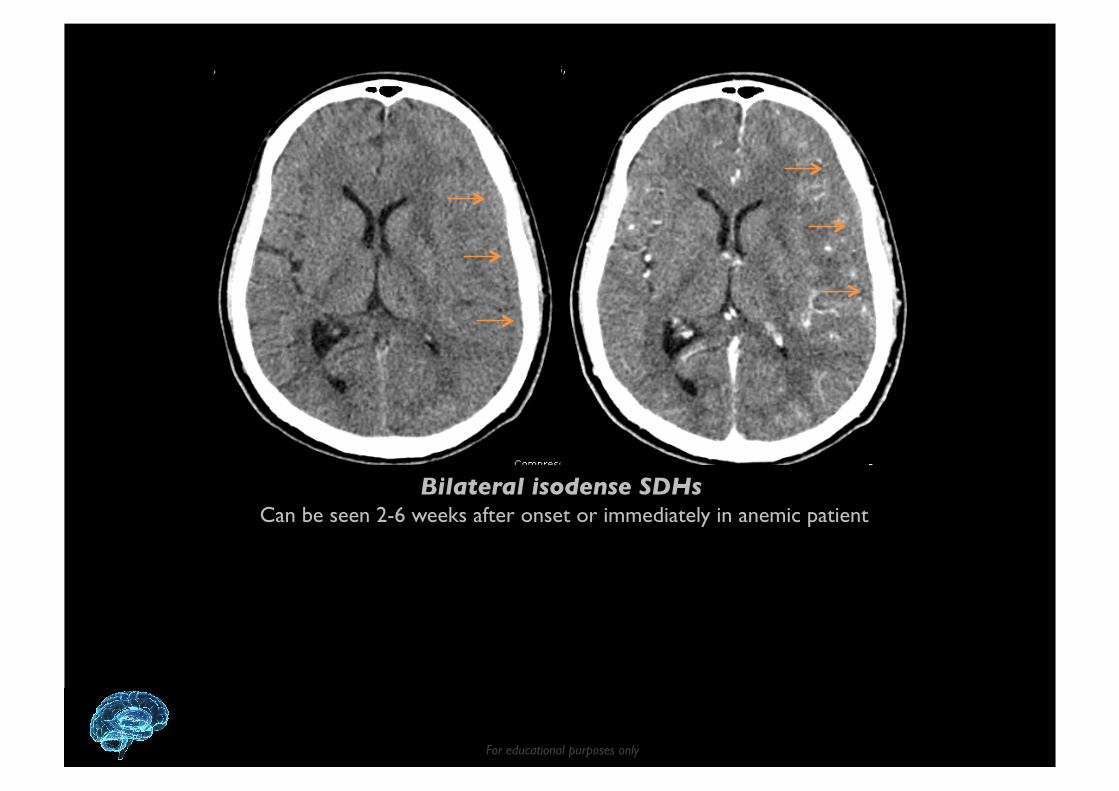
Bilateral isodense SDHs Can be seen 2-6 weeks after onset or immediately in anemic patient
For educational purposes only
