Embed Size (px)
Citation preview

หลักการและแนวคิดเรื่อง “ความปลอดภัยของผู้ป่วย” ผศ.นพ.บวรศม ลีระพันธ ์
การปฐมนิเทศนักศึกษาแพทย์ชั้นปีที่ 6 (ศิษย์แพทย์รามาธิบดี รุ่นที่ 46) คณะแพทยศาสตร์โรงพยาบาลรามาธิบดี ม.มหิดล ประจำปีการศึกษา 2558
28 เมษายน 2558 Pix source: Kittichai Sareetho “Health care on bicycle” (PMAC 2015 World Art Contest, 14-17 years old)
Presentation Outline
Pix source: online.wsj.com
1. ทำไมแพทย์ต้องเรียนรู้เรื่องความปลอดภัยของผู้ป่วย? 2. ความผิดพลาดที่พบบ่อยในกระบวนการดูแลผู้ป่วยคืออะไร?
และเกิดขึ้นได้อย่างไร?
3. ในฐานะแพทย์ เราจะมีกลไกเพื่อป้องกันการความผิดพลาดในกระบวนการดูแลผู้ป่วยเหล่านี้ได้อย่างไร?

Patient Safety: What & Why
Pix source: online.wsj.com
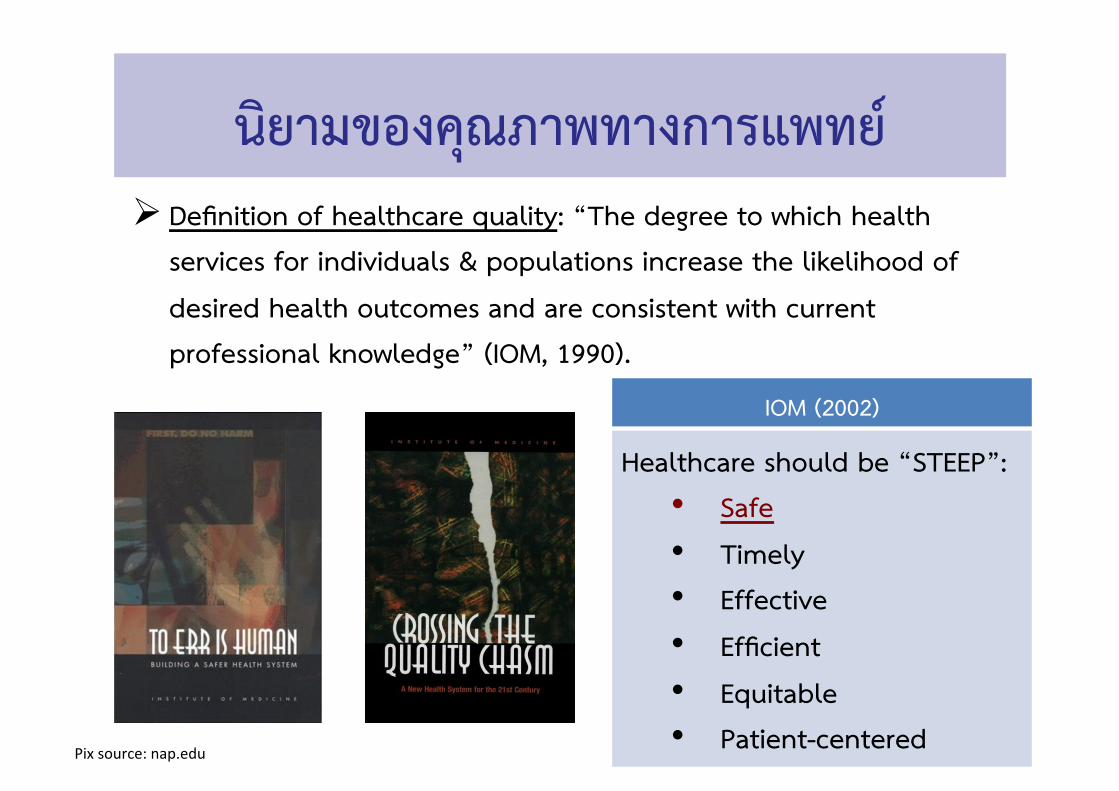
นิยามของคุณภาพทางการแพทย ์
IOM (2002)
Healthcare should be “STEEP”: • Safe
• Timely • Effective
• Efficient
• Equitable • Patient-centered
Ø Definition of healthcare quality: “The degree to which health services for individuals & populations increase the likelihood of
desired health outcomes and are consistent with current professional knowledge” (IOM, 1990).
Pix source: nap.edu

