Embed Size (px)
Citation preview

Dr. Amit VatkarMBBS, DCH, DNB Pediatrics
Fellow in Pediatric Neurology, MumbaiTrained in Neurophysiology & Epilepsy, USA
Contact No. : +91-8767844488Email: [email protected]
Clinical Neurology and Neuro- Examination

CLINICAL NEUROLOGY• Is it Difficult… RITUAL…Formula Based…!• MANOUVERES-MYSTERIOUS SIGNS… (Pronunciation PERPLEXITIES)
• Rare Diseases with too many details.
BASIC PRINCIPLES1) History of Physical Examination2) Anatomic Diagnosis3) Syndromic Diagnosis4) Etiologic ->Pathological diagnosis5) Functional Diagnosis->Potential Restoration of function











CLINICAL EXAMINATION OF NERVOUS SYSTEM
1.Higher functions2.Cranial nerves3.Motor system4.Sensory system5.Cerebellar system6.Stance and gait7.Spine and cranium8.Signs of meningeal irritation
HIGHER FUNCTIONS
• conciousness• orientation• attention• memory• language• psychological status• lobar functions• cognitive skills

Level of consciousness
• Alert: an awake person with a normal level of consciousness.
• Lethargic: a sleepy patient who requires stimulation to maintain an awake state.
• Stuporous: patient can not be aroused to a fully awake state, although they may respond semi-purposefully with withdrawal or moaning to stimulation.
• Comatose: patients with no purposeful response to any type of stimulation.

Orientation
• Classically to person, place, and time (day, date, month, & year).
Memory: • Immediate: name three objects such as “apple, table,
and penny” (ask the patient to • repeat them back to you now). After 5 minutes, ask
the patient to recall those three • objects again. • Short & Long Term: usually assessed at the time of
the medical interview and history.

LANGUAGE
• Comprehension• Repetition• Expression• Confrontation naming• Reading• Writing• Calculation• Constructional ability

Speech / Language
• Usually assessed at the time of the medical interview and history.
• Useful terms involving language/speech include the following:• Aphasia: disorders of understanding, thought, and/or word
finding.• Dysphonia: difficulty with voice production. • Dysarthria: difficulties with the articulation of speech because
of coordination problems • of breath, vocal cords, larynx, palate, tongue, and/or lips.

PSYCOLOGICAL STATUS
• Sleep
• Affect & mood
• Appearance & behaviour
• Abnormal perceptions

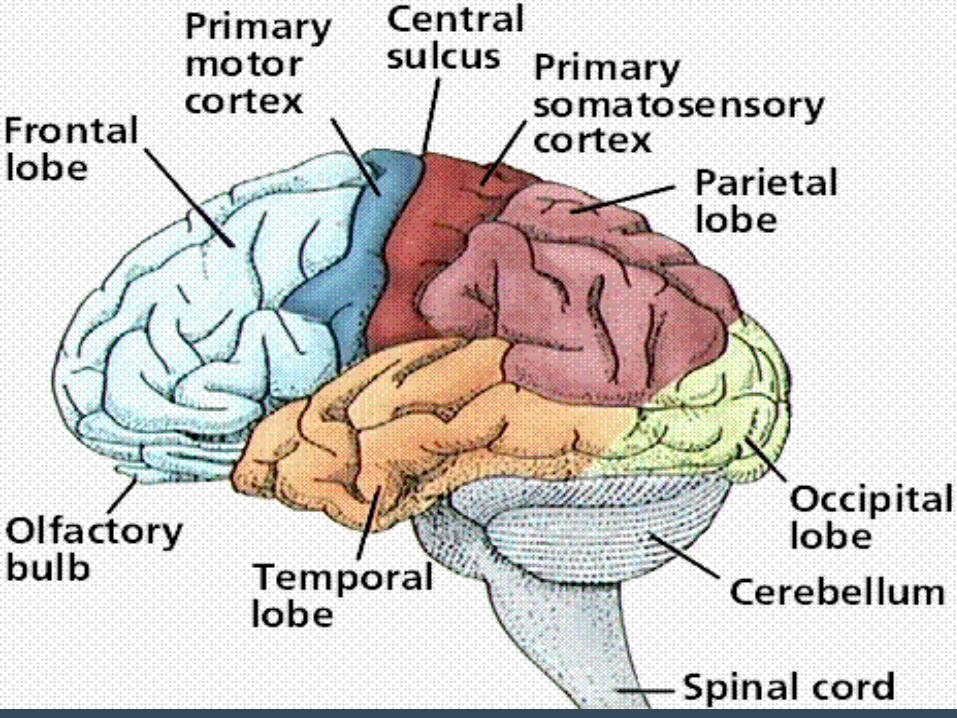
LOBAR FUNCTIONS
• FRONTAL• Classical – Motor• Apathy• Disinhibition• Apraxia• Primitive reflexes
• PARIETAL• Dominant – Cortical sensation,Dyscalculia,Dyslexia• Nondominant - Visuospatial
• TEMPORAL• Memory
• OCCIPITAL• Agnosia
COGNITIVE SKILLS
• Planning & sequencing
• Fund of knowledge
• Insight & judgement
• Problem solving & decision making

