Embed Size (px)
Citation preview
Inferior wall MI and its complications
CLINICIAN IN CHARGE:
PROF. HILAL AH RATHER
Prof. Dept. of Cardiology
MODERATOR :
PROF. A R LONE
Dept of Medical oncology

45 yrs old male
Chronic smoker
Diabetic
HTN
presents with:
Retrosternal chest pain X 4 hrs
It was sudden onset,
Localised to left side of chest,
Stabbing in nature,
Feeling of heaviness on chest,
Radiation to left arm,( since 12 midnight)
On further enquiry, he gives History of:
Multiple episodes of vomiting,
Diaphoresis
Transient loss of consciousness(1-2 min)

Cough
Breathlessness
Sputum production
fever
Palpitations
Pain radiating to back
Headache
Weakness of any part of body.
Negative history

GPE:- Conscious, cooperative, oriented
VITALS:-
PULSE : 34 bts/min, regular,
BLOOD PRESSURE: 80/60mmHg
RR: 28 cycles/min
Spao2: 88%
Temp: Afebrile
JVP: Raised
Chest: NVBS, b/l symmetrical
CVS:- Normal precordium.
No murmur /s1s2+
P/A:- soft/ Non distended.
CNS:- GCS 15/15
Neck free, No meningeal Signs,
Cranial Nerves Normal
No neurological Deficit

HB TLC DLC PLT MCV ESR
14.2 21.54 87/6.
4
122 85/29 14
12.3 13.5 79/16 76 87/29 10
12.8 11.2 82/15 86 84/28
11.6 6.7 72/18 74
UREA CREATININE
58 1.12
65 .92
64 .86
69 .85
58 .90
Na K Ph PCo2 HCO3
136 2.5 7.46 33 23.5
149 4.1 7.35 41 16.7
135 3.1 7.44 44 22.6
138 3.8 7.43 42 22.5
141 4.4 7.26 12

ROUTINE URINE EXAM:
PC 3-4
RBC’S – NIL
SUGAR, ALB - NIL
CXR : wnl.



IWMI with Complete heart block with shock
with suspected RVMI.


IWMI with Complete heart block with shock
with RVMI with ? Proximal RCA Involvement.

O2 inhalation
IV Fluids
Inj stk 1.5 million units i/v in 100 ml of ns over 1hr.
Tab ecosprin 300mg stat f/b 150 od
Tab clopidogrel 300 mg stat f/b 150 mg od
Tab atorvastatin 80mg stat f/b 40 od
INJ Clexane 0.6ml S/C BD
Inj dopamine 5 ug/kg/min(4 days)
Inj dobutamine 5-10 ug/kg/min(6days)
Inj NA 7.5 to 10 ug/kg/min(5days)

Normal lV function
EF-68%
RWMA in inferior and inferoseptal segments
Mild PAH/TR.

In view of deteriorating hemodynamic status,
patient planned for pharmaco invasive PCI.

Mean pulmonary artery pressure: 18mmHg
LM: normal
LAD: mid lad-D1 long bifurcation lesion 80-90%
S2 septal lesion (ostial 80% lesion).
LCA: distal lcx 60-70% dis, proximal lCAplaquing.
RCA: Dominant, proximal plaquing, tight lesion in mid RCA (90% stenosis). Distal plaquing.
PCI to RCA(culprit vessel) done in the same setting with Nobori 3×18 stent

During pharmacoinvasive PCI he developed
multiple episodes of atrial tachycardia
managed with 200J synchronized DC shock.
Multiple episodes of hypotension responded
to inotropic support
TP lead placed in IVC prophylactically in
v/o of unstable rhythm and recurrent
bradycardia.

Post procedure when patient received inward he developed multiple episodes of venttachycardia.
Pt received multiple DC shock f/bAmiodarone infusion.(150mg I/V f/b 1mg/kgx6hr f/b .5mg/kgx 18hrs.)
In the same setting later patient developedmultiple episodes of SVT,AF,VT,AIVR(3-5episodes) and managed with multiple DCshocks..


Ph 7.26
Hco312.2
Pco2 26
Na 141
K 4.4
Urine for
ketones
++
Bsugar
468mg/dl
Again complicated by DKA with sev
acidosis in the evening..
Patient managed with insulin
infusion and i/v fluids DNS with
10meq k+ /500ml DNS @ 75ml/hr..