• ความปลอดภัย (Safety): ได้แก่ การออกแบบระบบบริการสุขภาพให้สามารถป้องกันความผิดพลาดทางการแพทย์ (medical errors) หรือหลีกเลี่ยงการบาด
เจ็บของผู้ป่วยซึ่งเกิดจากการได้รับบริการสุขภาพ (iatrogenic injuries)
Quality as Safety
Source: Modified from IOM (2001); Pix source: thieme-connect.de/ejournals; tumblr.com

Training in Quality & Patient Safety
Pix source: www.who.int/pa5entsafety/en/

Training in Quality & Patient Safety
Pix source: www.hms.harvard.edu/hfpsq/

Source: www.hopkinsmedicine.org/armstrong_ins5tute
Training in Quality & Patient Safety

Source: residency.medicine.duke.edu/duke-‐program/training/management-‐and-‐leadership
Training in Quality & Patient Safety

Pix source: bbc.co.uk/bitesize/standard/biology
หลุมพราง (Pitfalls) ในกระบวนการดูแลผู้ป่วย
ความผิดพลาดทางการแพทย ์(Medical Errors)

ความเสี่ยงในโรงพยาบาล
Source: Amalber5 et al. (2005): Pix source: focusedehs.com; alexhibbert.com

Pix: B Leerapan. Lutsen Mountain, MN. Oct 2009.
ฤดูใบไม้ร่วง!

Examples of Common Medical Errors
Diagnostic Errors • Cognitive errors • Issues in communication/info flow
Transition and Handoff Errors • Person-to-person • Site-to-site handoff
Hospital-associated Infections • Ventilator-associated pneumonia • Central line-associated bloodstream
infections • MRSA Infections
Preventable Complications/AEs • Pressure ulcers • Falls • Delirium • Venous Thromboembolism
Surgical Errors • Wrong-Site/Wrong-Patient • Retained Sponges and instruments
Medication Errors • Wrong patient, wrong route,
wrong dose, wrong time, wrong drug

Pix source: kevin.lexblog.com
“แค่ทำหน้าที่ตามมาตรฐานวิชาชีพให้ดีก็พอแล้ว”

“แค่ทำงานแบบมืออาชีพไม่เพียงพอหรือ?”
Pix source: devastatecharlie.blogspot.com; uboat.net; strangecosmos.com; historylink101.com

“แค่ทำงานแบบมืออาชีพไม่เพียงพอหรือ?”
Pix source: devastatecharlie.blogspot.com; uboat.net; warbirdinforma5onexchange.org; pwencycl.kgbudge.com
Pix source: airportjournal.com; pwencycl.kgbudge.com
การพัฒนา (ระยะสั้น)

Pix source: virtualphalcon.blogspot.com; canitbesaturdaynow.com; science.howstuffworks.com
การพัฒนาอย่างยั่งยืน (ระยะยาว)

Pix source: www.be2hand.com; www.descoinstruments.com
การพัฒนาอย่างยั่งยืน (ระยะยาว)

