Embed Size (px)
Citation preview
OBSTETRICS II FOR SECOND YEAR
GENERIC MIDWIFES
By Gebremaryam Temesgen October 2014

OVERVIEW OF MATERNAL MORTALITY
2
Definitions
Maternal Mortality = is defined as 'the death of a
woman while pregnant or within 42 days of
termination of pregnancy, irrespective of the
duration or site of pregnancy, from any cause
related to or aggravated by the pregnancy or its
management but not from accidental or incidental
causes.
Can be Direct or Indirect Maternal Deaths
Cont…
Direct maternal death. The death of the mother
resulting from obstetrical complications of pregnancy,
labor, or the puerperium, and from interventions,
omissions, incorrect treatment, or a chain of events
resulting from any of these factors.
An example is maternal death from exsanguination
after uterine rupture.

Cont…
Indirect maternal death. A maternal death not
directly due to an obstetrical cause, but resulting
from previously existing disease, or a disease that
developed during pregnancy, labor, or the
puerperium, but which was aggravated by maternal
physiological adaptation to pregnancy.
An example is maternal death from complications of
mitral valve stenosis.
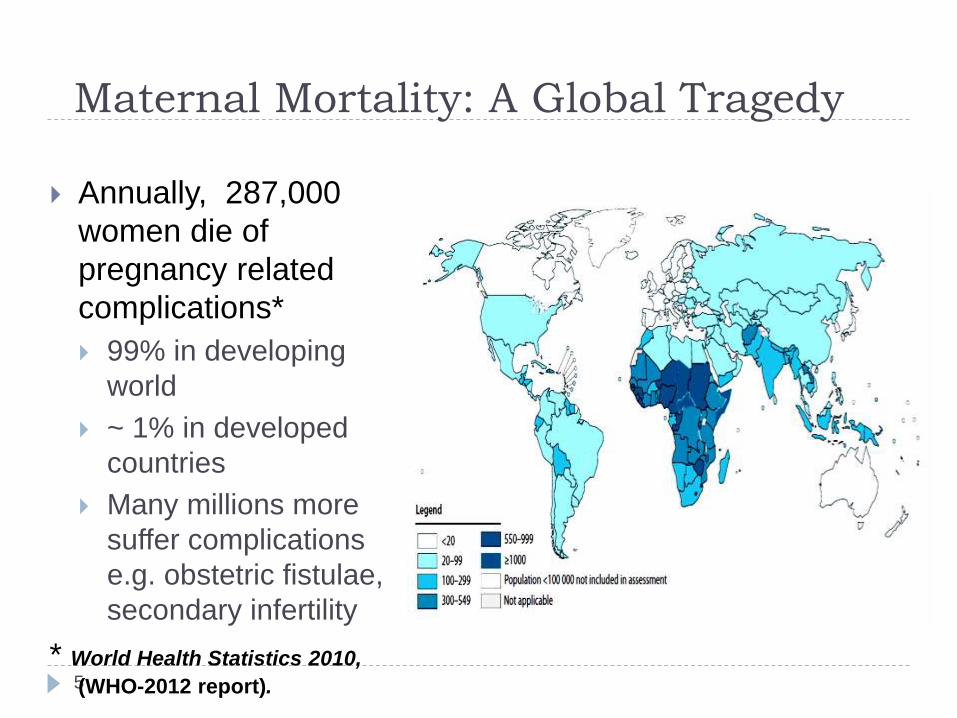
Maternal Mortality: A Global Tragedy
5
Annually, 287,000
women die of
pregnancy related
complications*
99% in developing
world
~ 1% in developed
countries
Many millions more
suffer complications
e.g. obstetric fistulae,
secondary infertility
* World Health Statistics 2010,
(WHO-2012 report).

