Embed Size (px)
DESCRIPTION
Presented at the National Academy for State Health Policy's 20th Annual State Health Policy Conference in Denver, Colorado. Author: Robert L. Kane, MD
Citation preview

Minnesota Efforts to Minnesota Efforts to Promote Nursing Home Promote Nursing Home
QualityQualityRobert L. Kane, MDRobert L. Kane, MD
University of Minnesota School of Public HealthUniversity of Minnesota School of Public HealthNASHP MeetingNASHP Meeting
October 15, 2007October 15, 2007

Project TeamProject Team
Robert Kane (UM)Robert Kane (UM) Greg Arling (UI)Greg Arling (UI) Bob Held (DHS)Bob Held (DHS) Valerie Cooke (DHS)Valerie Cooke (DHS) Christine Mueller (UM)Christine Mueller (UM)

A Variety of Strategies A Variety of Strategies Have Been TriedHave Been Tried
Pay-for-PerformancePay-for-Performance Quality BonusQuality Bonus NH Report CardsNH Report Cards Quality Incentive PaymentsQuality Incentive Payments

Pay-for-PerformancePay-for-Performance
Payment based on quality scorePayment based on quality score Payment applied to CMIPayment applied to CMI NHs tiered by quality scoreNHs tiered by quality score Average costs per tierAverage costs per tier NH keeps larger portion or actual NH keeps larger portion or actual
costs according to qualitycosts according to quality

Quality Profile ElementsQuality Profile Elements
Available NowAvailable Now Survey deficienciesSurvey deficiencies Staff/resident ratioStaff/resident ratio Staff retentionStaff retention Use of pool staffUse of pool staff Quality indicatorsQuality indicators % single rooms% single rooms Quality of Quality of
Life/Resident Life/Resident SatisfactionSatisfaction
Under DevelopmentUnder Development Family SatisfactionFamily Satisfaction Short StayShort Stay Community Community
DischargeDischarge Environmental Environmental
Assessment –ability Assessment –ability to support to support independence, independence, dignity and dignity and rehabilitationrehabilitation
Dementia CareDementia Care

Quality ScoreQuality Score
On a 100 point scale, maximum points On a 100 point scale, maximum points assigned to each quality measure are:assigned to each quality measure are:– Direct Care Hours Direct Care Hours 1010– Staff Retention Staff Retention 2020– Use of Pool Staff Use of Pool Staff 55– Quality Indicators from MDS Quality Indicators from MDS 3535– Quality of Life/Satisfaction Quality of Life/Satisfaction 2020– Survey Deficiencies Survey Deficiencies 1010

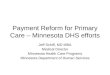
Relation of Case Mix Component + Relation of Case Mix Component + Support Services Cost PPD and Support Services Cost PPD and
Quality ScoreQuality Score
CM & SS Cost PPD
24022020018016014012010080
To
tal Q
ua
lity
Sco
re (
0-1
00
)
90
80
70
60
50
40
30
20 Rsq = 0.0935

Characteristics:Characteristics:
Nursing facility specific ratesNursing facility specific rates Rates are a function of a pre-Rates are a function of a pre-
determined price, quality and actual determined price, quality and actual costs costs
Acuity-based ratesAcuity-based rates Annually re-basedAnnually re-based Prospective rate systemProspective rate system Phase-in over 4 year periodPhase-in over 4 year period

Quality TiersQuality Tiers
Ten tiersTen tiers Ten point incrementsTen point increments Tier 1 - lowest quality scoresTier 1 - lowest quality scores Tier 10 – highestTier 10 – highest

Calculate Target Rates for Calculate Target Rates for Operating ComponentsOperating Components
Costs per patient day for each Costs per patient day for each provider are arrayed for each provider are arrayed for each categorycategory
Lowest populated quality tier target Lowest populated quality tier target rate is 10th percentile of costsrate is 10th percentile of costs
Highest is 90th percentile of costsHighest is 90th percentile of costs Adjusted to achieve budget Adjusted to achieve budget
neutralityneutrality

Quality Incentive PaymentQuality Incentive Payment
Use quality score to adjust difference Use quality score to adjust difference between target rate and specific between target rate and specific facility costfacility costFacilities with costs above or below Facilities with costs above or below
the target rate receive a portion of the target rate receive a portion of the difference, depending on the difference, depending on quality scorequality score
The closer the facility’s costs are to The closer the facility’s costs are to their target rate, the higher their target rate, the higher percentage of the difference the percentage of the difference the facility is paidfacility is paid