Modified from: Leap (1994)
สาเหตุของความผิดพลาดทางการแพทย์ (Causes of Medical Errors)
Cognitive Errors (“Slips”)
Cognitive Errors (“Mistakes”)
Latent Errors
• Habit • Interruptions • Hurry • Fatigue • Anger • Anxiety • Boredom • Fear
• Biases memory • Overemphasis on
discrepant • Availability of heuristic • Confirmation bias • Overconfidence • Coning of attention • Reversion under stress
• Design of work that exceeds the capacity of the human brain
• Condition of work that generate known causes of errors
• Poorly design & maintenance of equipment
• Inadequate training
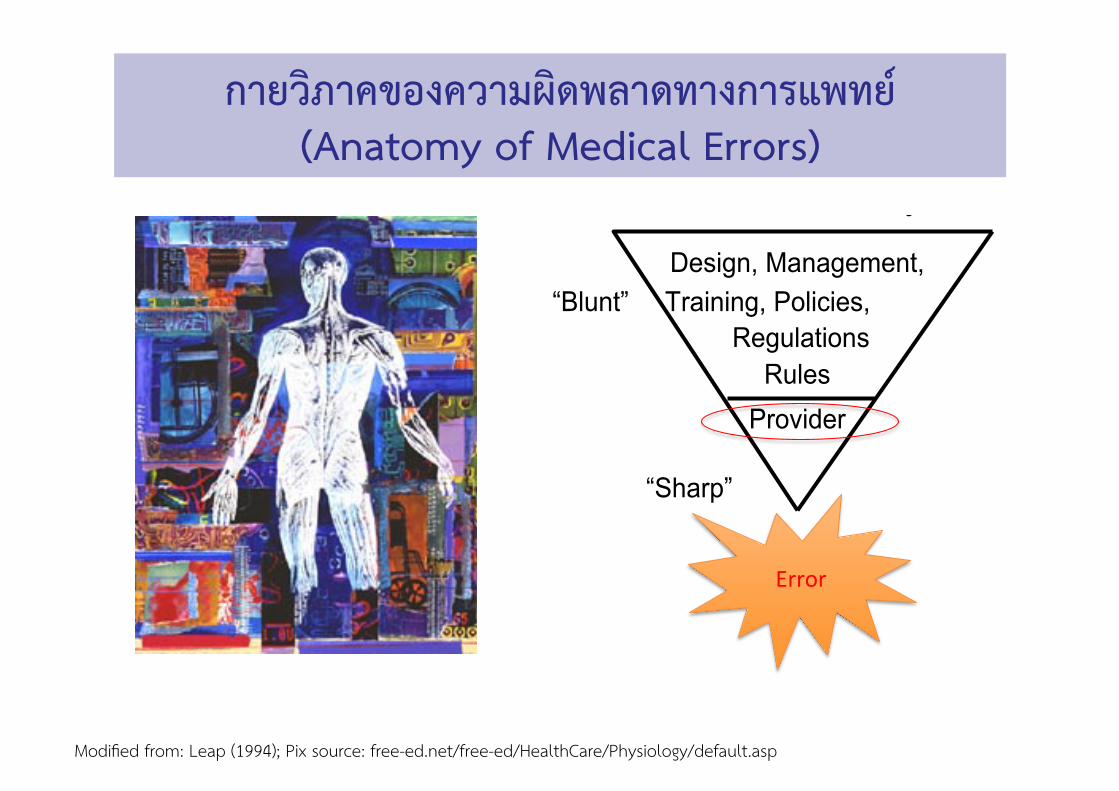
Modified from: Leap (1994); Pix source: free-ed.net/free-ed/HealthCare/Physiology/default.asp
5
The Real Word
Healthy appearing decrepit 69 year old male, mentally alert but forgetful
The skin was moist and dry.
Occasional, constant, infrequent headaches.
Patient was alert and unresponsive
Rectal examination revealed a normal sized thyroid.
She stated that she had been constipated for most of her life, until she got a divorce.
Levels of Safety
Design, Management, “Blunt” Training, Policies,
RegulationsRules
Provider
“Sharp”
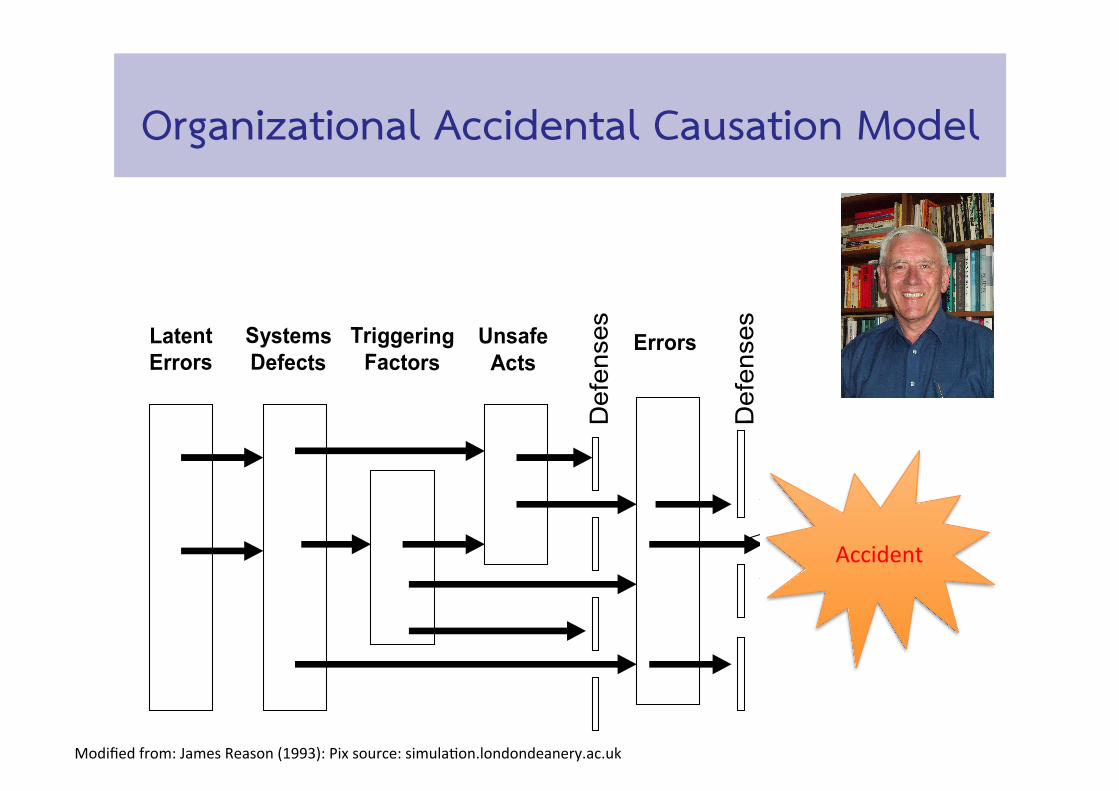
Accident Causation Model
ACCIDENT
Latent Errors
Systems Defects
Triggering Factors
UnsafeActs
Def
ense
s
Errors
Def
ense
s
Contributing Factors (Vincent)