Maternal Mortality trends
6
Globally, the total number of maternal deaths
decreased from 543 000 in 1990 to 287 000 in 2010.
Likewise, the global maternal mortality ratio (MMR)
declined from 400 maternal deaths per 100 000 live
births in 1990 to 210 in 2010
Maternal Death Watch
(Global)
7
380 women become pregnant
190 women face unplanned or
unwanted pregnancy
110 women experience a
pregnancy related complication
40 women have an unsafe
abortion
1 woman dies every two
minutes from a pregnancy-
related complication
Every Minute...
Of every day...

8
Ask group: What are the major
causes of maternal
mortality?

9
*Nearly all (99%) abortion deaths are due to unsafe abortion. **This category
includes deaths due to obstructed labor or anaemia.
Other direct causes include embolism, ectopic pregnancy, anesthesia-related. Indirect
causes include: malaria, heart disease. Source: WHO 2010.
Causes of maternal deaths, global

Maternal Mortality in Ethiopia
10
Out of estimated 2,924,225 pregnancies in
2003E.C, only 16.6% attended by a skilled health
provider. (Health and Health Related Indicators EFY,2003)
Maternal mortality ratio increased from 664/100
000 live births in 2005 to 676/100 000 live births
in 2011 (DHS-2011),
Our country is one of the six countries in 2008 which
contribute more than 50% of all maternal deaths. (THE
LANCET on 12 April 2010)

Maternal Mortality in Ethiopia; contd…
11
0
5
10
15
20
25
30
35
40
45
50
Delivery at healthfacility
ANC TT2+ PW/PAB
5
27
17
5
28 28
10
34
48EDHS 2000
EDHS2005
EDHS 2011

Maternal Mortality in Ethiopia; contd…
12
Causes of maternal mortality in Ethiopia; (Facility based study)

Neonatal Health: Scope of Problem
13
Newborn health and survival are closely linked to
care the mother receives before and during
pregnancy, childbirth, and the postnatal period.
Every year:
4 million neonatal deaths (first month of life)
4 million stillbirths
Eight neonatal deaths every minute
Two-thirds Rule
Global Infant Mortality Rates
14
More than 7 million infants die annually between birth and 12 months of age
Of those who die in the first year
Nearly 2/3 die in the first month
Of those who die in the first month
2/3 die in the first week
Of those who die in the first week
2/3 die in the first 24 hours

Ask group: What are major causes of
neonatal mortality?
15

Causes of Newborn Death
16
Ethiopia’s Neonatal Health status
17
Neonatal mortality is 37 per1,000 live births (DHS
2011).
50 percent of infant deaths in Ethiopia occur during
the first month of life.
One in every 17 Ethiopian children dies before
reaching age one,

Child Mortality Rate trends in Ethiopia:
NMR, IMR and U5MR
18
0
20
40
60
80
100
120
140
160
180
NeonatalMortality rate
InfantMortality rate
underfivemoratlity rate
49
97
166
39
77
123
37
59
88
EDHS2000
EDHS2005
EDHS2011