The matrixThe matrix
Quality Tier 1 2 3 4 5 6 7 8 9 10
Case Mix Adjusted Support CareCost Minus Target Cost Minus Target
> $25 > $10 0% 0% 0% 0% 0% 0% 0% 10% 20% 30%20 to 25 8 to 10 0% 0% 0% 0% 0% 0% 10% 30% 40% 50%15 to 20 6 to 8 0% 0% 0% 0% 0% 20% 30% 50% 60% 80%10 to 15 4 to 6 0% 0% 0% 0% 20% 40% 50% 70% 90% 100%5 to 10 2 to 4 0% 0% 0% 20% 50% 70% 70% 90% 100% 100%0 to 5 0 to 2 0% 0% 20% 40% 70% 100% 105% 110% 110% 120%
0 to -5 0 to -2 10% 10% 20% 30% 50% 50% 60% 80% 90% 100%-5 to -10 -2 to -4 0% 0% 10% 15% 25% 25% 30% 40% 45% 50%
<-10 -4 to -6 0% 0% 0% 0% 0% 0% 0% 0% 0% 0%
Within These Incremental Amounts: Nursing facility Share Will Be:

Who are the WinnersWho are the Winners
ConsumersConsumers WorkersWorkers Facilities with high qualityFacilities with high quality Facilities that are efficientFacilities that are efficient Facilities that have better physical Facilities that have better physical
plantsplants Facilities that have the ability to adapt Facilities that have the ability to adapt
to a system that demands quality and to a system that demands quality and efficiencyefficiency

Not passed by legislatureNot passed by legislature
Too complicatedToo complicated Some constituents lost moneySome constituents lost money NH oppositionNH opposition No consumer advocacyNo consumer advocacy

Quality Add-onQuality Add-on NHs paid an additional percentage of payments NHs paid an additional percentage of payments
based on quality scoresbased on quality scores Year 1: 5 indicators: turnover (15%), retention Year 1: 5 indicators: turnover (15%), retention
(25%), pool use (10%), MDH survey (10%) and QIs (25%), pool use (10%), MDH survey (10%) and QIs (40%).(40%).
Could earn up to 2.4% of their operating rate Could earn up to 2.4% of their operating rate – set up to be an average 1% quality add-on industry set up to be an average 1% quality add-on industry
wide. wide. – Additional 1.3% as COLA. Additional 1.3% as COLA.
Year 2: quality of life (20%) and direct care hours Year 2: quality of life (20%) and direct care hours per day(10%), retention (20%), QIs (35%), pool per day(10%), retention (20%), QIs (35%), pool (5%) and MDH survey (10%) (5%) and MDH survey (10%)
Could earn up to 0.3% as a quality add-on. Could earn up to 0.3% as a quality add-on. – designed to be .13% on average industry wide. The designed to be .13% on average industry wide. The
remaining 1.87% was given as a COLA. remaining 1.87% was given as a COLA.

NH Report CardsNH Report Cards
Information for consumersInformation for consumers Individualized informationIndividualized information Based on available dataBased on available data

ComponentsComponents
Nursing HoursNursing Hours
Staff TurnoverStaff Turnover
Use of Pool Staff Use of Pool Staff
Proportion of Single RoomsProportion of Single Rooms
Quality Indicators from MDSQuality Indicators from MDS
Survey DeficienciesSurvey Deficiencies
Quality of lifeQuality of life From survey of a sample of residents in each From survey of a sample of residents in each
NHNH

Report Card LogisticsReport Card Logistics User indicated zip code location and User indicated zip code location and
three most important variablesthree most important variables received information on NHs order by received information on NHs order by
preferencespreferences QOL, citations most valuedQOL, citations most valued

Performance-Incentive Performance-Incentive Payment GoalsPayment Goals
Improve the quality of care and Improve the quality of care and quality of life of nursing home quality of life of nursing home residents in a measurable way.residents in a measurable way.
Deliver good quality care more Deliver good quality care more efficientlyefficiently
Rebalance long-term care and make Rebalance long-term care and make more efficient and effective use of more efficient and effective use of resources.resources.

Quality Incentives- Round 1Quality Incentives- Round 1
$1.2M state share and with fed match $1.2M state share and with fed match and private pay amounts to about and private pay amounts to about $3.5M in incentive payments $3.5M in incentive payments
155 applications, 20 projects funded - 155 applications, 20 projects funded - 1 collaborative of 13 facilities so 32 1 collaborative of 13 facilities so 32 facilities in total received incentive facilities in total received incentive payments. payments.
Most incentives 5% of operating rateMost incentives 5% of operating rate Need to show evaluation plan Need to show evaluation plan

Quality Incentives – Round 2Quality Incentives – Round 2
Consortia encouragedConsortia encouraged Evaluation should fit the QIs in useEvaluation should fit the QIs in use Intent to study projects to determine Intent to study projects to determine
the financial impact to the Medicaid the financial impact to the Medicaid budget.budget.
$6.7M state share and with fed $6.7M state share and with fed match and private pay amounts to match and private pay amounts to about $20M in incentive paymentsabout $20M in incentive payments

MN 2007 NH Rebasing LawMN 2007 NH Rebasing Law
NHs will receive cost payments for NHs will receive cost payments for care related costs up to 120% of care related costs up to 120% of group mediansgroup medians
6 groups formed from geography and 6 groups formed from geography and NH typeNH type
8 year phase in with hold harmless 8 year phase in with hold harmless Then, care related payments based Then, care related payments based
on limits from 105% to 125% based on limits from 105% to 125% based on quality scoreson quality scores