Embed Size (px)
Citation preview

Management of diabetes in hemodialysis
patients
Ghada El-KanishyProf. of Internal Medicine
Mansoura Faculty of Medicine

ALTHOUGH DIABETES is the most common cause of ESRD worldwide, accounting for 44% of ESRD patients in the US Renal Data System in 2005,data are scarce on how diabetes should best be treated in patients in ESRD.

•Diabetic patients on dialysis also show a higher morbidity and mortality than non-diabetic dialysis patients.
•Cardiovascular disease is the main cause of mortality in CRF diabetic patients

Good glycemic control predicts better survival of diabetic ESRD patients starting hemodialysis treatment
Diabetes Care 2001 May; 24(5): 909-913
uraemia-associated anorexia
inadequate gastrointestinal glucose absorption
insulin metabolism disorders (IR and reduced insulin clearance)
↑ risk of hypoglycemia
ESKD and dialysis affect drug clearance
Factors influence glycaemic control in diabetic dialysis patients:

Management of diabetes in hemodialysis patients

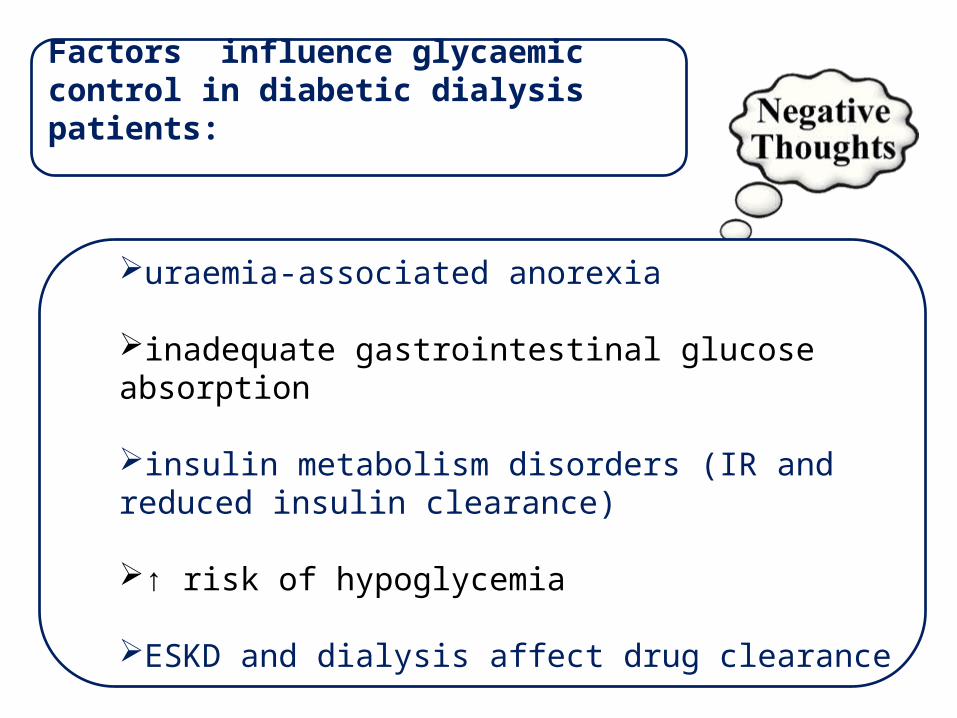
oral hypoglycemic drugs
Challenges in use of OHD in diabetics on HD

Sulfonylureas
Sulfonylureas stimulate endogenous insulin secretion by pancreatic β cells

SulfonylureasPotentially cause hypoglycemia, especially in• High doses• Omission or reduction of carbohydrate intake• Alcohol abuse• Hepatic dysfunction• Malnutrition• Advanced age • Interactions with certain drugs that displace SUs from
their plasma protein-binding sites salicylates, sulfonamides,
vitamin K antagonists, beta-blockers, and fibric acid derivatives

Sulfonylureas

Second generation SU
SU undergo
hepatic metabolism with variable percentage of renal excretion
Sulfonylureas
Glyburide & glimepiride have
relatively longer half-lives active metabolites that are renally excreted
and so are NOT recommended for ESKD.

