Embed Size (px)
Citation preview

Median Nerve Injuries
Dr SD Sanyal

Anatomy
• Mixed nerve (contain motor & sensory fibers).
• Root value: C 5,6,7,8 & T1
• Runs in the median plane of the forearm , so its called median nerve

Anatomy
• Arises in the axilla by joining:
1) Lat Cord of the brachial plexus
2) Med Cord of the brachial plexus
Anatomy: Axilla
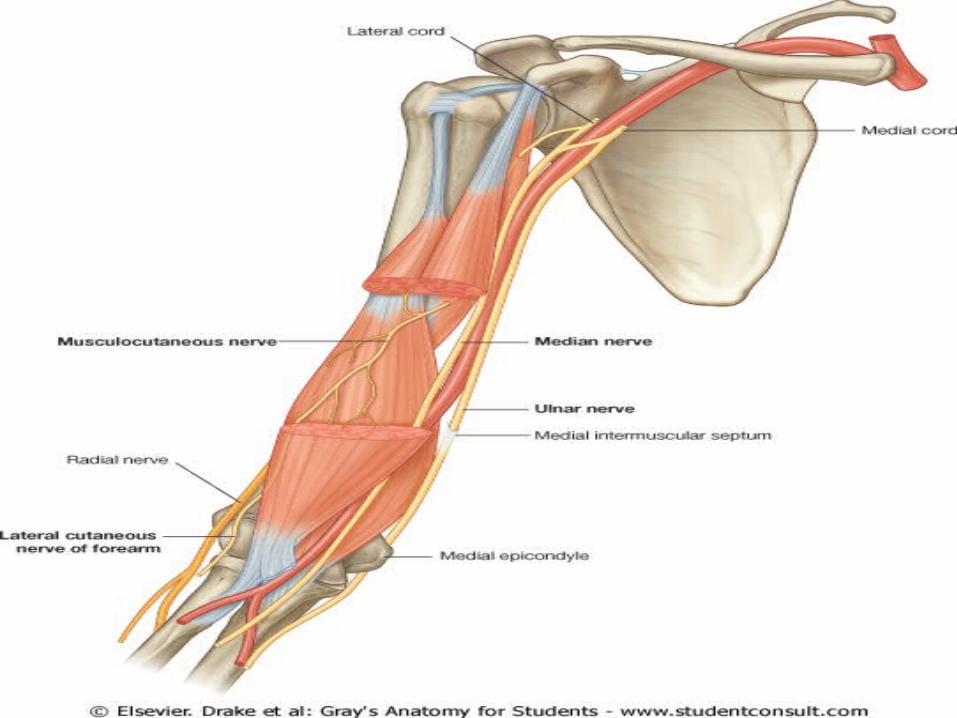
• After being from Lateral Cord Medial Cord of brachial plexus
Runs on the lateral aspect of Axillary artery

Anatomy: Arm
• Continues to run lateral to the brachial artery till the mid-arm
• Crosses the artery anteriorly and passes anterior to the elbow joint into forearm