Patient developed severe junctional bradycardiaand hypotension.
Amiodarone infusion stopped.
I/v atropine given, but pt persisted with severebradycardia and hypotension.
TP lead advanced into RA and TPM switched on,Position confirmed on monitor.HR set on100/min.
Patient hemodynamically improved.

Patient developed again one episode of SVT
in the evening and managed with Inj
diltiazem 10mg I/v stat.
Patient again developed 3 episodes of
sustained VT in the evening at 10 pm..
Managed with DC shock and overdrive pacing
again started on amiodarone infusion..



Dopamine tapered off and stopped and
started on Dobutamine 2.5ug/kg/min and NA
continued and up titrated to from 10 to 15
ug/min
Patient remains hemodynamically stable on
dual inotropic support.
No fresh episode of any arrhythmia
documented..

Symptomatically better
Patient remained haemodynamically stable
on dual inotropic support being gradually
tapered off..
No further episode of any arrhythmia
documented
TP lead removed on day 6th..

Patient gradually tapered off support…
Since day 9th patient was ambulatory.

Young male, chronic smoker ,diabetic,hypertension. Admitted as a case of IWMIwith RVMI.
Managed pharmacoinvasively, stented inRCA..complicated post operatively bymultiple episodes of Tachyarrythmias, Af, VT,AIVR managed with multiple DC shocks ,RVand Atrial pacing.
Discharged in a stable condition and plannedfor PCI to LAD-DI later On..
DISCHARGE


Right ventricle myocardial infarctions (RVMIs)accompany inferior wall ischemia(usuallyinvolves inferior wall of left ventricle) in up toone-half of cases.
The clinical sequelae of RVMIs vary from nohemodynamic compromise to severe hypotensionand cardiogenic shock.
Diagnosis is based on physical examination,ECG,ECHO and CAG.right-sided precordial leadsparticularly lead V4R must always be included.(ACC guidelines)

RVMI leads to reduced LV filling which translates intopoor LV pre load in addition ischemia to theconduction pathways disrupts normal rate andrhythm.
Adequate fluid administration in combination withpositive inotropic agents and early coronaryreperfusion are crucial components of treatment.
Diuretics and nitrates should be avoided.
Intra-aortic balloon counter pulsation and rightventricle assist devices may be used with success inRVMIs associated with medically refractory heartfailure.

The occurrence of RV impairment depends primarilyon the location of the MI, which ranges from rarecases in the anterior heart wall to more commonlocations such as in the inferior wall in 24% to 50% ofcases.
The relatively small percentage of RVMIs may beexplained by several factors:
1. Lower oxygen requirements of the RV due to itssmaller muscle mass and workload.
2. Increased blood flow during diastole and systole;
3. More extensive collateralization of the RV, primarilyfrom the left coronary system; and
4. Diffusion of oxygen from intrachamber bloodthrough the thin wall of the RV and into theThebesian veins .

Physical examination
1. The typical triad observed on physical
examination is hypotension occurring with
jugular vein distention and clear lungs.
2. A tricuspid regurgitation murmur,
Kussmaul’s sign and pulsus paradoxus are
signs of significant hemodynamic effects
due to RV ischemia.

ST segment elevations in leads II, III and aVF.
Disproportionate ST segment elevation with
greater ST elevation in lead III than in lead II
is pathognomonic for an RVMI.
ST segment elevation across the entire right
precordium from V1R through V6R; a sole ST
segment elevation in lead V4R >1.0 mm is a
reliable marker of an RV infarction, with
100% sensitivity, 87% specificity.

RV dilation with depressed systolic function
RV free wall dyskinesia with paradoxical
septal motion.
Asses the LV function secondary to RWMI—in
case of refractory to IV fluids—to rule out
cardiogenic shock.
Angiography often reveals occlusion of the
right coronary artery (RCA) proximal to the
acute marginal branch, while more proximal
occlusions usually suggest more extensive
necrosis of the posterior and, potentially, the
anterior RV myocardial wall.
In patients with left coronary artery
dominance, a left circumflex coronary artery
(LCX) occlusion may also be found

