Embed Size (px)
Citation preview

IMAGE GUIDED-ADAPTIVE RADIOTHERAPY
….Have We Really Understood ?
Where do we stand now?
Presented by: Dr. Vijay Kumar KModerator: Dr. Tanweer

LINE OF PRESENTATION
• What exactly is Adaptive Radiotherapy
• Rationale
• Concept Of ART
• Types or Components
• Site Specific

NATURE ADAPTS
• From Latin “adaptare” means “to fit”

IGRT…! what exactly it is ?
• “External beam radiation therapy with positional verification using imaging prior to each
treatment fraction”
• “Any use of imaging to aid in decisions in the radiotherapy process”
• “A procedure that refines the delivery of therapeutic radiation by applying image-based
target re-localization to allow proper patient repositioning for the purpose of ensuring
accurate treatment and minimizing the volume of normal tissue exposed to ionizing
radiation” – ASTRO
• “The use of imaging for detection and diagnosis, delineation of target and organs at risk
(OAR), determining biological attributes, dose distribution design, dose delivery
assurance, and deciphering treatment response,” a so-called six-dimensional definition

• Although both IGRT and Adaptive Radiotherapy exists from long back,
With time… with improving technology…
• Radiation techniques improved and so, THE OUTCOMES.
• Adaptive Radiotherapy never an individual entity without IGRT..!!

EVOLUTION OVER DECADES

• A radiation treatment process where the treatment plan can be modified using a
systematic feedback of measurements is named ‘Adaptive radiation therapy’ (ART).
• The importance of using an adaptive process in radiation therapy is that the
treatment plan, especially the margin and treatment dose, can eventually be
customized to the individual patient.
• Adaptive radiation therapy has been introduced to incorporate the position
variation of the individual patient into the treatment optimization process during the
course of radiotherapy.

• The concept of ART can also be applied to compensate for other treatment
variations such as radiation sensitivity and density of clonogenic cells when
they become measurable during the treatment course.

15/07/2016

DEFINITION OF ART
• Adaptive radiotherapy can be defined as,
Temporally changing the treatment plan delivered to a patient based on
observed anatomic changes caused by tumor shrinkage, weight loss, or
internal motion – Leibel Philips.
“The ability to measure changes in location, morphology and
physiology (like breathing, tumor response, weight loss) and adapt the
course of treatment will lead to adaptive treatment, also called 4D
adaptive treatment” – ICRU 83

FACTORS CAUSING ANATOMIC CHANGES TO TUMOR AND NORMAL TISSUES
• Anatomic motion (PHYSIOLOGICAL) caused by the musculoskeletal,
respiratory, cardiac, gastrointestinal, and genitourinary systems.
• Treatment-induced changes such as cell death and tumor shrinkage, tumor
growth resulting from accelerated repopulation, weight loss or gain because
of changes in appetite caused by radiation, concomitant chemotherapy or
hormone therapy, fibrosis of normal tissue, and so on

RATIONALE
• Changing anatomy of both tumor and normal tissue—
It naturally follows that the delivery of radiotherapy should be temporally
changing to match the observed anatomic changes
In other terms,
If the PTV and normal anatomy are changing with time, we are obligated to
adapt our treatment delivery where possible.

DIFFERENT WAYS TO ADAPT
TYPES OF ART Examples
Motion adaptive Beaumont’s ART process, ‘Plan of the
day’ IMRT
Biological adaptive Theragnostic planning
Response adaptive Mid-treatment response evaluation,
shrinkage of GTV & OAR
Time adaptive Mid-course CT and planning

PROCESS INVOLVED IN ART

COMPONENTS
• Adapt to tumor motion
• Adapt to tumor / organ deformation and volume change

ADAPTING TO TUMOR MOTION
• Move couch electronically to adapt to the moving tumor
• Exac trac 6D Robotic couch
• Move a charged particle beam electromagnetically
• RPM system
• Move a robotic lightweight linear accelerator
• Cyber knife
• Move aperture shaped by a dynamic MLC
• Calypso system

CONCEPT OF ART
• Adaptive radiotherapy can occur at three different timescales:
Offline - between treatments,
Online - immediately prior to a treatment, and in
Real time - during a treatment


IMAGE REGISTRATION
• Registration : means to align two imaging data sets in a common coordinate space
by transforming one image set while keeping the other one fixed.
• Voxel to voxel matching b/n 2 image sets.
• Fixed image to floating image
• A transformation matrix created
• It is an optimization process- success achieved after iterative comparisons.