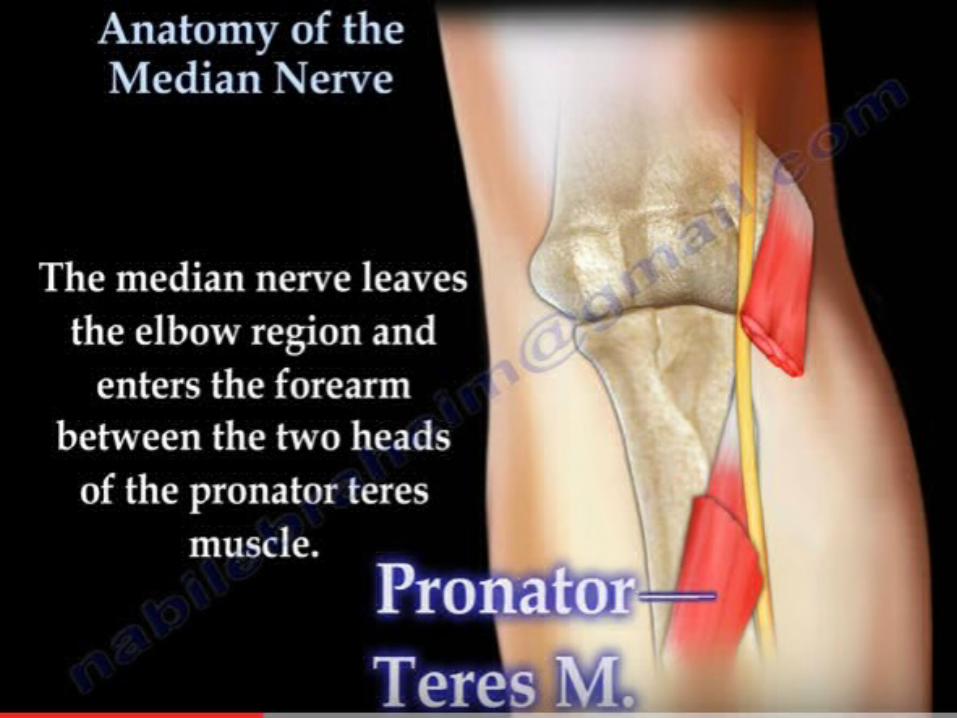
Anatomy: Forearm
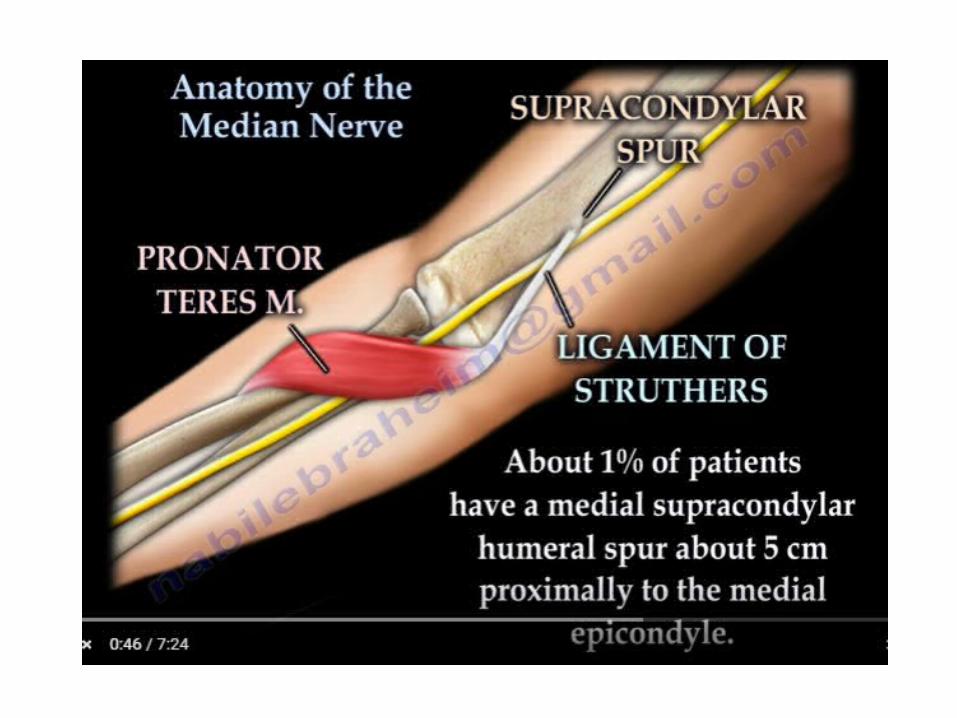
• Enters to the forearm b/w two heads of pronator teres .
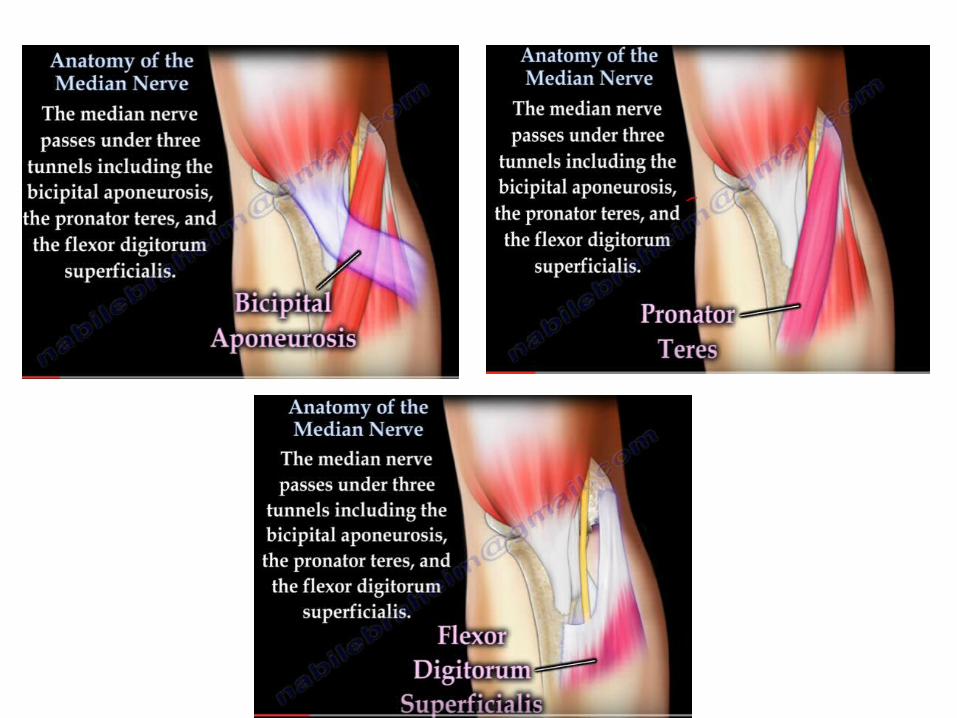
• Runs deep to the fibrous arch of FDS , in proximal 1/3rd
