Embed Size (px)
Citation preview

Integrated Manual Therapy & Orthopedic Massage
For Complicated Shoulder Conditions
Assessment Protocols Treatment Protocols
Treatment Protocols Corrective Exercises
Artwork and slides taken from the book Clinical Massage Therapy: A Structural
Approach to Pain Management Published by Pearson Education
By
Author & International Lecturer
James Waslaski LMT, CPT

Integrated Manual Therapy & Orthopedic Massage
For Complicated Shoulder Conditions Today’s manual therapist needs to have multiple skills in order to address a wide variety
of complicated musculoskeletal pain conditions. Specialization in just one modality is
becoming a thing of the past because of limited patient outcomes. This unique total
system consists of orthopedic assessment, clinical reasoning, multidisciplinary and multi-
modality therapies, and precise corrective stretching and strengthening exercises.
Participants will learn to integrate the skills of leading practitioners from the fields of
massage therapy, physical therapy, athletic training, personal training, osteopathic and
chiropractic to restore balance, posture, function and pain free living. Recent clinical
studies will forever change the way manual therapists look at musculoskeletal pain,
muscle-tendon strain pain, and adhesive capsulitis of the shoulder. Manual therapists will
learn techniques to help eliminate pain from shoulder capsule adhesions, shoulder
impingement, rotator cuff injuries, thoracic outlet, including multiple nerve crush
phenomenon, and complicated frozen shoulders. Corrective stretching and strengthening
techniques will be also taught to keep the muscles balanced, and joints aligned for pain
free living. Our Unique 12 Step Protocol will be used throughout this presentation.
Twelve Steps: 1. Client History 2. Assess Active Range of Motion 3. Assess Passive Range of Motion 4. Assess Resisted Range of Motion 5. Area Preparation 6. Myofascial Release/ Compression Broadening 7. Cross Fiber Gliding/Trigger Point Therapy 8. Multidirectional Friction 9. Pain Free Movement 10. Eccentric Scar Tissue Alignment 11. Stretching 12. Strengthening James Waslaski is an Author & International Lecturer who teaches approximately
40 seminars per year around the globe. He’s served as AMTA Sports massage Chair
and FSMTA Professional Relations Chair. He’s developed 8 Orthopedic Massage and
Sports Injury DVDs, and authored manuals on Advanced Orthopedic Massage and
Client Self Care. His new book, Clinical Massage Therapy: A Structural Approach to
Pain Management was published by Pearson Education in 2011. James presents at
state, national and international massage, chiropractic, and osteopathic
conventions including keynote addresses at the FSMTA, World of Wellness, New
England Regional Conference, the World Massage Festival, and Australian National
Massage Conventions. His audience includes massage and physical therapists as
well as athletic trainers, chiropractors, osteopaths, nurses and physicians. He is a
certified personal trainer with NASM. James received the 1999 FSMTA International
Achievement Award and was inducted into the 2008 Massage Therapy Hall of
Fame. www.orthomassage.net

8/3/2013
1
CLINICAL MASSAGE THERAPYA Structural Approach to Pain Management
CHAPTER
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Shoulder Conditions
5
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Chapter Outline
• Twelve-Step Approach to Shoulder Conditions
• Specific Muscle Resistance Tests• General Shoulder Protocol• Pectoralis Major• Pectoralis Minor• Subclavius• Biceps and Coracobrachialis
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Chapter Outline
• Upper Trapezius and Middle Deltoid• Subscapularis• Rhomboids• Triceps and Posterior Deltoid• Scapula Reposition• Supraspinatus and Upper Trapezius• Infraspinatus and Teres Minor• Common Conditions
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Learning Objectives
• Choose the appropriate massage modality or treatment protocol for each specific clinical condition of the shoulder
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Learning Objectives
• Work on the short, contracted muscle groups such as pectoralis major, pectoralis minor, subclavius, biceps,upper trapezius and subscapularis before working on the weak, inhibited antagonists such as triceps,rhomboids, middle trapezius, lower trapezius infraspinatus, and teres minor
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Learning Objectives
• This will ensure:– structural integration—balance of the
muscle groups– that the therapist eliminates the
underlying cause of the shoulder problems before addressing the clinical symptoms

8/3/2013
2
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Learning Objectives
• Restore pain-free shoulder normal joint range of motion
• Restore normal muscle resting lengths in the muscle groups of the shoulder
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Learning Objectives
• Create shoulder stability• Differentiate between soft-tissue
problems caused byMyofascial restrictionsMuscle–tendon tensionMyoskeletal alignment problems
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Learning Objectives
• Differentiate between soft-tissue problems caused by trigger point tension joint capsule adhesions strained muscle fibers scar tissue
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Learning Objectives
• Teach the client self-care stretches and strengthening exercises to perform at home to maintain shoulder structural balance and pain-free movement following therapy
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Precautionary Note
• Do not work on a client with a recent injury (acute condition) exhibiting inflammation, heat, redness, or swelling. RICE therapy (rest, ice, compression, elevation) may be the appropriate treatment in this situation.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Precautionary Note
• This work cannot be performed on clients with severe shoulder conditions like a complete rupture of a muscle, complicated labrum tears, and fractures.