IMAGE REGISTRATION
• According to the nature of transformation-
• It is of 2 types- Rigid registration and Deformable registration.
• Rigid fusion-
• Direct intensity match or point match
• No compensation for motion or patient position
• 6 degrees of freedom

• Deformable image registration –
• Complicated
• Consists of a matrix with huge number of unknowns.
• Multimodality images can be fused
• Allows dose and contour information to be transferred between images, substantially
reducing workload.
• As the timescales for adaptation decrease, the computation time of deformable image
registration must correspondingly decrease.


APPLICATIONS
(1) Better Target Definition
(2) Image Enhancement
(3) Propagation Of Organ Contours From One Image Set To Another
(4) Calculation Of Accumulated Dose In Organs Experiencing Inter- Or Intra-
fraction Organ Deformation For 4-D Or Adaptive Therapy Planning
(5) 4-D Image Reconstruction

ISSUES:
• Definition of registration metric function
• Algorithm
Registration can be broadly divided into
• Manual, landmark-based, surface-based, intensity-based, and mutual information–based registrations.
Depending on the mechanism or method used to model the deformation, registration can usually be
categorized into
• Elastic model, viscous fluid model, optical flow model, finite element model, radial-basis function model
such as basis spline model, and thin-plate spline model.

• Basis spline model- most commonly used
• Selection algorithm- depend on metric function
• Most of algorithms depend on intensity matching but ignore tissue features –
can be countered by physiologic and anatomic knowledge
• Eg- Bone wrapping
• Cost function- Similarity measure
• Penalty function- discourages undesirable transformations.

Deformable Transformation
Fixed ImageMoving ImageFixed Image
Courtesy Dr Prahlad

Deformable Transformation
Courtesy Dr Prahlad

Deformable Transformationy
x
Courtesy Dr Prahlad

FIXED IMAGE
Courtesy Dr Prahlad

MOVING IMAGE
Courtesy Dr Prahlad

REGISTERED IMAGE
Courtesy Dr Prahlad

REGISTERED IMAGE
Courtesy Dr Prahlad

REGISTRATION BEYOND DEFORMATION MODEL
• pCT vs pCT- easy but pCT vs CBCT-- ?
• d/t poor quality or gross anatomic changes
Eg- 1. variation in rectal contents, bowel gas, feacal matter- direct intensity matching
cannot be done.
2. motion of lung, liver
3. weight loss or gain ( algorithms reliable only for a volume change of 3% -
time span b/n consequent imaging to be reasonable)

TRANSFER OF CONTOURS
• Accuracy of registration matters- influenced by image content distant from
ROI.
• Surface mapping techniques: efficient for pCT to CBCT contour transfer
• ROI contour extended surface
• Hybrid – deformable and surface model best method
• Narrow shell around ROI extended 1-2cm on pCT merged with CBCT

CBCT
• Large variation of HU for same material under different scanning conditions.
• In the absence of organ motion– Accuracy is acceptable for dose verification but not
for treatment planning.
• With organ motion– 5-8% discrepancy can be seen.
• Electron density matching– may be a solution.
• Where it stand in ART ?

OFFLINE ADAPTATION
• The imaging system used : Conventional CT scanner or an in-room CT
scanner.
• The adaptation can be triggered by :
• As a protocol (for example after 20 and 40Gy delivered dose),
• Clinical observations of masks not fitting, weight loss, or other surface changes,
or by changes observed on an in-room imaging system

• The rationale - substantial shrinkage of the tumor/weight loss throughout the
course of therapy, between the anatomy at the time of the original CT scan
and the cone beam CT scans acquired during treatment.
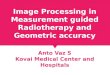
Planning CT After 16# After 25#



ONLINE ART
• Online Adaptation is typically referred to Imaging Just prior to each
treatment and the plans were adapted to changing anatomy daily.

ONLINE ART
• This can be done either by correcting the errors or by modifying the
contours.
• Daily re-planning ??

• Although it may be trivial to occasionally re-plan a limited number of
patients offline, frequent re-plannings of many patients are labour and time
intensive, especially if online re-planning is necessary.

GRAPHICS PROCESSING UNIT (GPU)
• Researchers at the University of California–San Diego have explored the
potential to perform online re-planning utilizing the vast computational
capability of the graphics card technology.
• It is possible to dramatically improve the computational efficiency of the
traditionally computationally intense tasks in RT such as dose calculations,
inverse planning re-optimizations, CT reconstructions,and deformable image
registrations for fast contour mapping.