z Work environmentz Team factorsz Individual (staff) factorsz Task factorsz Patient factorsz Organization and Managementz Institutional context
Accident Causation Model
ACCIDENT
Latent Errors
Care Managem’t
Problem
Def
ense
s
Def
ense
s
Contributory Factors
J.Reason, BMJ 2000;320:768-770
The Swiss Cheese Model of System Accidents
กายวิภาคของความผิดพลาดทางการแพทย์ (Anatomy of Medical Errors)
Error
5
The Real Word
Healthy appearing decrepit 69 year old male, mentally alert but forgetful
The skin was moist and dry.
Occasional, constant, infrequent headaches.
Patient was alert and unresponsive
Rectal examination revealed a normal sized thyroid.
She stated that she had been constipated for most of her life, until she got a divorce.
Levels of Safety
Design, Management, “Blunt” Training, Policies,
RegulationsRules
Provider
“Sharp”
Accident Causation Model
ACCIDENT
Latent Errors
Systems Defects
Triggering Factors
UnsafeActs
Def
ense
s
Errors
Def
ense
s
Contributing Factors (Vincent)
z Work environmentz Team factorsz Individual (staff) factorsz Task factorsz Patient factorsz Organization and Managementz Institutional context
Accident Causation Model
ACCIDENT
Latent Errors
Care Managem’t
Problem
Def
ense
s
Def
ense
s
Contributory Factors
J.Reason, BMJ 2000;320:768-770
The Swiss Cheese Model of System Accidents
Modified from: James Reason (1993): Pix source: simula5on.londondeanery.ac.uk
Organizational Accidental Causation Model
Accident