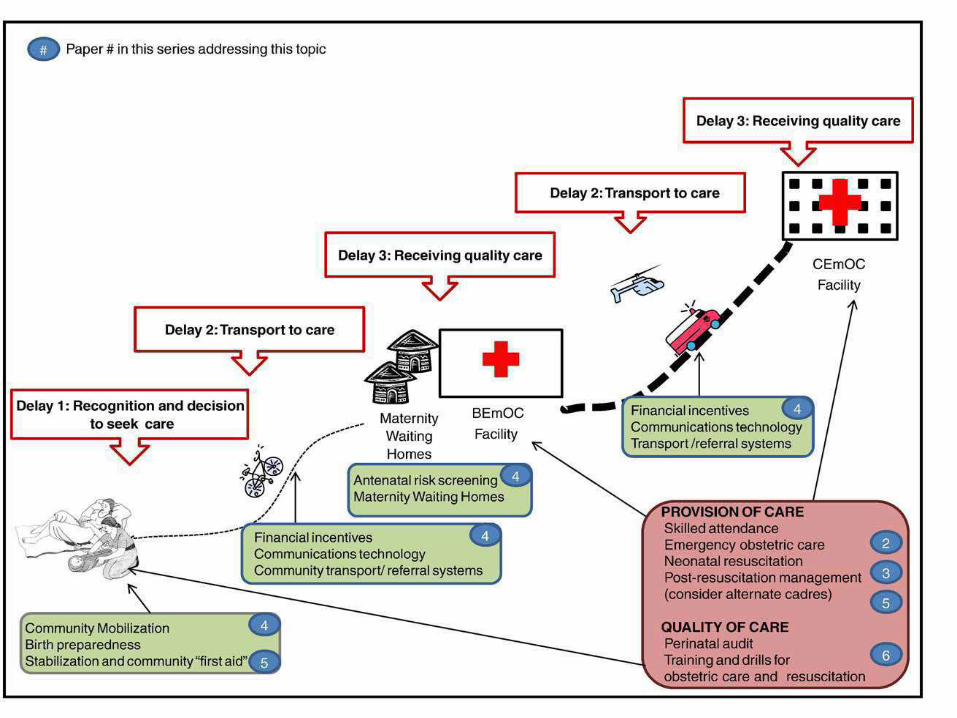
But WHY Do These Women and Newborns
Die?
19
Delay in decision to seek care Lack of understanding of complications
Acceptance of maternal and newborn death
Low status of women
Socio-cultural barriers to seeking care
Delay in reaching care Mountains, islands, rivers — poor organization
Lack of transport
Delay in receiving care Lack of triage system
Lack of supplies, personnel
Poorly trained personnel; poor attitudes
Three Delays Model

Ask group: What are some interventions that have
not proved successful in reducing mortality?
21

Interventions to Reduce
Maternal and Newborn Mortality
22
Historical Review
Traditional birth attendants
Antenatal care
Risk screening
Current Approach
Skilled attendant at delivery

Historical Review of Interventions
23
The flawed assumption:
Most life-threatening obstetric
and newborn complications
can be predicted or prevented

The Crucial Facts
24
Major obstetric complications are not predictable EVERY woman and newborn faces risk
Maternal deaths are not predictable
Most maternal deaths occur during labour, delivery
or the first 24 hours postpartum
When problems are managed in a timely and
effective manner, mothers and babies lives are
saved Providers and the facility must be prepared to address
emergencies at all times
80% of maternal deaths are preventable by appropriate
treatment
Interventions: Antenatal Care
25
Antenatal care clinics started in US, Australia, Scotland between 1910–1915
New concept - screening healthy women for signs of disease
By 1930’s large number (1200) ANC clinics opened in UK
No reduction in maternal mortality
Is ANC important? YES!! Focused, individualized care leads to early detection of
problems and birth preparation

Interventions: Risk Screening
26
Disadvantages
Very-poorly predictive
Costly: Removes woman to maternity waiting
homes
If risk-negative, gives false security
Conclusion: Cannot identify those at risk of
maternal mortality
Every pregnancy is at risk

What are the key interventions to reduce
maternal and neonatal mortality?
27
Access to family planning,
Skilled attendants during pregnancy and childbirth
Access to emergency obstetric and newborn care
(EmONC),
Effective referral system
Fully functioning health services 24/7

Most important intervention:
Skilled Attendant at Childbirth
28
A skilled health provider is:
an accredited health professional – midwife, doctor
or nurse – who has been educated and trained to
proficiency in the skills needed to manage normal
(uncomplicated) pregnancies, childbirth and the
immediate postpartum period and in the
identification, management and referral of
complications in women and newborns
(WHO, ICM & FIGO 2004)
WHO 1999.
Interventions:
Skilled Attendant at Childbirth
29
Interventions proven effective resulting in
decreased maternal mortality rates (MMR):
Malaysia: basic maternity services; MMR decreased
from 320 to 157
Cuba: national priority; MMR decreased from 118 to 31
China: facility based childbirth; MMR decreased from
1500 to 50