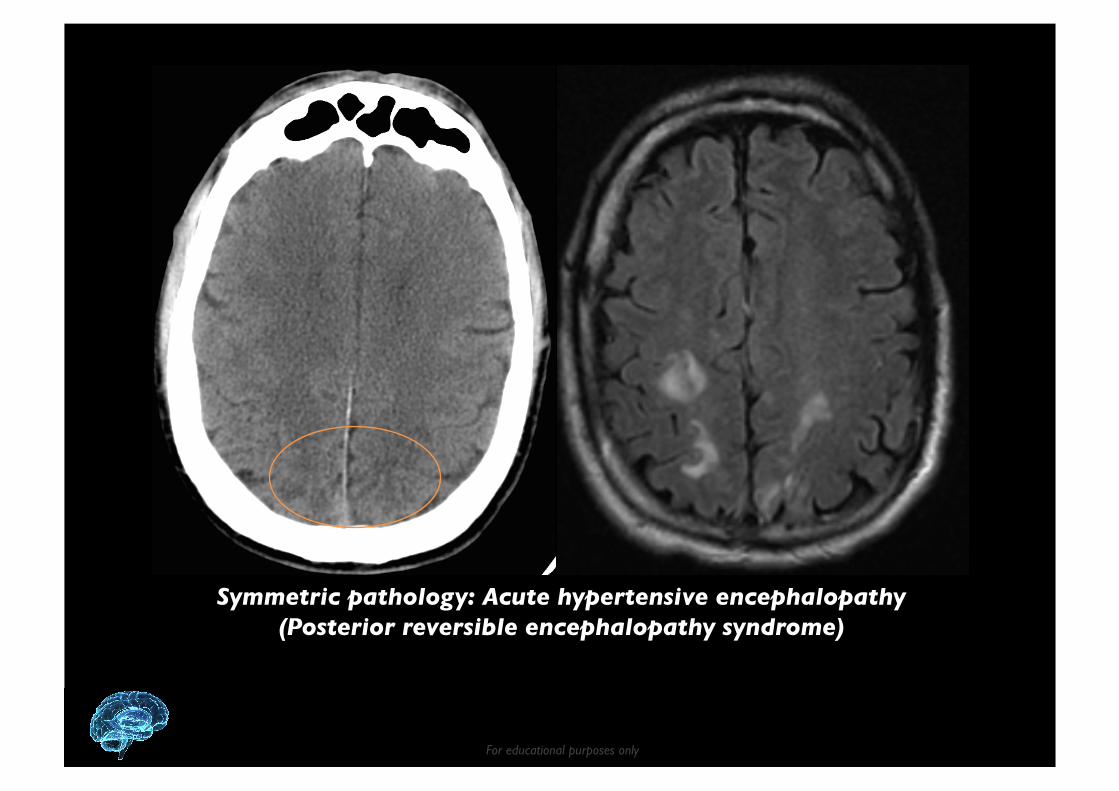
Symmetric pathology: Acute hypertensive encephalopathy (Posterior reversible encephalopathy syndrome)