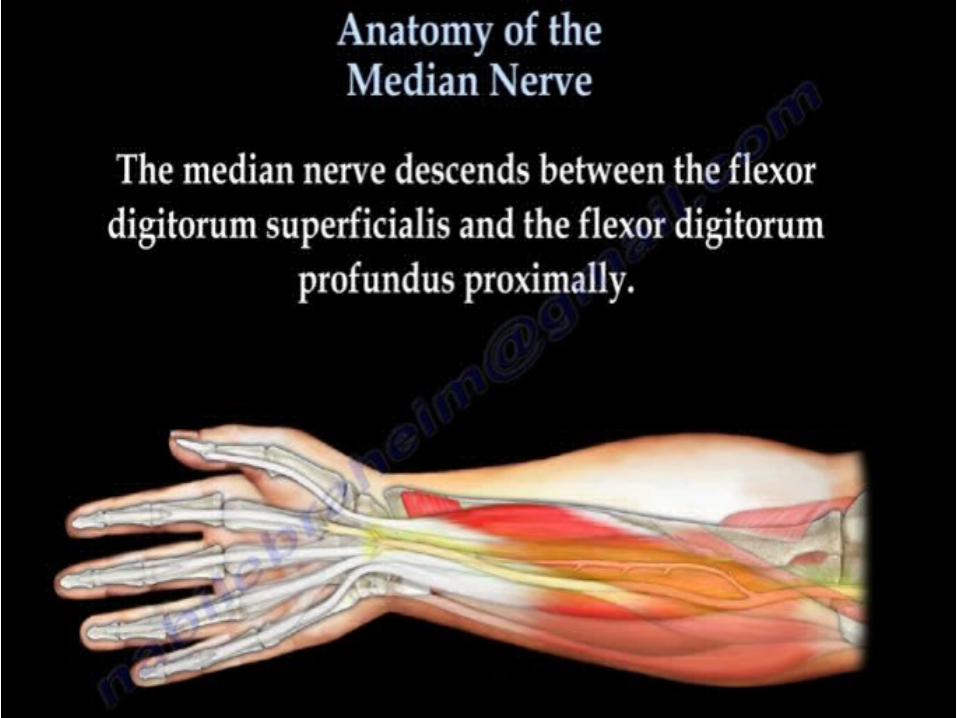
• Mid forearm it descends b/w FDS and FDP
• About 5 cm above wrist , it comes to lie on the lateral side of the FDS , becomes superficial just above wrist