Modified from: Reason (1993); Pix source: webmm.ahrq.gov
“Swiss Cheese Model”

Figure Source: medicexchange.com
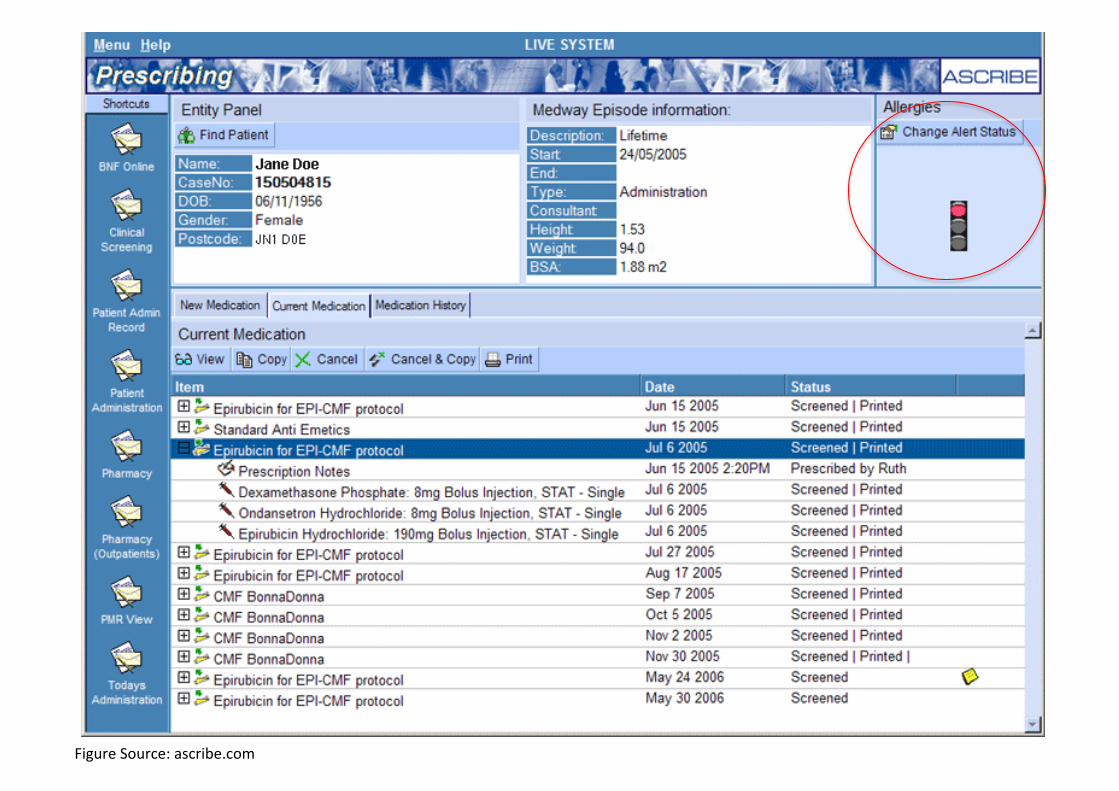
Figure Source: ascribe.com

Figure Source: nejm.org

Source: amazon.com, matichonbook.com
• By design, safe healthcare systems should prevent medical errors and avoid iatrogenic injuries.
Disclaimer: Yes, this is my self-advertisement!

Levels of Health System vs. Policy
Source: Gilson, editor (2012). Health Policy and Systems Research: A Methodology Reader.
= Patient care teams"
= Health Centers, Hospitals"
= National systems"

How to avoid those pitfalls?
Pix source: online.wsj.com

คาถากันตกหลุม #1: เข้าใจว่ามนุษย์ทุกคนมีโอกาสทำผิดพลาดได ้
หลุมพราง #1: มองว่าคนอื่นทำผิดพลาด แต่ฉันไม่มีวันพลาด! (I am careful, and I will never fail you!)
มองเห็นทั้งศักยภาพและขีดจำกัดของตนเอง และมองหาระบบที่จะช่วยลดความผิดพลาดของตนเอง
Pix source: bbs.playpark.com; siamhealth.net; utdclub.com

