Embed Size (px)
DESCRIPTION
Judy Deimel, Nurse Practitioner (Cognitive Health), Northern Adelaide Nurse Practitioner Project delivered this presentation at the 2013 Developing the Role of the Nurse Practitioner conference. The event is designed for organisations and managers looking to better understand, utilise and grow the role of the nurse practitioner in their health service. For more information about the annual event, please visit the conference website: http://www.healthcareconferences.com.au/nursepractitionersconference
Citation preview
The Northern Adelaide Nurse
Practitioner Project
A Cognitive and Culturally
Sensitive Response to Residential
and Community Aged Care
Judy Deimel NP
Overview • Northern Adelaide Nurse Practitioner Project (NANPP)
• Service providers (1) Helping Hand, (2) ACH Group and (3) Aboriginal Elders and Community Care Services
• Philosophy of respecting culture and cognition
• Nurture, nature and mentoring the nurse practitioner
• Collaboration for successful planning, evaluation & sustainability
– Service archetype
– Key performance indicators
– Barriers and facilitators
– Financial viability
• Conclusion

Background Project Aims
• DoHA funded “Nurse Practitioner Aged Care Models of Practice”
• Improve timeliness and access to care for the most vulnerable and disadvantaged older people i.e.
– Aboriginal and Torres Strait Islanders;
– Individuals with dementia and/or mental health issues;
– Acute illness or acute exacerbation of chronic conditions;
– At risk of hospitalisation;
– Palliative care
• Test the best use of Nurse Practitioner (NP) skills and expertise in aged care

Background Project Aims
• Test sustainable funding models for Nurse Practitioners in aged care
• Identify facilitators
• Overcome barriers to Nurse Practitioners in aged care
• Streamline care delivery for older people when transiting from/to aged care, general practice and acute care

Helping Hand Aged Care
• Residential Aged Care Facility (RACF)
– Ingle Farm 96 places (16 dementia secure), 2 respite, 6+ Transitional Care Packages (TCP)
• Community
– Healthy Ageing Clinic
Commercial Road Salisbury
Coordinators, Allied Health and
NP office

Helping Hand – Gaps and Windows • RACF
– Ingle Farm x 5 General Practitioner meet and greet – GP suggestions = INR, unstable Type 2 Diabetes, Behavioural & Psychological Symptoms of Dementia (BPSD), delirium, antipsychotics, staff education, 1 x “show me your Scope of Practice (ScOP)”
– Ingle Farm weekly intervention meeting
– Orientation week needed to break down the wariness to effect resident review and handover teaching sessions on delirium
• Community
– Consumers with cognitive impairment
no diagnosis; behavioural changes
– Education
ACH Group
• ACH Group already has NPC
• RACF
– Highercombe, Hope Valley 120 places + 15 TCP
– Milpara, Rostrevor 92 places
• Community
– Community East, Newton: Nursing, Care Coordinators, OT, physiotherapist, TCP, DVA, community packages

ACH Group – Gaps and Windows
• RACF
– Emphasis on active ageing ‘Partners in Positive Ageing’ model
– Supportive Residential Services Manager (RSM)
– Transition Care Program – declined NP support
– Early Intervention Working Party 1/12 meeting keen for NP input, source for resident referrals;
– Antipsychotic audit; delirium education
– GP mentor identified; 1 x indemnity discussion
• Community
– Allied Health receptive, TCP RN

Aboriginal Elders Village and Community Care
• Residential
• Aboriginal Elders Village Davoren Park
23 residential places
– Enrolled Nurses and Care Workers (CW) +++, Registered Nurse (RN) 1/7, Activity Coordinator
– 2 GPs, unused examination room (now NP room)
• Community
• Aboriginal Home Care Bowden
– 53+ HACC clients
– Coordinators and CWs +++
Aboriginal Elders – Gaps and Windows
• Residential Identified Gaps
– TRUST and CULTURAL RESPECT
– Systematic resident review (ScOP)
– Education
• Community
– HACC = opportunity for early intervention ,not yet requiring packaged care
– Funding for day respite with potential for NP clinic
– Possible referrals from Muna Paiendi Primary Health Care Service Elizabeth Vale
– Education