• Gu et al. have shown that a full 3D-dose calculation based on finite-size pencil
beam algorithm achieved a speed up of 200 to 400 times, taking less than 1 second
for typical IMRT plans.
• Men et al. found that, for a typical nine-field prostate IMRT plan with 5-by-5 mm2
beam-let size and 2.5-by-2.5-by-2.5 mm3 voxel size, re-optimization would only take
2.8 seconds.
• Park et al. found that for a filtered back-projection reconstruction of a typical 3D
CBCT, volume can be done in a real-time fashion (i.e., as soon as the scan is done)

CLOUD COMPUTING
• Pioneered by Meng et al. And Wang et al. at stanford university.
• It’s a form of SUPERCOMPUTING technology.
• The task is divided up and handled in a parallel computing manner,
automatically.
• This system does not require the computers to be physically located near the
user, and they can be accessed from anywhere with an internet
connection,
• The larger the number of nodes used, the faster the computations.

WORK-FLOW

LIMITATIONS
• The technology is new and research in RT is in its infancy; but the potential
benefits remain to be seen.
• How often should new plans be generated? Once? Weekly? Daily?
• Whether altering the target volume would adversely impact tumor control ?

REAL-TIME IMAGE-GUIDED ADAPTIVE RADIOTHERAPY
• Imaging session and treatment session are intertwined
• Time separation is shown to be on the order of seconds or less.
• Rationale - significant drift in the mean position of a tumor during
radiotherapy treatment.
• The concept of intra-fraction motion management arises…here !

MOTION MANAGEMENT
• Respiration induced
• Organ motion

METHODS TO CONTROL / COMPENSATE FOR LUNG MOTION
DURING RESPIRATION
• Free breathing methods:
Internal Target Volume (ITV)-based treatment
Gating
Tracking
• Breath-hold methods:
Active Breathing Coordinator (ABC) - DIBH

GATING
• Treatment delivery is done in the phase of respiration where the tumor
motion & resulting treatment volume is minimum, by coupling the beam
delivery with the phase of respiration
• It can be invasive or non-invasive.

REAL TIME TUMOR TRACKING
• Imaging is used to track the actual tumour motion during treatment delivery
and to move the treatment beam accordingly based on the varying
position of the tumour.
• Usually requires an internal fiducial, implanted within the tumour.
• Can also be done non-invasively in some cases.

SIMULATION
• Patients for gating/ tracking/ITV-
based treatment undergo plain
4DCT scan for planning (3mm
slices), using Mayo belt/ Anzai belt/
RPM system to correlate the
respiratory phases and
corresponding CT images.
• Ten data sets are thereby
generated.

VOLUME DELINEATION
• Tumor delineation is done on the end-expiratory data set. This is because, in this
phase, lung motion is minimum.
• No CTV margin is given for stereotactic body radiotherapy for early inoperable lung
cancers.
• For locally advanced disease, CTV margins between 0.6-0.8 cm are usually applied.
• Setup margins of 0.5 cm are normally applied (to the GTV/ CTV/ITV, as appropriate)
to arrive at the PTV

Gating can be internal or external
• Internal – Uses tumor motion surrogates such as implanted fiducial markers or
marker-less imaging of internal anatomy.
• Eg: RTRT system
• External – uses external respiratory surrogates such as markers placed on the
surface of the patient’s abdomen, a compression belt, or spirometer signals.
• Eg: RPM system, Exac trac

RPM SYSTEM (VARIAN)
• Lightweight plastic block with two or six passive infrared
reflective markers
• Monitored by video camera mounted on the treatment
room wall.
• The surrogate signal is the abdominal surface motion.
• Both amplitude and phase gating are allowed.
• disables the beam when the waveform becomes
irregular, such as with patient motion or coughing, and re
enables the beam after establishing breathing is again
regular.

EXAC-TRAC GATING/NOVALIS GATING
• This device uses external markers for gating.
• it uses x-ray imaging to determine the internal anatomy position and to verify
its reproducibility during treatment.
• By updating the correlation between the internal and external signals in a
reasonable frequency, x-ray exposure to the patient is minimized, while the
external gating signal accuracy is maintained.