For educational purposes only
Midline pathology: Sagittal sinus thrombosis
For educational purposes only
VENTRICLES
Hydrocephalus (first evident in dilation of temporal horns) Compression/shift of ventricular system
For educational purposes only
Hydrocephalus
Recognition of ventricular enlargement
Distinguish it from parenchymal atrophy “In hydrocephalus, sulci are effaced relative to ventricular size” Periventricular white matter low attenuation
Transependymal CSF spread due to increased ICP Level of obstruction
For educational purposes only
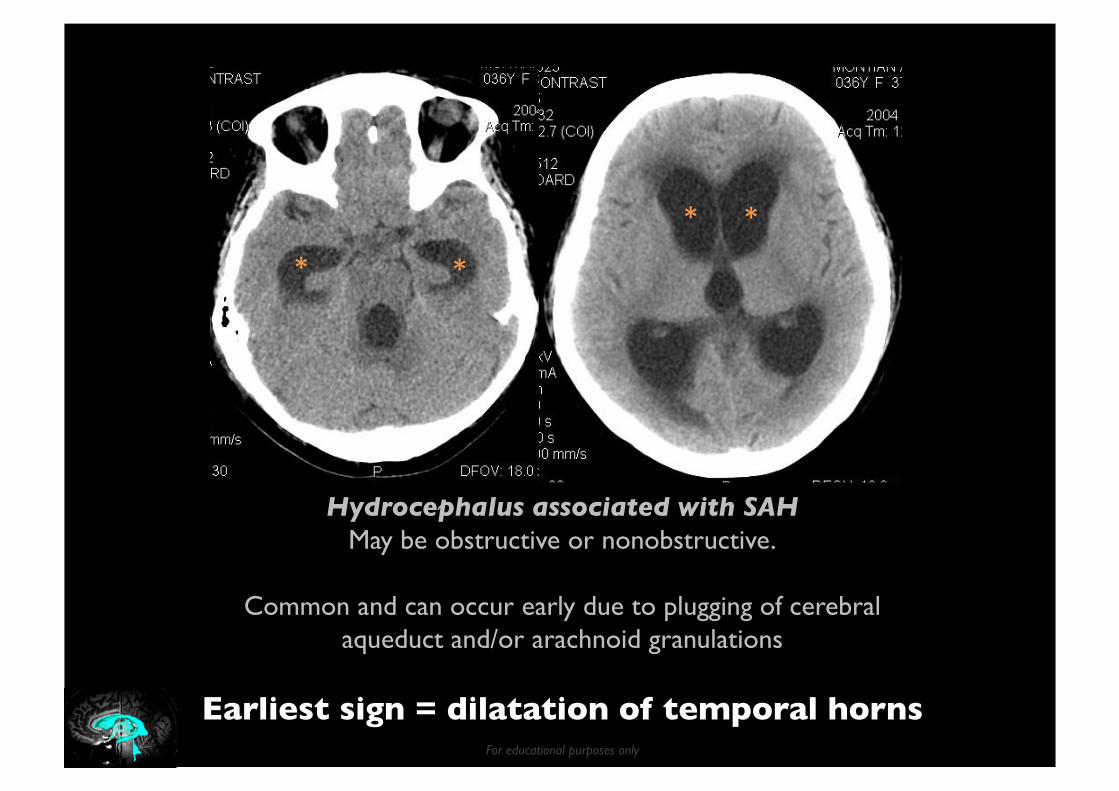
Hydrocephalus associated with SAH May be obstructive or nonobstructive.
Common and can occur early due to plugging of cerebral aqueduct and/or arachnoid granulations