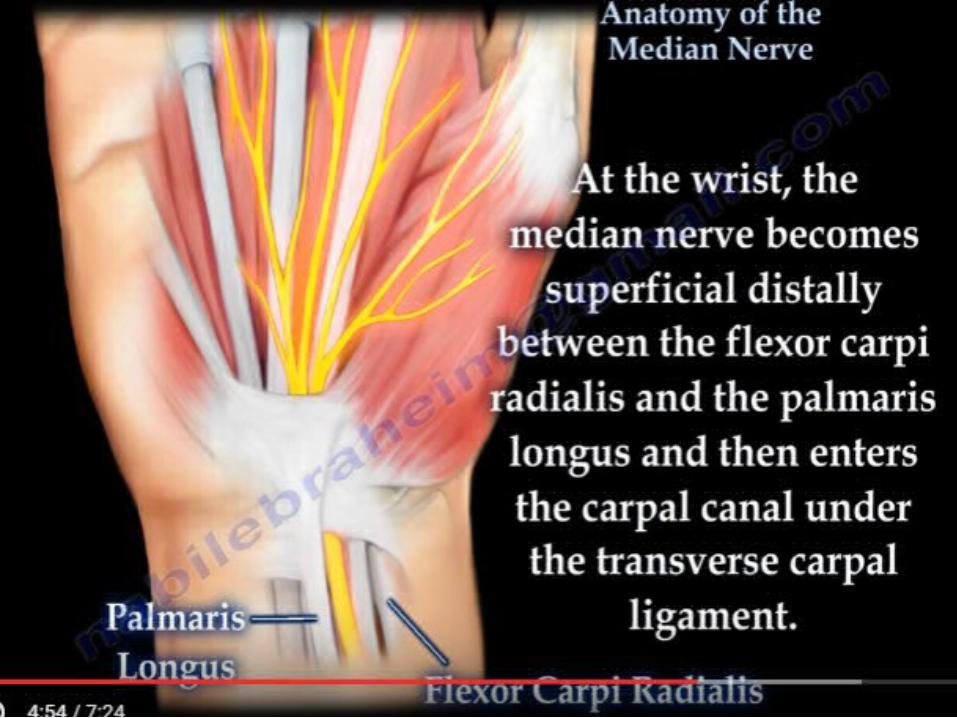

Anatomy: Hand
• Passes deep to the flexor retinaculum and enters the Hand
• Muscular braches supply muscles of Thenar eminence: - abductor pollicis brevis - opponens pollicis - flexor pollicis brevis


Anatomy: Hand
• Divides into 4 to 5 palmar digital branches supplying lateral three and half digit and their nail beds
• Motor braches to the first and second lumbrical muscles