คาถากันตกหลุม #2: เข้าใจว่าแก่นของคุณภาพคือ“ระบบงาน”
หลุมพราง #2: มองเรื่องคุณภาพเป็นเพียง สมรรถภาพส่วนบุคคล (Is it individual competency?)
มองเห็นทั้งปลายแหลม (sharp end) และปลายทื่อ (blunt end) ของงานที่ยังมีความผิดพลาดหรืองานที่ยังไม่ได้คุณภาพ
Pix source: docblogs.wordpress.com; gearjunkie.com

คาถากันตกหลุม #3: “รู้จักแก่นและกระพ้ี เข้าใจความเหมือน
และความแตกต่างของแนวคิดและเครื่องมือการบริหารจัดการ”
Pix source: praphansarn.com; school.discoveryeducation.com/
หลุมพราง #3: มองระบบคุณภาพของรพ.ว่าไม่ใช่ธุระของแพทย์ (Is it a job of clinicians?)
ปรับเปลี่ยนแนวคิดจากการทำงานตามมาตรฐานวิชาชีพเท่านั้น ไปสู่การจัดการเพื่อพัฒนากระบวนการดูแลผู้ป่วยในโรงพยาบาล

Conclusion: What externs can do?
Pix source: online.wsj.com

Patient Safety in Hospital Settings
What externs can do?
① เรียนรู้ศักยภาพและขีดจำกัดของตนเอง ② เข้าใจระบบที่เกี่ยวข้องกับกระบวนการดูแลผู้ป่วย ③ ร่วมทำงานเป็นทีมดูแลผู้ป่วยและสร้างโอกาสเพื่อ
พัฒนากระบวนการดูแลผู้ป่วย
“พัฒนาตน สนใจระบบ”

Patient Safety at Ambulatory Settings
What externs can do at OPDs? ① Reconcile medications for each patient regularly
② Write understandable and legible prescriptions with indications, and also use an electronic prescribing system when available
③ Empower your patients, and yourself, to serve as “safety double checkers”
“RULE”

Basic Principles of Patient Safety Concepts/Theories Implications/Solutions
• Cognitive errors • Slips vs. Mistakes
• Latent Errors • Flaw designs of care delivery
systems
• Systems thinking • Swiss Cheese model • Complex Adaptive Systems
• Building in redundancies and cross checks • Standardization and
simplification • Forcing functions
• Culture of safety, learning from one’s mistakes • Well-trained, well-staffed,
well-rested workforce Source: Wachter (2012). Understanding Patient Safety

การพัฒนาคุณภาพรพ.ไม่ใช่งานเอกสารธุรการ แต่เป็นงานบริหารจัดการ
ความปลอดภัยของผู้ป่วยเกิดขึ้นได้โดยการพัฒนาคน (People) กระบวนการ (Process) และสมรรถภาพองค์กร (Performance)
Pix source: facebook.com/medicalhoumour
การพัฒนาความปลอดภัยของผู้ป่วยต้องใช้ทั้งสมองและหัวใจ

Pix source: facebook.com/pathtopeachandhappiness
การพัฒนาความปลอดภัยของผู้ป่วย • เปิดใจ การพัฒนาความปลอดภัยของผู้ป่วยไม่ใช่เรื่องยาก แต่ก็ไม่ใช่เรื่องง่ายจนทุกคนสามารถปฏิบัติได้ทันที
• ความรักองค์กร ความหวังดตี่อผู้ป่วย และความต้องการพัฒนาการทำงานของตนเองเป็นแรงจูงในที่สำคัญที่สุด
ของการทำงานพัฒนาคุณภาพ • นักพัฒนาต้องเรียนรูห้ลักคิด/ทฤษฎี สามารถเชื่อมโยงแนวคิดต่างๆ ได้
เข้าใจการใช้เครื่องมือต่างๆ แต่ ไม่ยึดติด และมีการฝึกปฏิบัติเสมอ













![Chapter 9 [1] Patient Safety. Introduction Patient safety comprises the reporting, analysis and prevention of adverse healthcare events and medical error](https://img.dokumen.tips/doc/110x75/56649ef45503460f94c07b5a/chapter-9-1-patient-safety-introduction-patient-safety-comprises-the-reporting.jpg)