Embed Size (px)
Citation preview

Nur Amalina Aminuddin082012100067
NUTRITION AND FLUID THERAPY

30% in surgical patients with GI disease60% in prolonged hospital stay patientsHave higher risk of complications and death
Aim of nutritional support Identify patients at risk of malnutrition Ensure their nutritional requirements are met
MALNUTRITION

Metabolic response to starvation Low plasma insulin High plasma glucagon Hepatic glycogenolysis Protein catabolism Hepatic gluconeogenesis Lipolysis Adaptive ketogenesis Reduced resting energy
expenditure ( 15-20kcal/kg/d)
PHYSIOLOGY

Metabolic response to trauma and sepsis Increased counter- regulatory hormones Increased energy requirements ( 40kcal/kg/d) Increased nitrogen requirements Insulin resistance and glucose intolerance Increased gluconeogenesis and protein catabolism Loss of adaptive ketogenesis Fluid retention

1.Laboratory techniques
Albumin <30g/l : poor prognostic indicator
Immunity Eg.lymphocyte count or skin test for delayed
hypersensitivity Not precise/ reliable/ practical
NUTRITIONAL ASSESSMENT

Weight loss >10% in 6 months
poor outcomeBMI
<18.5 : nutritional impairment
< 15 : increased hospital mortality
Anthropometric techniques Estimate body fat and
muscle mass Indirect measure of
energy and protein stores
Bioelectrical impedence analysis (BIA) Estimate intra- and
extra cellular fluid volume
2.BODY WEIGHT AND ANTHROPOMETRY
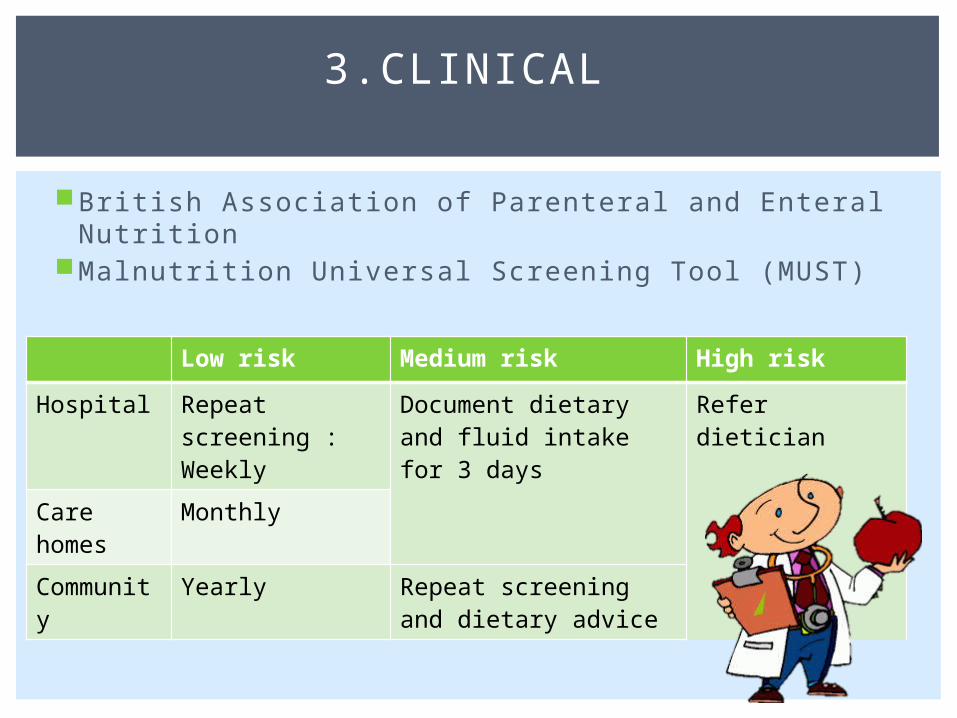
British Association of Parenteral and Enteral NutritionMalnutrition Universal Screening Tool (MUST)
3.CLINICAL
Low risk Medium risk High riskHospital Repeat
screening :Weekly
Document dietary and fluid intake for 3 days
Refer dietician
Care homes
Monthly
Community
Yearly Repeat screening and dietary advice

I f BMI or weight loss cannot be established, use recalled value
I f both, use overal l impression of malnutrit ion Clinical impression or Clothes
becoming loose or loss of appetite or any underlying cause