Earliest sign = dilatation of temporal horns
* *
* *
For educational purposes only
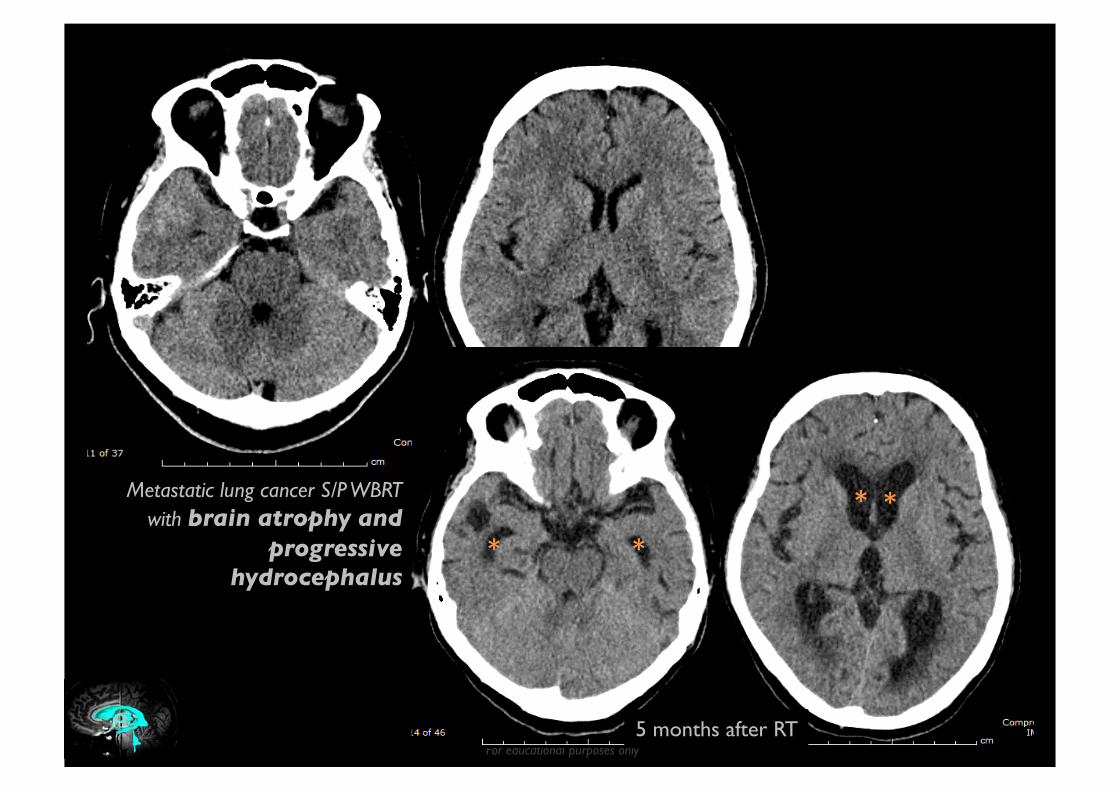
Metastatic lung cancer S/P WBRT with brain atrophy and
progressive hydrocephalus
5 months after RT
* * * *
For educational purposes only
Raised ICP
Complete effacement of third ventricle
Severe diffuse brain swelling of any cause “Third ventricle should be visible in all age groups” Look for other signs: effacement of extra-axial CSF
spaces and tonsillar herniation
For educational purposes only
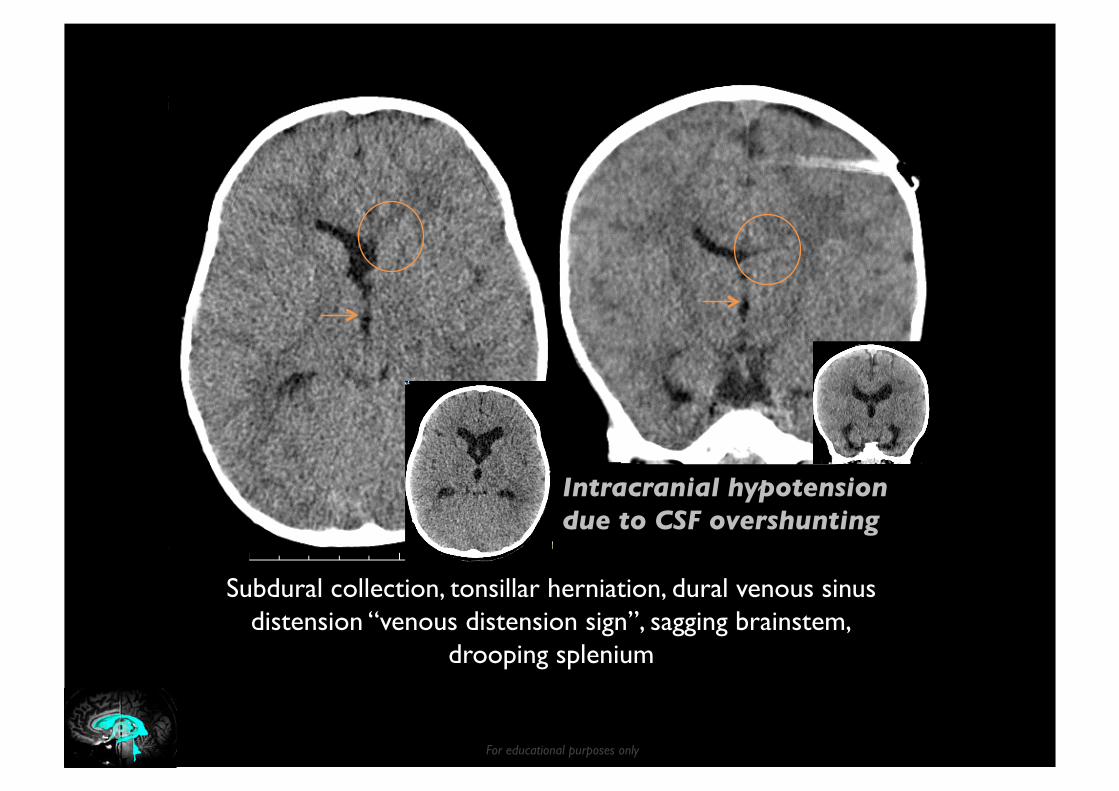
Intracranial hypotension due to CSF overshunting
Subdural collection, tonsillar herniation, dural venous sinus distension “venous distension sign”, sagging brainstem,
drooping splenium