Glipizide has a short half life of 2-4 hs with little hypoglycemic activity.

Meglitinides
•insulin secretagogues that stimulate pancreatic beta cells
•Short duration of action
Meglitinides• Nateglinide is hepatically metabolized,
with renal excretion of active metabolites which might precipitate hypoglycaemic effects.
• Repaglinide, in contrast, is almost completely converted to inactive metabolites in the liver, and less than 10% is excreted by the kidneys.

Meglitinides Repaglinide is considered a safe option until the
GFR falls to <30 mL/min/1.73 m2 . In advanced renal disease, repaglinide should
begin cautiously, with 0.5 mg daily, to avoid hypoglycemia.

Biguanides• Metformin is not metabolized and 90% is
excreted as the active drug by the kidneys.
• Plasma levels are thus substantially higher in pts with ↓ GFR

Biguanides• Use in non dialysis CKD

Biguanides in HD
Metformin poisoning

Biguanides
lactic acidosis
Rare ; 5 cases per 100,000 patient-years

Thiazolidinediones
Pioglitazone

Benefits and hazards of TZDs therapy
Diabetes, Obesity and MetabolismVolume 15, Issue 11, pages 967-977, 18 APR 2013 DOI: 10.1111/dom.12101http://onlinelibrary.wiley.com/doi/10.1111/dom.12101/full#dom12101-fig-0001

Thiazolidinediones
Fluid retention
• Caution is required in patients in:• compensated heart failure (NYHA class I
or II) • in those at risk of heart failure, such as
patients with previous myocardial infarction
Angina Hypertension LVH significant aortic or mitral valve
disease age greater than 70 years diabetes for more than 10 years.

Thiazolidinediones• In summary
Although ESRD and dialysis do not affect the metabolism of thiazolidinediones, these agents are not recommended in ESRD because of the associated risk of fluid accumulation and precipitation of heart failure.

Alpha-glucosidase inhibitors
• the use of α-glucosidase inhibitors in patients receiving dialysis is avoided because of the lack of long-term clinical trials of these agents in patients with ESRD and diabetes
KDOQI Clinical Practice Guidelines and Clinical
Practice Recommendations for diabetes and chronic kidney disease. Am. J. Kidney Dis. (2007)

Dipeptidyl peptidase 4 (DPP-4) inhibitors
• Limited data suggest that these agents are effective and relatively safe in CKD and ESRD patients.
• Dose adjustments are needed for some agents in this class.
.

Dose adjustment of DPP4i
National Kidney Foundation. KDOQI Clinical Practice Guideline for Diabetesand CKD: 2012 update. Am J Kidney Dis. 2012;60(5):850-886.

2015

Safety• meta-analysis of 59 randomized controlled
trials involving 36,620 patients treated with DPP-4 inhibitors for at least 24 weeks also showed a significant increase in the occurrence of HF compared with the placebo group
Circulation. 2014; 130(18):1579-88.

GLP-1 analogue Exenatide
• exenatide undergoes minimal systemic metabolism and is excreted in the urine.
• No dose adjustment is required if the glomerular filtration rate (GFR) is greater than 30 mL/min
• Exenatide is contraindicated in patients undergoing hemodialysis or in patients who have a GFR less than 30 mL/min

GLP-1 analogueliraglutide
• In contrast to exenatide, liraglutide is not primarily eliminated by the kidney and the pharmacokinetics are independent of kidney function;
– However, liraglutide is not recommended if GFR less than 30 mL/min due to limited experience.

Sodium-glucose cotransporter-2 (SGLT-2) inhibitors
• This therapeutic class has been approved for the treatment of patients with T2DM with an eGFR of ≥45 mL/min/1.73 m2.
• Canagliflozin has been evaluated, showing safety and efficacy in a subset of patients with stage 3 CKD
Am J Nephrol.2014;40((1)):64–74

Because of its urine-dependent mechanism of action, these medications are NOT EFFECTIVE in pts with severe renal impairment
SGLT-2

Oral antihyperglycemic drugs
– Glipizide– Repaglinide– linagliptin

Insulin

Hemodialysis
• use insulin rather than oral agents
• Insulin doses may change substantially during the transition from earlier stages of CKD to dialysis.
• 2005

Insulin dosing in CKD

↓ initial dose of insulin by approximately 50 %, as for nondialysis CKD patients with GFR <10 mL/min.
The dose should be titrated upward, as indicated by blood glucose monitoring
Which isulin is preferred ?