Average Daily Water Balance
Daily electrolytes requirement (mm/d): Sodium 50-90 Potassium 50 Calcium 5 Magnesium 1
FLUID AND ELECTROLYTES

Nature and volume of fluids administered are determined by: Assessmnet of patient ( pulse,BP,CVP, hydration status,
urine, s.electrolyte and hematocrit) Estimation of loss Estimation of supplement fluids Electrolytes composition
Solution Na K Ca Cl Lactate
Colloid
Hartmann’s 130 4 2.7 109 28NS ( 0.9% NaCl) 154 154Dextrose saline 30 30Gelofusine 150 <1 150 Gelatin 4%Haemecel 145 5.1 6.2
6145 Polygelin 75g/l
Hetastarch Hydroxyethyl starch 6%
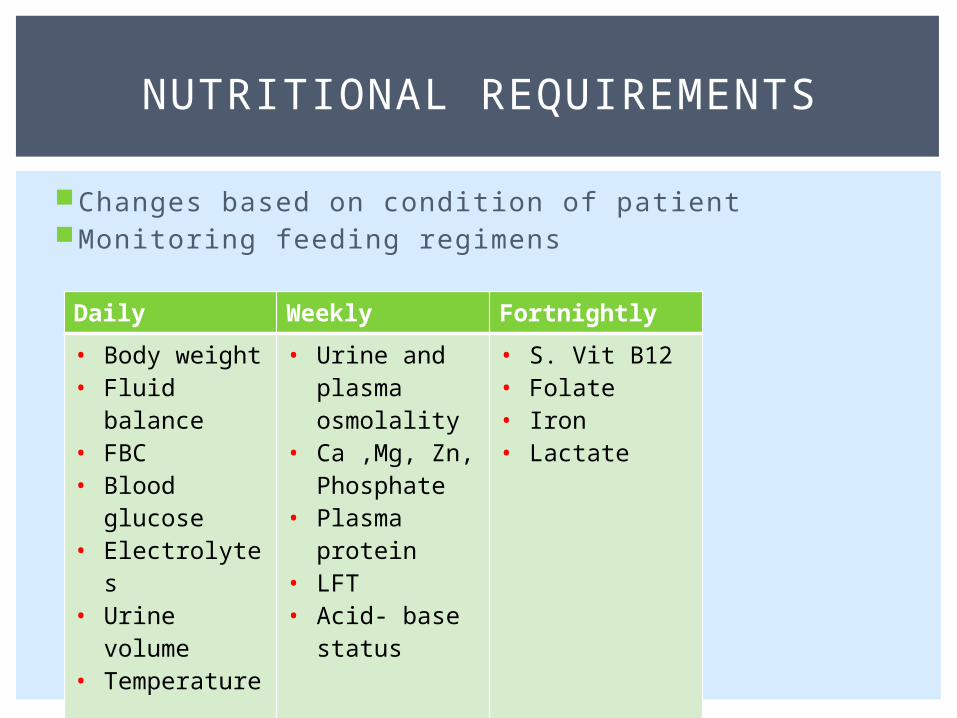
Changes based on condition of patientMonitoring feeding regimens
NUTRITIONAL REQUIREMENTS
Daily Weekly Fortnightly • Body weight• Fluid balance• FBC• Blood
glucose• Electrolytes• Urine volume• Temperature
• Urine and plasma osmolality
• Ca ,Mg, Zn, Phosphate
• Plasma protein
• LFT• Acid- base
status
• S. Vit B12• Folate• Iron• Lactate

Total energy requirements20-30 kcal/kg/d1300-1800 kcal/d
CarbohydratesObligatory glucose
requirements: 2g/kg/dGlucose infusion at
4mg/kg/min
Protein Basic: 0.10-0.15g/kg
Fat Essential fatty acids
(linoleic, linolenic): 100- 200g/w
Given as mixture with glucose at 0.15g/kg/h Minimises metabolic
complications during parenteral nutrition
Reduces fluid retention Increases substrate
utilisation

Vitamins, minerals and trace elements Vit B and C: collagen formation, wound healing B12 supplements for intestinal resection/ gastric surgery/
alcohol dependence Vit A,D,E and K in steatorrhea and in absence of bile
Necessary to optimise amino acids utilisation

Norman William, Christopher, & P.Ronan, Bailey & Love’s Short Practice of Surgery, 25th edition
REFERENCE