For educational purposes only
SOME PEARLS & PITFALLS
For educational purposes only
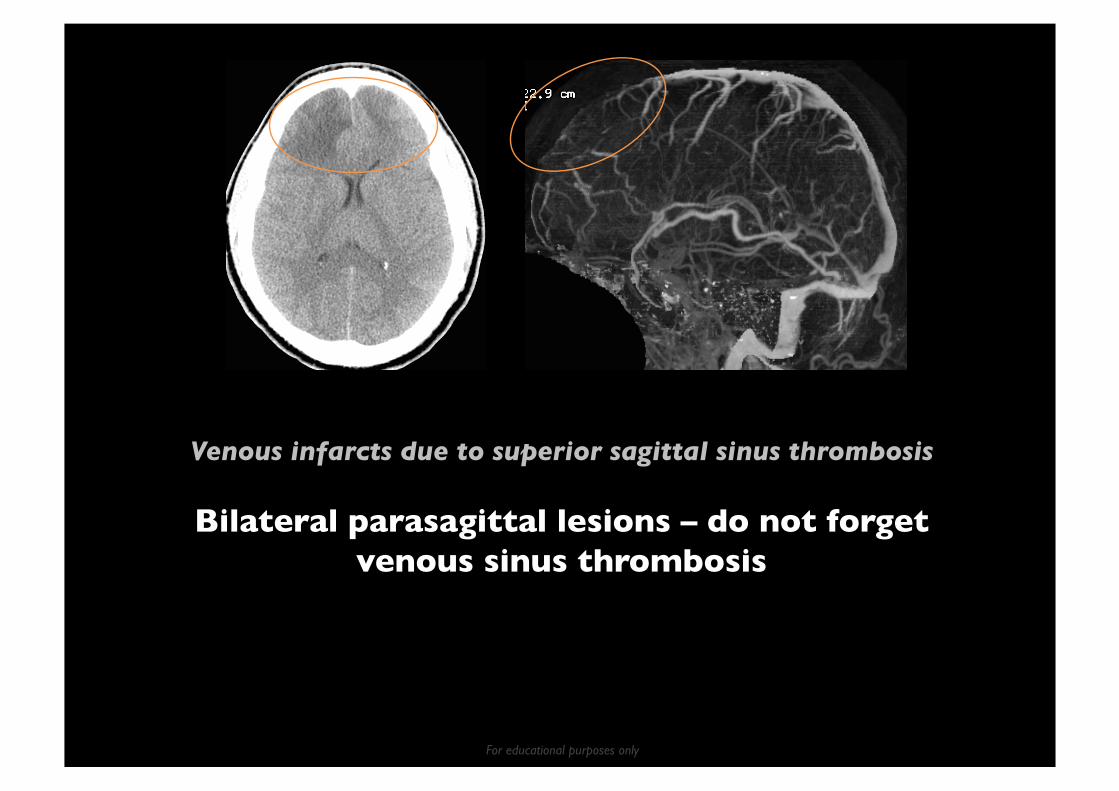
Venous infarcts due to superior sagittal sinus thrombosis
Bilateral parasagittal lesions – do not forget venous sinus thrombosis