• Oblique image pairs are taken by Exac-Trac system’s stereoscopic X ray
imagers.
• The system builds a correlation model between the end-positions and the
respiratory phase (accuracy of correlation 3mm).
• The treatment beam is then turned on and is configured to treat ONLY in
the gating window

R T -TRACKING
• Most ideal—and most technologically intense—strategy,
• Real-time tumor localization, fast processing and relay of information, and corresponding
repositioning of the beam all need to be dynamically seamlessly integrated.
Available Systems:
• ExacTrac system (VERO)
• Cyberknife
• Calypso System

PRINCIPLE OF TRACKING

REQUISITES OF CORRELATION MODEL
• Accuracy
• Speed
• Imaging dose required should be minimum

CYBER KNIFE: RTT MODES
Non-invasive:
Xsight lung
• Possible if:
• Tumour >1.5 cm, surrounded by air
• Tumour visible by imaging system
Invasive (with implanted fiducial):
Synchrony
• 3-5 fiducial markers need to be
inserted in close proximity to the lesion.
• They have to be well- separated
(>2cm) and non overlapping on
projections from the in room x-ray
images


VERO (BRAIN LAB-MITSUBISHI)

• Has 6MV C-band LA mounted on O-
ring gantry
• Gantry is mounted on gimbals
• Capable of Pan & Tilt motions
• Maximum motion allowed=2.5 cm in
isocentre plane or 2.5 degrees in
each direction
• Also has 2 kV X ray imagers,
mounted at 45 degree angle with the
MV beam axis
• Has facility for Cone Beam CT & Real
Time Tumor Tracking (based on Infrared
& stereoscopic X rays) .
• 6 degrees of freedom
• Patient repositioning not required as the
system can move itself
• Image verification possible at any
position during treatment.

ELECTROMAGNETIC TRACKING SYSTEMS (CALYPSO)
• Make use of electromagnetic transponders
(beacons)
• Embedded within the tumor
• Motion of these beacons may be tracked in real time
using a detector array system.
• Beacons need to be placed through a minimally
invasive procedure, their presence may introduce
artifacts in mr images, and there are limitations to the
patient size.
• Calypso has a geometric accuracy of <2 mm, but its
use at present is limited to prostate radiotherapy.

BIOLOGY GUIDED ART

RATIONALE FOR NON UNIFORM DOSE ESCALATION
• Local recurrences arise from micro environmental niches that are relatively resistant at
the radiation dose level that can safely be delivered using a uniform dose distribution
• molecular and functional imaging will allow spatiotemporal mapping of these regions of
relative radio-resistance
• advances in radiation therapy planning and delivery technologies facilitate the delivery
of a graded boost to such regions, which, in turn, should lead to improved local tumor
control with acceptable side effects

CHASING THE FAILURE PATTERNS

COMPARISON OF VARIOUS IMAGING MODALITIES

• Biology-based objective functions can be introduced to the radiation treatment planning
process by co-registration
• Dose painting
-Subvolume boosting-imaging defined discrete volume is given an additional boost
- Dose painting by numbers- in which a dose is prescribed at the voxel level and it is left for the
dose plan optimizer to arrive at a physically deliverable dose distribution

DOSE PAINTING BY NUMBERS
Gregoire et al., Lancet Oncol 2012

DOSE ESCALATION VS TOLERANCE

SITE SPECIFIC ADAPTIVE RADIOTHERAPY

HEAD AND NECK
• We usually adapt to changes in morphology of tumor and OAR’s.
• Provoking factors: weight loss, tumor response, progression of disease
Hansen et al.
• evaluated the impact of replanning in a cohort of 13 HNC patients with either significant
weight loss or tumor response during IMRT.
• Compared to replanning, not replanning significantly decreased dose to the target
volume and increased doses to normal tissues (spinal cord and brainstem). The doses to
95% of the PTV-GTV and the PTV-CTV decreased by up to 6.3 Gy and 7.4 Gy,
respectively.


Adaptive radiotherapy of head and neck cancer
Pierre Castadot, MD, John A. Lee, Eng, Phd, Xavier Geets, MD, Phd, AndVincent Grégoire, MD, Phd, FRCR
• Positioning errors and their causes and strategies that could be adopted to
counteract setup uncertainties.
• Anatomical modifications

Anatomical ModificationsOf Target Volumes And Organs
At Risk During Radiation Therapy
• These include the shrinkage of the primary tumor and nodal volumes,
resolving postoperative changes or edema, and weight loss.