• .
Intensive insulin analogue treatment provided better glycaemic control without long-term hypoglycaemia risk. Although the cost is a disadvantage, insulin analogues can be preferred in selected haemodialysis patients with diabetes mellitus
Nephrol. Dial. Transplant.(February 2006)

Dose adjustments due to impaired renal function should NOT be required for insulin degludec.

Problems with control of DM in patients on HD

• Goals ofglycemic control
• Monitoring ofglycemic control
• Fluctuation of blood glucose levels due to various and opposing effects of ESRD and dialysis.

GOALS OF THERAPY

GOALS OF THERAPY
7 - 8%
based upon the risk of hypoglycemia presence of comorbid conditions.

HbA1c target
relatively young (<50 years) and without
significant comorbid conditions
older patients with multiple comorbid
conditions
7 - 7.5 7.5 - 8

2014
high levels (≥8.5%) are associated with increased mortality risk. Very low HbA1c levels (≤5.4%) also may be associated with increased mortality risk.

MONITORING GLYCEMIC CONTROL
HbA1cGlycated Albumin
(GA)

HbA1c
• Not as accurate among ESRD patients as in the general population due to:
AJKD 2008; 52: 766–777.

Glycated Albumin (GA)
Reflects glycemic control over a much shorter interval (7 to 14 days, compared with 60 to 120 days for HbA1c)
GA measurements may not be reliable in
patients with proteinuria or in those on peritoneal dialysis
.

Glycated Albumin (GA
There are no long-term clinical trials
evaluating the relationship between GA and risk of chronic complications of diabetes
.

•HbA1c in these patients might lead to underestimation likely as a result of the increasing proportion of young erythrocyte by the use of erythropoietin.
•GA provides a significantly better measure to estimate glycemic control in HD patients with diabetes
•In patients on dialysis with anaemia and Hb levels <10 g/l, GA and daily fasting blood glucose levels more accurately reflect glycaemic control than haemoglobin A1c levels
2007

2013
Conclusions
HbA1c (compared with GA and other markers of glycemic control) was most closely associated with mean blood glucose

WHAT IS BETTER AS GLYCEMIC MARKER?

limited dataabsence of interventional outcome studies based on GAexpensive and laborious methodology
•It seems premature to abandon HbA1c in favour of glycated albumin
•HbA1C still remains the cornerstone as follow-up of longer term glycaemic control,
GA

For these reasons, HbA1c is preferred in monitoring glycemic control

Reasonable glycemic control in diabetics on HD is:
• FBG ≤ 140md/dl• PPBG ≤ 200mg/dl• HbA1c () 7-8%

Glucose monitoring

Fluctuation of blood glucose levels

Hyoglycemia

Hypoglycemia• 24-h mean glucose values and 24-h CGM
area under the glucose curve in hemodialysis patients on the day of their treatment is lower relative to nondialysis days, with frequent episodes of asymptomatic hypoglycemia.
Ardebili S et al. Assessing glycemic control in maintenance hemodialysis patients with type 2 diabetes. Diabetes Care2009