Essential Requisites - Cognitive and Cultural Sensitivity
Nurse Practitioner Cognitive Health
Nurse Practitioner Candidate Primary Health Care Gerontology
Aboriginal Elders &
Community Services
Helping Hand Aged
Care
ACH Group

NP Cognitive Health ScOP - Judy Deimel
Declining Memory
Dementia
Delirium
Depression
• Healthy brain ageing
• Comprehensive assessment; Dx/DD
• Living well with dementia PWD/carer
• BPSD - recognisable, understandable, and treatable
• Prevention / diagnostic assessment
• Multi-component non-pharma/pharma management
• Education – person with delirium, staff, family
• Rapport and assessment
• Dx defined by DSM-IV
• Cognitive Impairment, dementia & phenomenology of depression

ScOP Donna Preston
Primary Health Care Gerontology
Person-centred
care Mobility, vigour and self-care
Nutrition
Infections
Dementia
Delirium Depression
Continence
Medication
Skin integrity
Chronic complex
needs

Working Across 3 Organisations Nurturing the NP Schedule
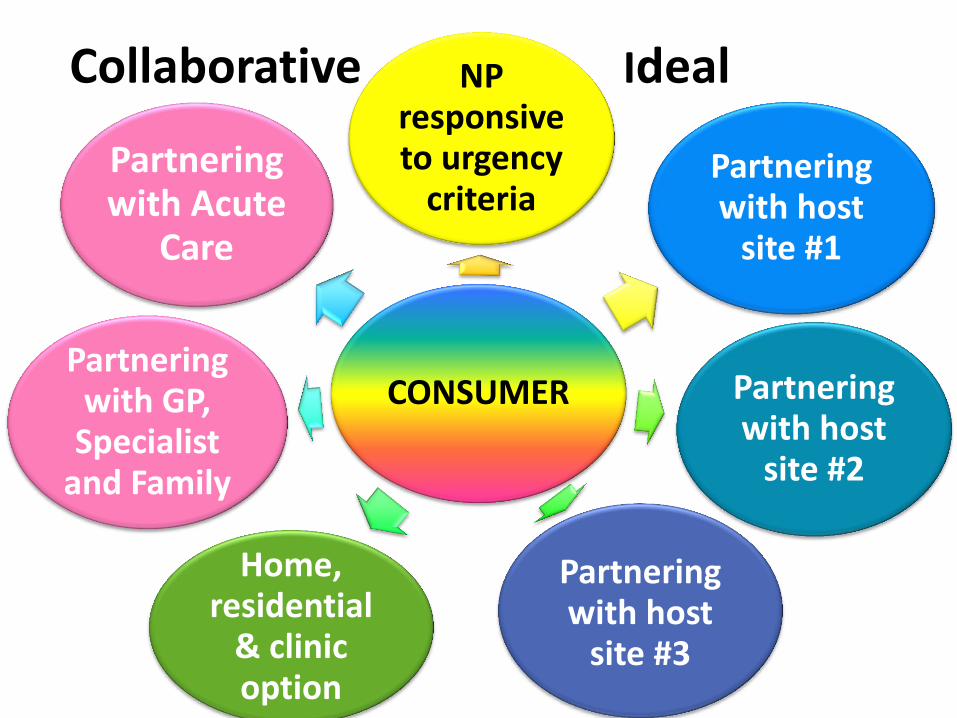
Collaborative Ideal
CONSUMER
NP responsive to urgency
criteria Partnering with host
site #1
Partnering with host
site #2
Partnering with host
site #3
Home, residential
& clinic option
Partnering with GP,
Specialist and Family
Partnering with Acute
Care

Collaborative Reality
• Medical mentoring drawn-out due to project lead change NP initiated resolution
• Geriatrician / Specialist – referral blockers meetings without achieving outcomes 6/12 in NP initiated resolution DBMAS Geriatrician
• GPs letters NPs practice visit informal meeting on site 5/12 later GP Clinic/Round
• Healthy suspicion from some nurses, Care Worker +ve
• Community slow on uptake education sessions
• Forged links with 3 Emergency Departments +ve