CRANIAL NERVES
• OLFACTORY– Pathway– Method of examination– Disorders

OPTIC NERVE
• Components of examination– Visual acuity– Field of vision– Colour vision– Fundus
• Pathway• Method of examination• Disorders

THIRD , FOURTH & SIXTH
• Pathway• Method of examination
– Movements of eyeballs & eyelids– Pupillary reflexes / APRD– Nystagmus
• Disorders

TRIGEMINAL NERVE
• Sensory– Ophthalmic– Maxillary– Mandibular
• Motor– Muscles of mastication
• Pathway• Method of examination• Disorders

FACIAL NERVE
• Motor– Muscles of facial expression
• Pathway• Method of examination• Disorders• Difference between UMN & LMN palsy• Causes for facial nerve palsy in children

VESTIBULOCOCHLEAR NERVE
• Pathway
• Method of examination
• Fundamentals of BERA
• Disorders

NINTH, TENTH, ELEVENTH & TWELFTH
• Pathway• Method of examination• Disorders

Cranial Nerves II-XII
• CN II: visual acuity, visual fields, pupillary reaction, & fundi• CN III, IV, and VI: pupillary reaction & extra-ocular movements• CN V: facial sensation, corneal response, & muscles of
mastication • CN VII: muscles of facial expression• CN VIII: hearing, nystagmus, & balance • CN IX & X: palatal rise to phonation & coordinated swallowing • CN XI: sternocleidomastoid & upper trapezius strength • CN XII: tongue size & movement
• ANATOMY OF CRANIAL NERVES
• STRUCTRES INVOLVED
• LOCALISATION

MOTOR SYSTEM
• Bulk• Tone• Power• Coordination• Abnormal movements• Reflexes
– Superficial– Deep– Autonomic– Primitive / Developmental

POWER
• KNOW • Strength is graded on a 0-5 scale as follows: • 0 = no movement • 1 = flicker of movement or slight twitch • 2 = moves with gravity eliminated • 3 = moves against gravity but not against resistance • 4 = moderate movement against resistance (sometimes
qualified as 4 + if patient can • generate moderate resistance or 4 – if patient can only move
against mild resistance) • 5 = normal strength or power

REFLEXES
• KNOW • Reflexes are graded on a 0-4 scale as follows:• 0 = absent• 1 = present, but depressed • 2 = normal• 3 = increased (hyperactive) • 4 = clonusspasmodc alternaton of muscuar contractons secondary to an
upper motor • neuron lesion) • The foowng refex nerve roots: AchillesS1, S2, PatearL3, L4), BcepsC5), • BrachioradiaC6), and TricepsC7) • A posve Babinski’s signndcates an upper motor neuron process

MOTOR SYSTEM
• Myotomes
• Basics of reflexes
• Reflexes of bladder & bowel
• Localisation especially in spinal cord
SENSORY SYSTEM
• Superficial• Deep• Pathways• Method of examination• Dysfunction

CEREBELLAR SYSTEM
• Anatomy• Mode of examination
– Coordination– Nystagmus– Tremor
• Disorders

STANCE & GAIT
• Types of gait
• AFP
SPINE & CRANIUM
• Spinal defects
• Measurements
• Macewan`s sign
• Auscultation

SIGNS OF MENINGEAL IRRITATION
• Neck stiffness
• Kernig sign
• Brudzinski sign

Dr. Amit VatkarPediatric Neurologist, Navi Mumbai
MBBS, DNB
Email: [email protected] No.: +91-8767844488
Visit us at: http://pediatricneurology.in/
THANK YOU !





