8/3/2013
3
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-1 Shoulder Flexion, 160–180 Degrees.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-2 Shoulder Extension, 50–60 Degrees.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-3 Shoulder Abduction, 180 Degrees.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-4 Shoulder Adduction, 30–45 Degrees.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-6 Shoulder Lateral/External Rotation,80–90 Degrees.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-5 Shoulder Medial/Internal Rotation,90–100 Degrees.

8/3/2013
4
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• When performing PROM, you should always be sensitive to the client’s breathing and patterns of guarding. Your overall confidence, combined with a calming voice, can help the client relax.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• If there is a torn muscle or tendon, it will be treated last, after you have balanced out opposing muscle groups and addressed the problems in the muscle belly leading to the muscle tear.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• Integrated Manual Therapy will stress this statement continually: Never treat a muscle–tendon strain, or a ligament sprain, unless the injured muscle–tendon unit, or injured ligament, is brought back to its normal resting position.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• If the client reports pain after you finish the resisted test, this is not a positive test and the problem may be in the surrounding or stabilizing muscles. The pain must be in the muscle you are testing during the test.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-10 Muscle Resistance Test, Subscapularis.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-11 Muscle Resistance Test, Pectoralis Minor.

8/3/2013
5
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-13 Muscle Resistance Test, Supraspinatus.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-15 Muscle Resistance Test, Middle Deltoid.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-14 Muscle Resistance Test, Infraspinatus and Teres Minor.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• Thoracic outlet syndrome can create symptoms similar to carpal tunnel syndrome. Always look for the source of the pain, don’t just rely on the symptoms.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-55 Thoracic Outlet Syndrome.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-59 Joint Capsule Adhesions.

8/3/2013
6
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Precautionary Note
• If the client tested positive for a muscle–tendon strain, it is highly recommended that you bring that muscle back to resting length, and treat the strain prior to attempting joint capsule work. If the client is guarded due to shoulder discomfort during the capsule work, you will not be able to access and release the deep fascial adhesions inside the shoulder capsule.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• You must change the protocol and perform the joint capsule work anytime during the session if you find a bone-on-bone-like end feel.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-17A Positional Release, Joint Capsule.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-17B Joint Capsule Release, External Rotation.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-17C Joint Capsule Release, Internal Rotation.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-17D Joint Capsule Release, Decompression.

8/3/2013
7
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• Always perform myofascial release before proceeding to deeper, more specific work.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-20A Myofascial Release, Inferior Fibers Pectoralis Major.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-20B Myofacial Release, Superior Fibers Pectoralis Major.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-21 Cross-Fiber Gliding Strokes and Compressive Stretch, Pectoralis Minor.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-28 Subclavius Myofascial Release.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-30A Biceps Myofascial Release.

8/3/2013
8
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-30B Compression Stretch, Biceps.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-30C Cross-Fiber Gliding Strokes.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• Contracting the muscle against resistance to fatigue the muscle prior to the stretch becomes a muscle resistance test, and the client may report pain in a specific area, which is a muscle strain. If so, proceed to multidirectional friction (step 8), pain-free movement (step 9), and eccentric scar tissue alignment (step 10) until the client is pain-free.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-25 Muscle Resistance Test For Pectoralis Minor Strain.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-26 Pectoralis Minor Multidirectional Friction.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-27 Eccentric Muscle Contraction for Scar Tissue Alignment.