For educational purposes only
Hemorrhagic venous infarct due to superior sagittal sinus thrombosis
Cortical SAH – do not forget venous sinus thrombosis

For educational purposes only
Ruptured PCoA aneurysm presenting with IVH
Recognize early hydrocephalus
There should be nothing in the 3rd ventricle except clear black CSF

For educational purposes only
Ruptured AVM presenting with neck pain
Do not forget to look at posterior fossa in neck CT
Brain CT performed later confirming IVH

For educational purposes only 1 day 2 days 3 days
IA thrombectomy performed
CTA: phase 1 phase 2 phase 3
Left hemispheric symptoms for 1 hour
ASPECTS score = 9
IA Rx not recommended
mCTA: Right distal M1 occlusion Delayed collaterals 2 phases and decreased prominence/extent Collaterals score = 2 (intermediate)
Multiphase CTA is a promising tool to help making decision about IA Rx
For educational purposes only
Multiphase CTA in Stroke
Good leptomeningeal/pial collaterals beneficial in stroke
Repeated acquisitions after routine CTA = multiphase “Multiphase CTA”
Degree and extent of pial arterial filling of whole brain in a time-resolved manner
Assess collaterals better than one phase Avoid pitfalls of false occlusion on CTA

For educational purposes only
Multiphase CTA
147 patients
Interrater reliability n=30, k=0.81, P<.001
Menon BK, et al. Radiology 2015;275: 510

For educational purposes only
Multiphase CTA - Interpretation
Score Delayed Filling
Prominence Extent
Good 5 No Normal or increased Symmetric
4 1 phase Normal Symmetric
Intermediate 3 2 phases Normal Normal
1 phase Decreased Decreased
2 2 phases Decreased Decreased
1 phase No vessels in some areas
No vessels in some areas
Poor 1 3 phases A few vessels visible A few vessels visible
0 3 phases No vessels visible No vessels visible
Menon BK, et al. Radiology 2015;275: 510
For MCA territory occlusion Comparing with contralateral asymptomatic side

For educational purposes only
Multiphase CTA
Predicting clinical outcome at 24 hours
Best = baseline infarct volume (<80 vs. >80 mL) 2nd best = multiphase CTA (score >3 vs. <3)
Predicting clinical outcome at 90 days
Best = multiphase CTA (score >3 vs. <3) 2nd best = single-phase CTA (score >2 vs. <2)
Better than CTP mismatch ratio
Menon BK, et al. Radiology 2015;275: 510

For educational purposes only Images from Menon BK, et al. Radiology 2015;275: 510
78yo F, NIHSS 18, Rt hemispheric symptoms 1.5 hrs ASPECTS score = 8
mCTA: Rt M1 occlusion Delayed collaterals 1 phase Collaterals score = 4 (Good) IA Rx recommended
CTP: Blue = infarct core = 113 mL IA Rx not recommended
Incongruent mCTA and CTP IA Rx performed with success

For educational purposes only
Few Words on CT Perfusion
Acute stroke imaging
IV tPA: exclude hemorrhage IA tPA: confirm large-vessel occlusion, define/size “infarct core” (and grade collaterals)
Perfusion imaging does not measure “core”, it’s just probablistic – limited reliability for individual patient
No defined thresholds (different among vendors) New trials IA tPA successful because of new devices
and advanced imaging (occlusion, estimate core)

For educational purposes only
Summary (1)
No “safe” dose of radiation – it’s our responsibility
Concern, but not too much, of contrast-induced nephropathy (CIN)
Systematic CT interpretation “Blood Can Be Very Bad” Keep in mind: IPH due to venous sinus thrombosis Suspected SAH: CT & LP

For educational purposes only
Summary (2)
Use stroke window to identify subtle changes
Be aware of symmetric pathology: midline, bilateral symmetric
Be able to identify “mild” hydrocephalus New technique on the horizon- multiphase CTA for
acute stroke evaluation
For educational purposes only
“Training a neurologist today requires a careful balance between teaching traditional methods of observation-based diagnostic skills and the interpretation of newer and readily accessible imaging techniques.
Ong CJ. Ann Neurol 2015 Apr
In an environment in which head CT is often ordered before patients are even examined, it is difficult to imagine training a neurologist without its ubiquitous presence.”

For educational purposes only
“The challenge of this generation of neurologists is to maintain the framework of localization and disease categorization while optimizing the use of the technology at our disposal.
Addressing this issue may require a more deliberate structuring of resident education.”
Ong CJ. Ann Neurol 2015 Apr

For educational purposes only
“As a neurology trainee myself, I find the advice of the old guard to the new may embodied by the advice of my father, also a neurologist who trained in the 1970s.
‘You correlate the patient with the imaging,’ he would say, ‘not the imaging to the patient’ –”
Ong CJ. Ann Neurol 2015 Apr

For educational purposes only
THANK YOU VERY MUCH FOR YOUR ATTENTION!





