Other branches
• Articular branches: supply the proximal radio-ulnar joint
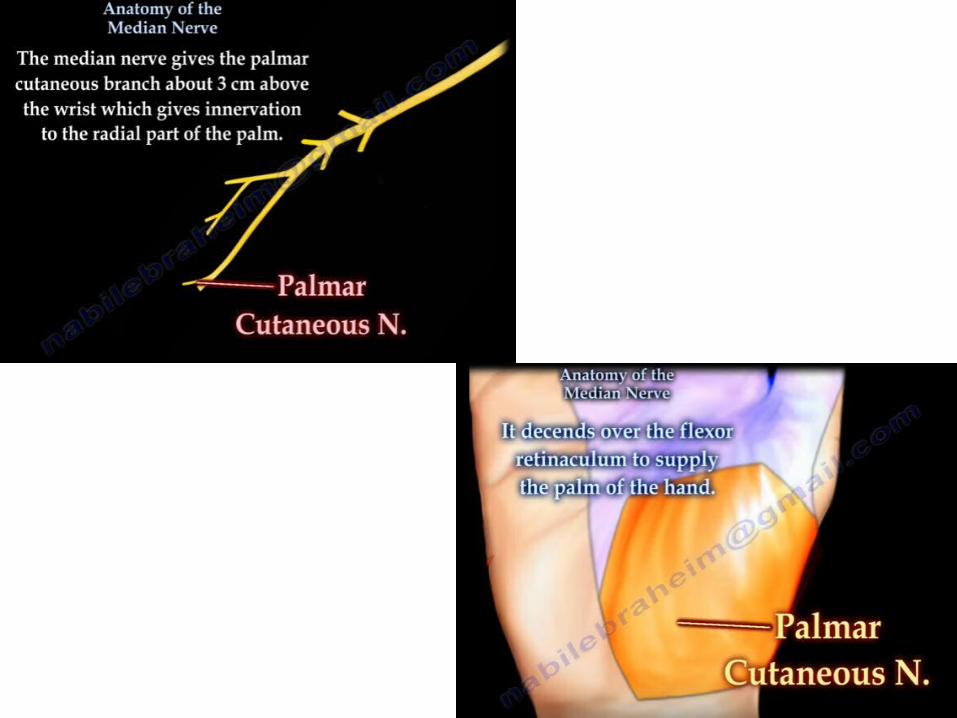
• Palmar cutaneous branch: supplies skin over
thenar eminence


Injuries
• High• Low

High Median Nerve injuries
• Injury proximal to the elbow
• Due to forearm fractures or elbow dislocation
• Stab injuries and GSW’s • Paralysis of all the muscles supplied by the
median nerve in the forearm and hand
Low Median Nerve Injuries• Injury in the distal third of the forearm
• Sparing of the forearm muscles
• Muscles of the hand paralysed
• Anaesthesia over the median nerve distribution in the hand
• Thenar eminence is wasted and thumb abduction and opposition are weak
• Sensation lost over the radial three and half digits and trophic changes may seen
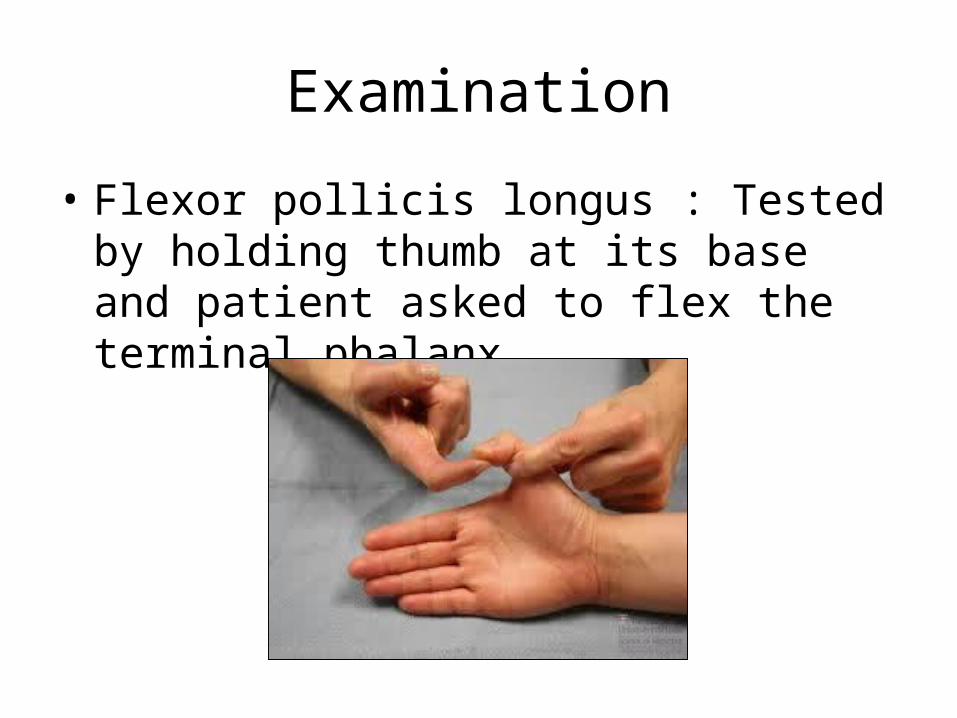
Examination
• Flexor pollicis longus : Tested by holding thumb at its base and patient asked to flex the terminal phalanx