8/3/2013
9
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-35 Upper Trapezius Myofascial Release.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-36 Middle Deltoid Myofascial Release.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-40A Subscapularis Myofascial Release.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-40B Downward Scapular Rotation.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-41 Subscapularis Stretch.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• Ischemic muscle pain and trigger points in the middle traps and rhomboids will usually disappear by working and releasing the pectoral muscles, subscapularis, and upper trapezius. This creates balance around the scapula by relaxing the painful, weak, inhibited rhomboids and middle and lower trapezius.
8/3/2013
10
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• There are no stretching exercises for these muscles as they are weak and inhibited. They need to be strengthened. See the Client Self-Care Manual or Corrective Stretching and Strengthening DVDs at www.orthomassage.net.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
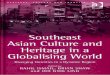
Figure 5-44A Myofascial Release, Triceps.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-44B Myofascial Release, Triceps and Posterior Deltoid.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-44C Myofascial Release of Posterior Deltoid, Middle Trapezius, and Push Erector Spinae onto Spine.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-45A Downward Scapular Rotation.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
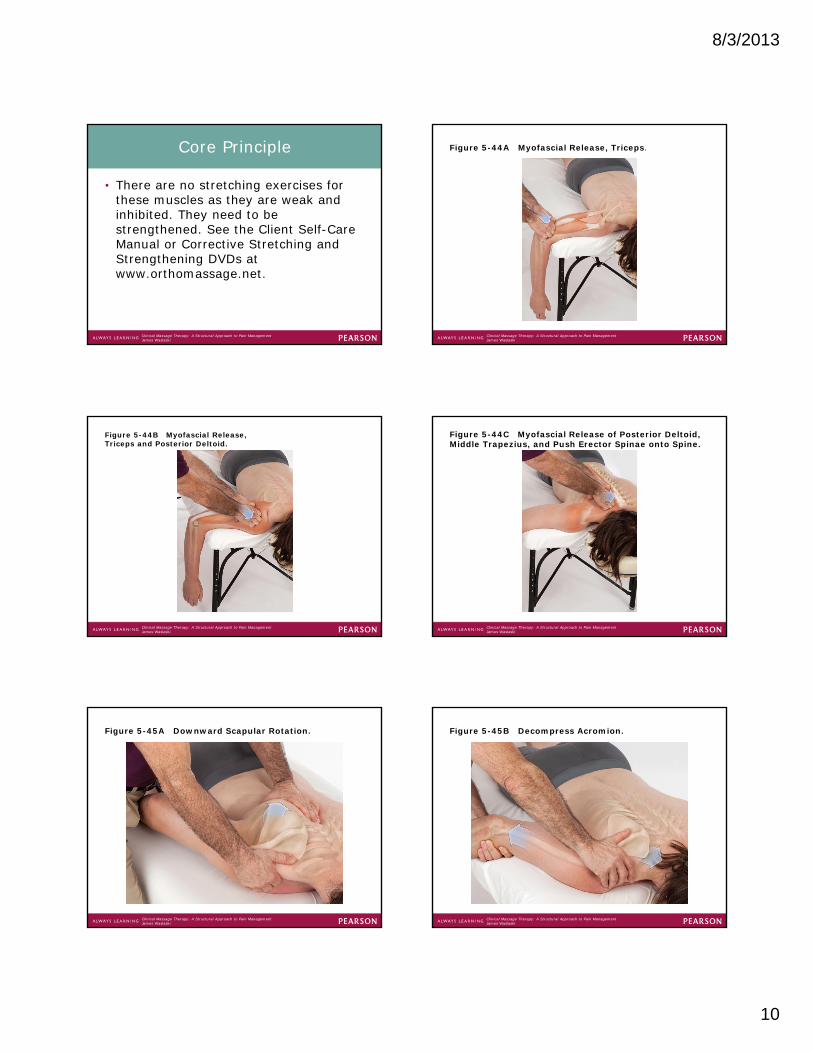
Figure 5-45B Decompress Acromion.

8/3/2013
11
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• For effective treatment of supraspinatus impingement and resultant supraspinatus tendinosis, it is imperative to release the pectoralis minor, upper trapezius, and tight subscapularis muscles before working the supraspinatus.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-46 Cross-Fiber Gliding Strokes and Trigger Point Work, Supraspinatus.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-48 Supraspinatus Muscle Resistance Test.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• If there is not a muscle–tendon strain or ligament sprain, multidirectional friction would not be part of the treatment.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-49 Supraspinatus Multidirectional Friction.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• The greatest error during the eccentric alignment procedure is being too aggressive and not keeping the technique pain-free each time. Too much force in opposing directions can cause a new injury or reinjure the site.

8/3/2013
12
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-50 Supraspinatus Eccentric Muscle Contraction.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-51 Infraspinatus and Teres Minor Myofascial Release, Cross-Fiber Gliding Strokes and Trigger Point Work.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• Remember, it is not suggested that you stretch the rhomboids, infraspinatus, and teres minor muscles, as they are weak, inhibited, and eccentrically contracted and do not need to be stretched any further. There are exercises to strengthen these muscles in the client self-care section at the end of the chapter.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-52 Infraspinatus/Teres Minor Muscle Resistance Test.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-53 Infraspinatus Multidirectional Friction.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-54 Eccentric Muscle Contraction,Infraspinatus and Teres Minor.

8/3/2013
13
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-42 Myofascial Release, Rhomboids.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-43 Reduce Forward Thoracic Curves.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Stretching (Client Self-Care)
• Goal: for the client to perform stretches suggested and demonstrated by you to create normal muscle resting lengths in shortened or contracted muscle groups.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-62 Pectoralis Major Stretch.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-63 Pectoralis Minor Stretch.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-64 Properly Stretch Pectoralis Minor into Doorway.

8/3/2013
14
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-65 Subscapularis Stretch.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Strengthening (Client Self-Care)
• Goal: to strengthen weak, inhibited muscle groups around a joint creating muscle balance throughout the —structural integration.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Core Principle
• The client must stretch the tight, contracted muscles before strengthening the opposing weak, inhibited, or overstretched muscles.
Clinical Massage Therapy: A Structural Approach to Pain ManagementJames Waslaski
Figure 5-66 Rhomboid Strengthening.