1. Post infarction ischaemia.
2. RVMI
3. VPCs/VT/VF
4. AF
5. AFL
6. AIVR
7. Sinus bradycardia
8. Pericarditis
9. Septum rupture
10. Cardiogenic shock

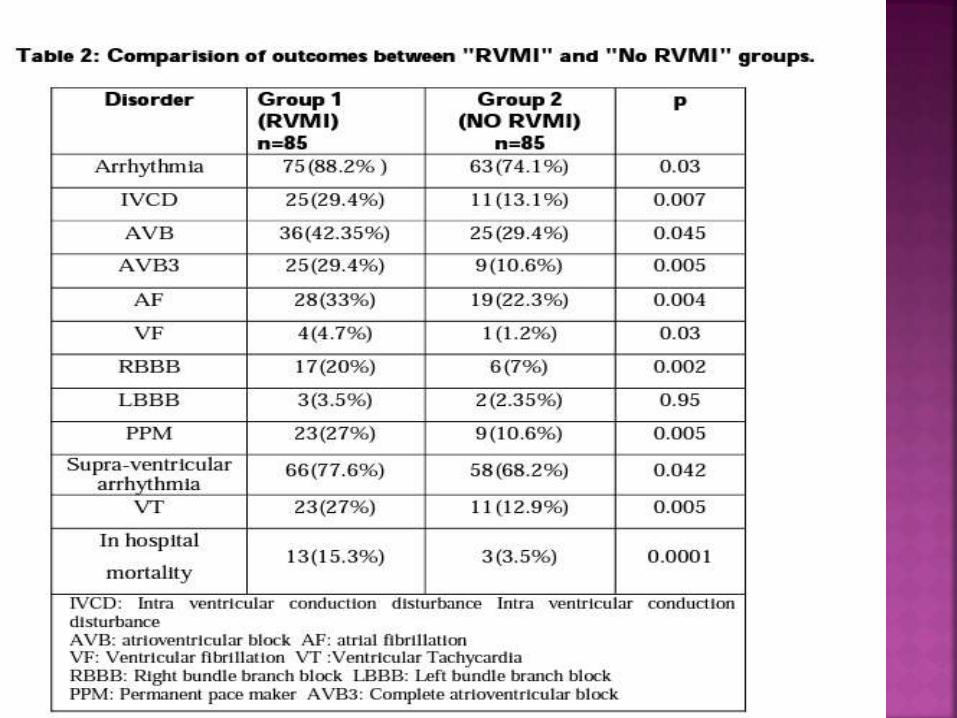
RVMIs are more often complicated by all
types of arrhythmias compared with ‘simple’
inferior or anterior wall LVMIs.
Barrillon et al were the first to recognize the
significantly higher risk of severe conduction
disorders in patients with RV involvement.
Complete atrioventricular (AV) or sinoatrial
blocks occurred in onehalf of cases in which
ST segment elevation or a QS pattern in V3R
and/or V4R were present.

Initial therapy, requires the administration of sufficient
volume to increase RV filling; it is critically important to
avoid drugs that cause venodilation and a decrease in RV
filling (eg, nitrates, diuretics). Treatment is generally
recommended to begin with a volume challenge of 300 mL to
600 mL normal saline over 10 min to 15 min.
Invasive hemodynamic monitoring is recommended, because
further infusion may be harmful in some patients, who don’t
respond to fluid challenge if additional increases in RV
volume prevent sufficient LV filling via interventricular
interactions and intrapericardial pressure equalization.
Based on hemodynamic monitoring studies, exceeding a RAP
or PCWP of 20 mmHg is generally not recommended .

If initial volume loading fails to improve arterial
pressure and cardiac output despite significant
increases in RAP and PCWP, then positive
inotropic agent therapy, can be effective in
stabilizing patients.
Restoration of sufficient coronary blood flow
represents the only treatment that addresses the
underlying problem, and early reperfusion
improves RV performance as well as the clinical
course and survival.

1. IWMI in 30-50% cases associated with RVMI.
2. Triad of raised jvp ,hypotension ,and clear
lungs think of RVMI.
3. Take Rt sided V4R in all patients with IWMI.
4. Presence of RVMI increases mortality of
patients.
5. IV fluids and ionotropes ,A-V sequential
pacing play a equally contributing role in
the managements of patients on
presentation.

Thank You
Dr. piyush khajuriaPG Student





























