Embed Size (px)
Citation preview

MONTEGGIA FRACTURE-DISLOCATION IN CHLDRENRockwood & Wilkins’ fractures in children 2015
BY: DR HAMID HEJRATI
RESIDENT OF ORTHOPEDIC SURGERY
IRAN, MASHHAD UNIVERSITY OF MEDICAL SCIENCE

INTR0DUCTION
1814 Giovanni Batista Monteggia, a surgical pathologist and public health official in Milan, Italy
“a traumatic lesion distinguished by a fracture of the proximal third of the ulna and an anterior dislocation of the proximal epiphysis of the radius.”

1967 Jose Luis Bado, while director of the Orthopedic and Traumatology Institute in
Montevideo, Uruguay, classification of Monteggialesions.

CLASSIFICATION
Bado classification
A. Type I (anterior dislocation)
B. Type II (posterior dislocation)
C. Type III (lateral dislocation)
D. Type IV (anterior dislocation with radius shaft fracture)

ASSOCIATED INJURIES
Fracture of the wrist and the distal forearm.
Galeazzi fractures
Radial head and neck fractures type II fractures
Fractured radial neck and midshaft ulnar fracture type I equivalent lesions
Fractures of the lateral condyle

TYPE I
DEFINITION: A type I lesion is an anterior dislocation of the radial head associated with an ulnar diaphyseal fracture at any level. This is the most common Monteggia lesion in children.
ULNAR FRACTURE SITE: metaphysis or diaphysis
INJURY MECHNISMS: direct trauma, hyperpronation, and hyperextension

TYPE I
SIGNS AND SYMPTOMS:, swelling about the elbow, significant pain and limted elbow flexion and extention an forearm supination and pronation, mild valgus, ecchymosis on the volar aspect, PIN pulsy, fullness in the cubital fossa

TYAPE I
RADIOGRAPHIC EVALUATION: maybe normal on AP despite obvius disruption on lateral view. Line drawn through the center of the radial neck and head should extend directly through the center of the capitellum, and remain intact regardless of the degree of flexion or extension of the elbow

TYPE I
TREATMENT:
An anatomic, stable reduction of the ulnar fracture Percutaneous intramedullary fixation of complete transverseand short oblique ulna fractures is standard. Open reduction and internal fixation with plate and screws of the rarer long oblique and comminuted fracture is also standard

TYPE I
stable reduction of the radial head dislocation Irreducible or unstable radial head approached surgically usually involves repairing entrapped soft tissues.
This aggressive approach avoids late complications.

TYPE I
A long-arm cast 4 to 6 weeks forearm in slight supination and the elbow flexed 90 to 110 degrees depending on the degree of swelling.
Radiographs are obtained every 1 to 2 weeks until fracture healing.

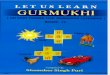
TYPE I
Reduction of a type I Monteggia fracture-dislocation

TYPE II
DEFINITION: A type II lesion is a posterior dislocation of the radial head associated with an ulnar diaphyseal or metaphyseal fracture. This is the most common lesion in adults but very rare in children
ULNAR FRACTURE SITE: metaphysis or diaphysis
INJURY MECHNISMS: direct force and sudden rotation and supination

TYPE II
CLINICAL FINDINGS: The elbow region is swelling, posterior angulation of the proximal forearm, marked prominence in the area posterolateral to the normal location of the radial head.

TYPE II
RADIOGRAPHIC EVALUATION: The typical finding is a proximal metaphyseal fracture of the ulna with possible extension into the olecranon. Midshaft fractures also occur, with an oblique fracture pattern. The radial head is dislocated posteriorly or posterolaterally and should be carefully examined for other injuries.
Accompanying fractures of the anterior margin of the radial head have been noted.

TYPE II
TREATMENT:
Ulnar reduction longitudinal traction.
Radial head reduction spontaneously or with gentle, anteriorly directed force over the radial head.
If the ulnar fracture is stable cast immobilization with the elbow in extension.
If the ulnar fracture is unstable percutaneous intramedullary K-wire
Comminuted or very proximal fractures open reduction and internal fixation with plate and screws or tension band fixation.

TYPE II
The Boyd approach can be used to obtain reduction of the radial head if it cannot be obtained through closed manipulation.
Associated compression fractures of the radial head require early detection to avoid late loss of alignment. Open reduction and internal fixation may be required to maintain radiocapitellar joint stability.
Cast immobilization usually 6 weeks

TYPE II
Longitudinal traction and pronation of the forearm and immobilization in 60 degrees flexion or complete extension

TYPE III
DEFINITION: A type III lesion is a lateral dislocation of the radial head associated with an ulnar metaphysealfracture. This is the second most common pediatric Monteggia lesion.
ULNAR FRACTURE SITE: metaphysis
INJURY MECHNISMS: varus stress at the level of the elbow

TYPE III
CLINICAL FINDINGS: Lateral swelling, varusdeformity of the elbow, and significant limitation of motion, especially supination, are the hallmarks of lateral (type III) Monteggia fracture-dislocations. Again, these signs can be subtle and missed by harried clinicians.

TYPE III
RADIOGRAPHIC EVALUATION: Radiographs of the entire forearm should be obtained because of the association of distal radial and ulnar fractures with this complex elbow injury.

TYPE III
TREATMENT: As with any Monteggia lesion, treatment is aimed at obtaining and maintaining reduction of the radial head, either by open or closed technique. This is usually performed by anatomic, stable reduction of the ulnar fracture that in turn leads to a stable reduction of the proximal radioulnar and radiocapitellar joints.

TYPE III
Immobilization:
If radial head dislocated in straight lateral or
anterolateral 100 to 110 degree
If there is posterolateral component for dislocation
70 to 80 degree

TYPE IV
DEFINITION: A type IV lesion is an anterior dislocation of the radial head associated with fractures of both the ulna and the radius. The original description was of a radial fracture at the same level or distal to the ulna fracture.
ULNAR FRACTURE SITE: diaphysis
INJURY MECHNISMS: hyperpronation and direct blow

TYPE IV
CLINICAL FINDINGS: More swelling and pain are present, Particular attention to the neurovascular status, increased risk for a compartment syndrome.
Failure to recognize the radial head dislocation is the major complication of this fracture.

TYPE IV
RADIOGRAPHIC EVALUATION: The radial and ulnar fractures usually are in the middle third, with the radial fracture usually distal to the ulnar injury. They may be complete or greenstick.

TYPE IV
TREATMENT: Stabilization of the radial fracture converts a
type IV lesion to a type I lesion Closed reduction ,intramedullary or plate fixation fallow type I protocol.
Immobilized in a long-arm cast 4 to 6 weeks in 110 to 120 degrees of flexion with the forearm in neutral rotation.
A short-arm cast is used thereafter if additional fracture protection is necessary.

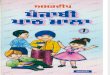
TYPE IV
Reduction schematic for type IV Monteggia fracture

Monteggia Equivalent Lesions
Type I Equivalents
Isolated dislocation of radial head
Radial neck fracture (isolated)
Radial neck fracture in combination with a fracture of the ulnar diaphysis
Radial and ulnar fractures with the radial fracture above the junction of the middle and proximal thirds
Fracture of ulnar diaphysis with anterior dislocation of radial head and an olecranon fracture


Type II Equivalents
Fractures of the proximal radial epiphysis or radial neck.

Type III and Type IV Equivalents
Fractures of the distal humerus (supracondylar, lateral condylar) in association with proximal forearm fractures.

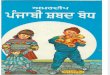
Type III equivalent TYPE IV equivalent

BOYD APPROACH