Examination
• Flexor digitorum superficialis & profundus (Oscher’s clasping test) - Patient is asked to clasp the hands , the index finger of affected side fails to flex
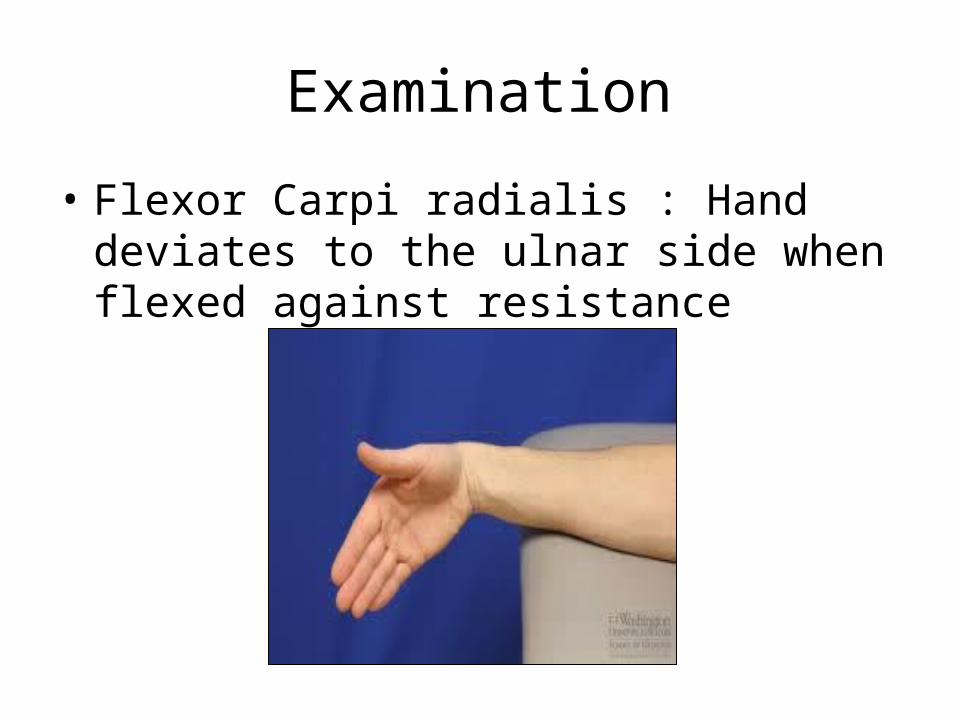
Examination
• Flexor Carpi radialis : Hand deviates to the ulnar side when flexed against resistance

Examination
• Muscles of Thenar eminance:- abductor pollicis brevis (Pen test) - hand laid flat on the table - pen held above the palm and the patient is asked to touch the pen with his thumb

Examination
• opponens pollicis : brings the tip of the thumb towards the tips of other fingers

Opponens pollices

Benedict Sign

Klien Nioh/ OK Sign

Ape Thumb

Principles of Surgical Management1. Direct Injury: Nerve repair2. Compression neuropathies: Decompression3. Long standing cases: Tendon transfersa) Low Median Nerve: - Re-
routing of ring/ middle finger superficial flexor around FCU to APB to aid thumb opposition
b) High Median Nerve: - Suturing of profundus tendons to ring and small finger tendons for restoration of IP jt movts- ECU re-routing and attachment to dorsal radius/ Transfer of biceps insertion from medial to lat radius for weak forearm pronation
Median nerve Compression Syndromes
• Carpal Tunnel• Pronator• Interosseous