Marketing on a Budget

Service Archetype Referral Guidelines
Referral Criteria
1. Client meets NP ScOP
2. Age
3. Catchment Area
4. Treatment (I.E. NP can provide evidence based treatment/ intervention that referrer cannot provide themselves
5. NANPP Referral form completed with sufficient information to enable triage

Service Archetype Referral Form

Referral Pathways
• Helping Hand, ACH Group, & Aboriginal Elders
• Residential / community
• TCP
• GP, SAAS, Geriatric Area Service, nursing, allied health, client, family
Triage
• Nurse Practitioners
• Project Facilitator
• Dedicated email, mobile numbers, fax number
• Meeting ScOP +/- referee notified
• Meeting ScOP client review via:
• Telephone +/or clinic response
NP Assessment
• Consent process
• Comprehensive assessment
• Report sent to referee, GP +/- specialist, family
• Referral to other services (outside NP ScOP)
• Client follow-up short and long term/discharge
• Medi+Assist evaluation

NP Clinical Report
•ISBAR format •Information
•Symptoms
•Background
•Assessment
•Recommendations

Key Performance Indicators (KPI) • Identify best use of NP skill set
– Appropriate, safe, timely and accessible
• Data capture
– – database (location, name, age, sex, ethnicity, first language, referral – reason, date, referee (e.g. Nurse, GP, GP round), date seen, NP name, Medicare, NP referrals, Length of service, date of follow-up, hospital avoidance, referral closed, time for report writing
• Transitioning between RACF, home and acute care
• Identify barriers and facilitators to service delivery
• Education, mentoring, clinical expertise for other HP
• Feedback clinical care/education client, staff and family

KPI Clinical Leadership
• Education: Delirium, Cog Assessment, Dehydration
• Research Projects:
– Audit: Antipsychotic prescribing in dementia audit
– Audit: RACF Dementia diagnosis audit of brain imaging
– Project: Hospital Avoidance
– Project: End of Life Dementia Care (DTSC Palliative Care) and QOL-MB (Quality of Life – Melva Brock)
– Project: NP INR Protocol and Guidelines
• Committees: Aboriginal Elders Dementia Respite
• Publishing: Gentian Violet in Wound Treatment
Northern Adelaide Nurse
Practitioner Satisfaction Survey

Referee & Client Contact Source

Reason for Referral

Location for NP Assessment & Review

6/12 Referral Numbers and Gender

6/12 Evaluation – Age and Ethnicity

Barriers and Facilitators
• Nursing peers
– some suspicion with new NP role
• General Practitioners
– NP recommendations not always welcomed/applied
• Specialist
– reluctant to attend RACF clients
• RACF Health facility – lack of NP role awareness despite letters & orientation – NPs learning the ropes e.g. who what where and why – Insufficient documentation of medical history
• Community - slow on the uptake

Barriers and Facilitators
• NP Project Facilitator Michelle Hogan RN
• NP service information – GP and site letters, brochure
• Setting aside sufficient time for orientation, soft & subtle
• Setting up a referral pathway
• Support from GPs, attending rounds, phone contact
• ScOP and mini version at RACF
• Attending multi-D meetings
• Formal reports in ISBAR format
• Education for staff and clients
• Education resources e.g. delirium, hydration
• Christmas cards; project email updates
Michelle Hogan

The Future - Financial Viability
• Key assumptions - the majority of clients require item numbers 82210 x3 and 82215 x3 reflecting care complexity and patient acuity
• Service sustainability – require average client through put on a daily basis of 6 - 8 MBS clients along with RACF co-payment
• Future
o Secure funds via another project initiative?
o Combined RACF CN wage with MBS remuneration?

Conclusion • NPs working in RACF must have philosophy espousing cultural and
cognitive sensitivity
• Allocate sufficient time for NP orientation to service
• For a successful recipe to develop the NP role - add large scoops of nurturing and mentoring for the person that is the NP
• NPs in aged care address skilled workforce issues where the predominance of RACF workforce are care workers
• NPs improve resident and staff education access
• NPs add value to collaborative case management, care coordination and research findings
• Marketing can be achieved on a low-cost budget
• Collaboration takes time, persistence & persuasion
• Maintain a comprehensive database for KPI and QA
• NP fiscal viability cannot be achieved with MBS remuneration alone

Thank you





