Dosimetric ImpactOf Anatomical Modifications
• Alteration in patient anatomy during treatment modifications of both
target volumes and OARs, the dose distribution that is actually delivered
to the patient might significantly differ from what was planned.


• 51 papers were reviewed.
• Adaptive radiotherapy (ART) could be applied to reduce dose to OARs and
eventually to improve quality of life.
• It is unlikely that every patient will benefit from ART.
• Selection of patients is most important.
• There are no guidelines to when and what time schedules adaptation should be
done.

• Anatomic and dosimetric changes are more pronounced in Parotid gland.
• The average volume decrease of the PG’s during radiotherapy was 26 ± 11%.
(Mostly during first half of treatment).
• The most common reported anatomic changes were volume loss and medial shifts
of the PG’s.
• On average, the PG mean dose increased with 2.2 ± 2.6 Gy as compared to the
dose calculated on the planning CT at baseline. (Site specific- may go up to 10Gy)

• It was directly associated with higher grade 2 or more xerostomia in those
patients.
• Weight loss >5% and/or decrease of neck diameter >10% was associated
with higher xerostomia.
• Chen et al. - In less than 20% of all head and neck patients replanning was
needed because of target underdosage or OAR overdosage, usually during
the first three weeks of treatment

• 36 patients
• 54-Gy dose to both high-risk and low-risk target volumes in Phase I.
• Phase II (adaptive) plans for 16 Gy to high-risk planning target volume.
RESULTS:
• Median reductions in gross primary and nodal disease volumes on mid-treatment scans were 34% and 43.2%,
respectively. Four patients developed local recurrences, all within the RT field. Median DFS and OS were 17.5 and
23.5 months, respectively.
ADVANCES IN KNOWLEDGE:
• This study supports the need for adaptive replanning for minimizing normal tissue toxicity without compromising
local control and adds to the existing body of literature.

ART IN PROSTATE CANCER
• Major concern is to reduce the treatment margins to reduce normal tissue toxicity
• To incorporate generic set up errors and application of predetermined set up margins.
• Individualized setup adjustments to reduce the magnitude of setup error
IGRT forms the basis for adaptation

DISTENDED RECTUM ON PLANNING CTLEADS TO INFERIOR CONTROL RATES

BEAUMONT’S ART PROCESS
CL-PTV can be constructed within the first week of treatment
using feedback of imaging measurements
Single plan modification during second week can lead to dose
escalation

Divided into three groups based on PTV patient specific dose-
70.2-72.0, 72.0-75.6 ,75.6-79.2 (based on bladder and rectal dose
constraints)
Patients-280
180 patients (65%) were treated to a prostate field only and 99
patients (35%) to prostate and seminal vesiclesToxicity at the high dose level was not different from toxicity at
the intermediate or lower dose levels

DEVELOPING CL PATIENT SPECIFIC PTV
Brabbins et al, IJROBP
2007

IMPACT ON TUMOR CONTROL (N-3062)
Brabbins et al IJROBP
2008

‘PLAN OF THE DAY’
• Daily megavoltage (MV) imaging helped to choose the most
appropriate PTV encompassing bladder for the particular day
(using plan-of-the-day approach).
CONCLUSIONS:
• Adaptive IGRT using plan-of-the-day approach for bladder
preservation is clinically feasible, with good oncological outcomes
and low rates of acute and late toxicities. Dose escalation is safe
and possibly improves outcomes in bladder preservation.

N-54
3DCRT technique
4 plans generated by 10#
CBCT daily on 1st week and then every 5# (post RT also)
Without further bladder filling control or imaging, a CTV to PTV margin
of 7 mm is insufficient

N-
113
N-87 (77%)
N-
1274

No strong correlations were found between
V95%(total-dose) reduction and initial seroma volume
or between V95%(total-dose) reduction and seromavolume decrease

-28 patients
-Repeat CT scans were taken daily during 1st week f/b once
weekly
-Substantial systematic and random shape variation
demanded for a PTV margin up to 2.4 cm at the upper-
anterior part of the CTV. Plan adaptation after fraction 4
resulted in a maximum 0.7 cm margin reduction and a
significant PTV reduction from 1185 to 1023 cc

CT -planning CT -4
Conclusions: With adaptive radiotherapy, maximum required
PTV margins can be reduced from 2.4 to 1.7 cm, resulting in
significantly less dose to the bowel area