Carpal Tunnel Syndrome• Compressive neuropathy as the nerve passes through the Carpal
Tunnel• Causes:
- Idiopathic : Most common- Inflammatory : Rheumatoid Arthritis
: Wrist osteoarthritis- Post traumatic : Bone thickening
- Endocrine : Myxoedema
: Acromegaly- Pregnancy- Gout- Repetitive wrist movts: Typists & Computer users
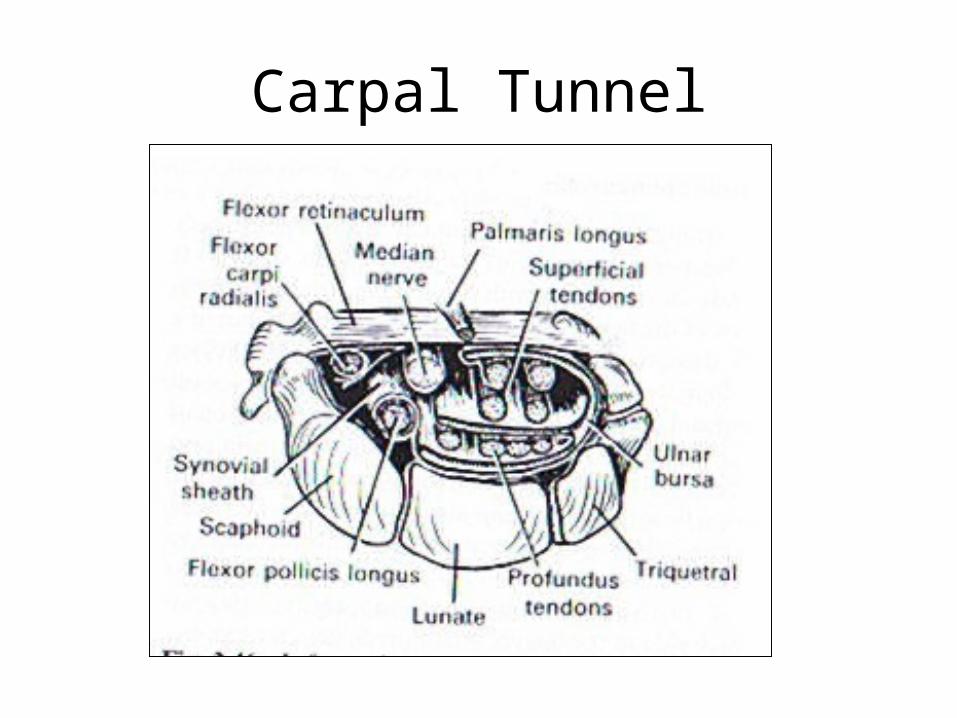
Carpal Tunnel

Symptoms
• Hand and wrist Pain• Paraesthesia • Hypoaesthsia• Sparing of Palmar cutaneous branch supply• Patient wakes at night with burning or aching pain and
shakes the hand to obtain relief and restore sensation• Aggravated by elevation of hand• Thenar atrophy and weakness of thumb opposition
and abduction may develop late
Diagnosis
• History • Clinical examination:
- Thenar wasting- Phalen’s sign- Tinel’s sign- Carpal compression test
• Electro Diagnostic Studies:- Very reliable for evaluation- Atypical cases may be present