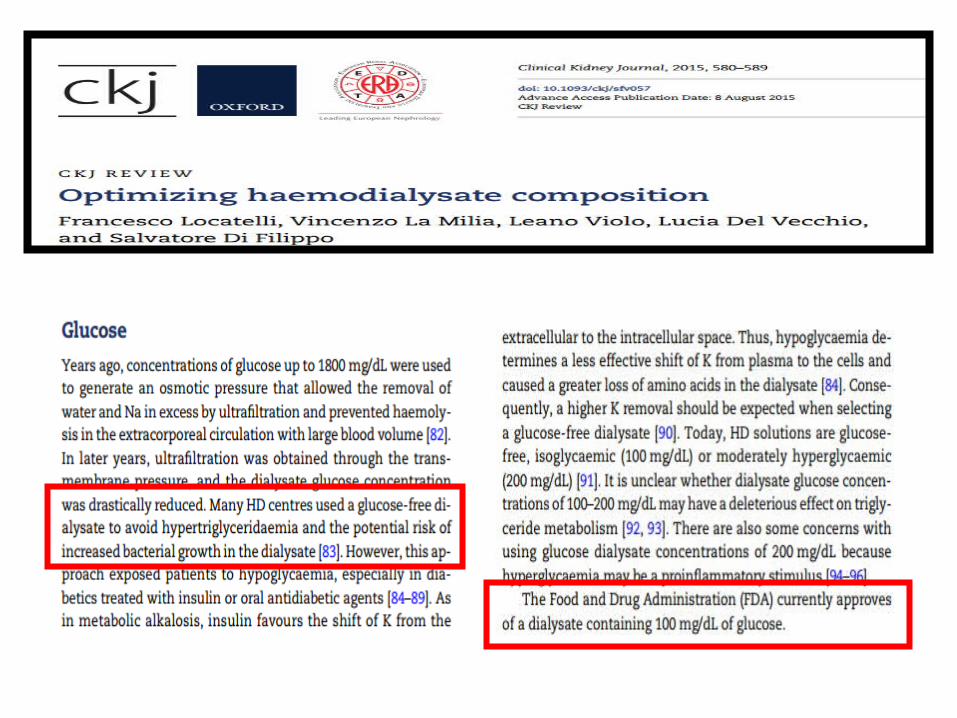
When a glucose-free dialysate is used asymptomatic hypoglycaemia (occurs in approximately 40% of patients with or without diabetes.
Jackson, M. A. et al. Clin. Nephrol. (2000)

Hyperglycemia

Hyperglycemia• causes
– Inadequate insulin dose – noncompliance (with diet or
the insulin regimen) – microvascular disease can
cause erratic absorption of insulin from the subcutaneous tissue, particularly if the patient does not rotate injection sites

Hyperglycemia and ketoacidosis

ketoacidosis• In ESRD
– minimal symptoms, even among those with extreme hyperglycemia
– glucosuria is absent in anuric individuals →hypovolemia and marked hypernatremia do not occur
– marked hyperkalemia which could reach life-threatening severity

ketoacidosis• management
– Insulin infusion is the only treatment required in majority of the patients.
– Emergency hemodialyis may be considered in severe pulmonary edema, profound metabolic acidosis and severe hyperkalemia
Alternating hypoglycemia and hyperglycemia

Mechanisms of haemodialysis-induced hypoglycaemia and haemodialysis-associated hyperglycaemia in patients with diabetes.

• Insulin-treated diabetes patients on hemodialysis showed different glucose profiles between the HD and the FD.
• In particular, in the HD they have had an increased glycemic variability, which may represent an adjunctive risk factor for cardiovascular complications.
Mirani M et al.,Diabetes Technol Ther. 2010.
Inter-day glycemic variability assessed by continuous glucose monitoring in insulin-treated type 2 diabetes patients on hemodialysis
• Significant 25% reduction in basal insulin requirements the day after dialysis compared with the day before.
• No significant change in boluses was observed
Day-to-Day Variation of Insulin Requirements of Patients With Type 2 Diabetes and End-Stage Renal Disease Undergoing Maintenance Hemodialysis
Sobngwi E et al.,Diabetes Care.(2010)


conclusion
•Glycemic control and monitoring in ESRD and HD are complex.
•Patients with ESRD are especially susceptible to hypoglycemia, so diabetic drug therapy requires special caution.
•Diabetic pharmacotherapy in ESRD should be individualized.

conclusion
•For most HD patients with type 2 DM,initial treatment is with insulin, rather than oral agents
• The newer insulins such as glargine and lispro are more favorable than NPH and regular insulin, but they cost more, which can be an obstacle for some patients

conclusion
•If an oral agent is used, the preferred agents are glipizide or repaglinide.
• HbA1c is used to monitor hyperglycemia in patients with diabetes on HD, although HbA1c may not be as accurate among ESRD patients as in the general population