Thenar atrophy


Tinel’s Sign
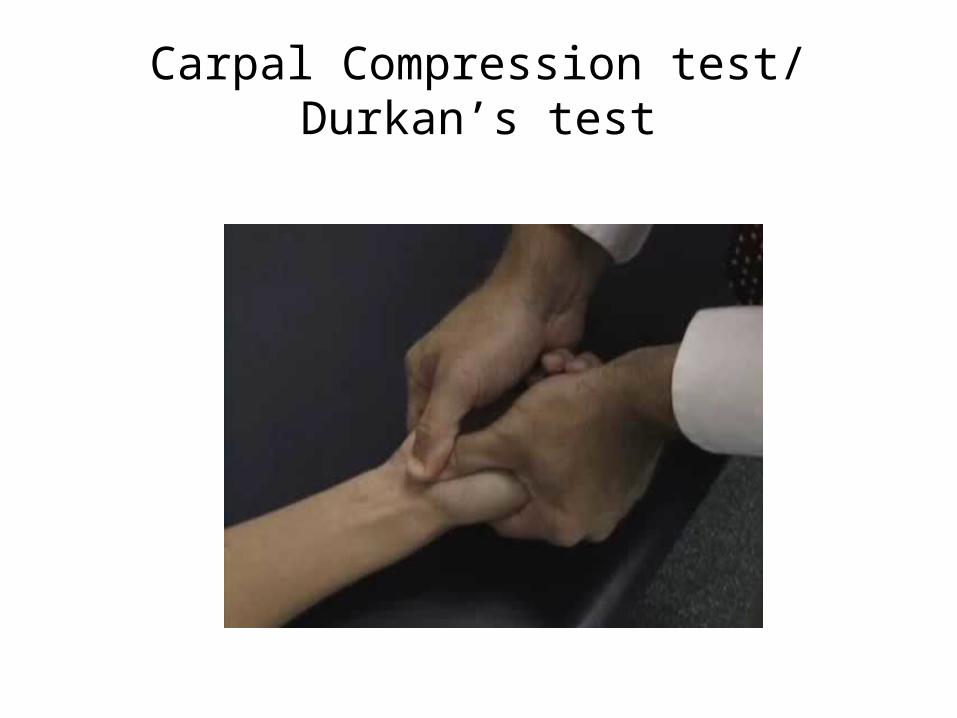
Carpal Compression test/ Durkan’s test
Management
• Splinting – prevents wrist flexion
• Corticosteroid/anesthetic injection
• Surgical decompression:Division of the transverse carpal ligament- Open- Endoscopic




Complications
• Injury to palmar cutaneous/recurrent motor branch of the median nerve
• Hypertrophic scarring
• Hematoma/Arterial injury
• Pillar pain
Pronator teres syndrome
• High Compression neuropathy
• It is rare compared to CTS and AIS
• Misnomer Proximal forearm median nerve compression
Symptoms & signs• Symptoms are similar to those of carpal tunnel syndrome• Sensory disturbances
- Thumb & Index > Middle finger• Night pain is unusual and forearm pain is more common• Hand numbness on gripping• Phalen’s test negative • Double crush phenomena
• Symptoms provoked by resisted elbow flexion with forearm supinated ( tightening of bicipital aponeurosis )
• By resisted forearm pronation with the elbow extended ( pronator tension )

Management
• No relief with steroids• Surgical decompression

Anterior Interosseous Syndrome
• Damage to the Anterior Interosseous Nerve• Pain in the forearm• Weakness of the gripping movement of the
thumb and index finger( unable to make ok sign )
• Causes:- Injury to elbow- Injury during open/closed reduction
Management
• Corticosteroids• Surgery:
- Resection/detachment of deep head of PT

Thank You






![MEDIAN NERVE - Government Medical College and … lectures/Anatomy/UL-median nerve.pdf · MEDIAN NERVE • Formation:from two roots from lateral cord [C(5),6,7]& from medial cord(C8,T1)](https://img.dokumen.tips/doc/110x75/5a7422797f8b9ad22a8bbdcd/median-nerve-government-medical-college-and-lecturesanatomyul-median-nervepdf.jpg)

![MEDIAN NERVE - gmch.gov.in lectures/Anatomy/UL-median nerve.pdf · MEDIAN NERVE • Formation:from two roots from lateral cord [C(5),6,7]& from medial cord(C8,T1) of brachial plexus](https://img.dokumen.tips/doc/110x75/5ed4b477d718f333af5c5484/median-nerve-gmchgovin-lecturesanatomyul-median-nervepdf-median-nerve-a.jpg)




















