Embed Size (px)
Citation preview
Cytokine & Growth Factor Reviews 26 (2015) 221–228
IFN-b and multiple sclerosis: From etiology to therapy and back
V. Annibali a,1, R. Mechelli a,1, S. Romano a, M.C. Buscarinu a, A. Fornasiero a,R. Umeton a, V.A.G. Ricigliano a,b, F. Orzi c, E.M. Coccia d, M. Salvetti a,*, G. Ristori a
a Centre for Experimental Neurological Therapies (CENTERS), Neurology and Department of Neurosciences, Mental Health and Sensory Organs, Sapienza
University of Rome, Italyb Neuroimmunology Unit, Fondazione Santa Lucia-I.R.C.C.S., Rome, Italyc Neurology and Department of Neurosciences, Mental Health and Sensory Organs, Sapienza University of Rome, Italyd Department of Infectious, Parasitic and Immune-mediated Diseases, Istituto Superiore di Sanita, Rome, Italy
A R T I C L E I N F O
Article history:
Available online 31 October 2014
Keywords:
Multiple sclerosis
Interferon beta
Epstein–Barr virus
Human endogenous retroviruses
Genome-wide Association Studies
A B S T R A C T
Several immunomodulatory treatments are currently available for relapsing-remitting forms of multiple
sclerosis (RRMS). Interferon beta (IFN) was the first therapeutic intervention able to modify the course of
the disease and it is still the most used first-line treatment in RRMS.
Though two decades have passed since IFN-b was introduced in the management of MS, it remains a
valid approach because of its good benefit/risk profile. This is witnessed by new efforts of pharmaceutical
industry to improve this line: a PEGylated form of subcutaneous IFN-b 1a, (Plegridy1) with a longer half-
life, has been recently approved in RRMS.
This review will survey the various stages of the use of type I IFN in MS, with special attention to the
effect of the treatment on the supposed viral etiologic factors associated to the disease. The antiviral
activities of IFN (that initially prompted its use as immunomodulatory agent in MS), and the mounting
evidences in favor of a viral etiology in MS, allowed us to outline a re-appraisal from etiology to therapy
and back.
� 2014 Elsevier Ltd. All rights reserved.
Contents lists available at ScienceDirect
Cytokine & Growth Factor Reviews
jo ur n al ho mep ag e: www .e lsev ier . c om / loc ate /c yto g f r
1. Introduction
Multiple sclerosis (MS) is an inflammatory demyelinatingdisease of the central nervous system (CNS) characterized, in itsmost common clinical presentation, by an unpredictable occur-rence of relapse and remission phases [1–3]. The disease generallyaffects young adults [4], with a preference for female gender, as
Abbreviations: ARR, annualized relapse rate; CIS, clinically isolated syndrome; CNS,
central nervous system; EBNA, Epstein–Barr nuclear antigen; EBV, Epstein–Barr
virus; EDSS, expanded disability status scale; ELISA, enzyme-linked immunosor-
bent assay; GWAS, genome-wide association studies; HERV, human endogenous
retroviruses; HIV, human immunodeficiency virus; IFN, Interferon; IFNAR, IFN–areceptor; IPA, ingenuity pathway analysis; IRF, interferon regulatory factor; ISGF,
IFN-stimulated gene factor; JAK, Janus-family tyrosine kinases; LMP1, latent
membrane protein-1; MRI, magnetic resonance imaging; MS, multiple sclerosis;
MSRV, MS-associated retroviruses; MxA, myxovirus-induced protein A; NAbs,
neutralizing antibodies; 20 ,50-OAS, 20 ,50-oligoadenylate synthetase; PEG, polyeth-
ylene glycol; RAL, raltegravir; RR, relapsing–remitting forms; STAT, signal
transducers and activators of transcription; SNPs, single nucleotide polymor-
phisms; TLR, toll-like receptors; TYK, tyrosine kinase.
* Corresponding author at: Neurologia, Ospedale S. Andrea, Via di Grottarossa
1035, 00189 Rome, Italy. Tel.: +39 06 33775994; fax: +39 06 33775900.
E-mail address: [email protected] (M. Salvetti).1 These authors contributed equally to this work.
http://dx.doi.org/10.1016/j.cytogfr.2014.10.010
1359-6101/� 2014 Elsevier Ltd. All rights reserved.
observed in many other immune-mediated conditions. Being amultifactorial disorder, its etiology involves both genetic andenvironmental risk factors. So far, genome-wide associationstudies (GWAS) have shown that genetic predisposition to MS isdetermined by more than 100 disease-associated susceptibilitypolymorphisms, located in coding and non-coding DNA [5]. Path-way analyses on MS-related genes demonstrated a relation withcellular networks specifically involved in immune cell functioning,antiviral response and interferon (IFN) signaling [6].
Major environmental risk factors for MS include Epstein–Barrvirus (EBV) infection, the reactivation of human endogenousretroviruses (HERV) in specific conditions, vitamin D deficit andcigarette smoking, as supported by epidemiological surveys,serological evidences and other experimental laboratory basedstudies [7–13]. Nonetheless, a comprehensive overview of theevents leading to MS development is still lacking.
There is no cure for MS and treatments focus on treatingrelapses, slowing the progression of the disease and managingsymptoms. Several immunomodulatory and immunosuppressivetherapeutic agents are currently available for relapsing-remittingforms (RR) of MS, being interferon beta (IFN-b) the firsttherapeutic intervention able to interfere with the course of thedisease and still the most used first-line treatment in RR MS.

V. Annibali et al. / Cytokine & Growth Factor Reviews 26 (2015) 221–228222
2. From etiology. . .
The hypothesis of a viral etiology in MS led to severalinvestigations on a large number of microbes, that, after an initialenthusiastic attention, failed to be demonstrably associated to MS.At the moment two agents seem consistently linked to diseasesdevelopment: EBV and HERV.
Converging epidemiological, clinical and laboratory studiessupport an etiologic role for EBV in MS [14]. EBV is a g-herpesvirusthat infect quite all the adult population and that persists ininfected B cells in a latent or lytic phase [15]. Humans are theexclusive natural host for EBV which may explain why MS isunique to humans [16]. Prospective studies have shown thatelevation in serum antibody titers to EBV precedes the occurrenceof MS [17,18]. Epstein–Barr viral load in the peripheral blood ofhealthy adults may predict the risk of MS [19], while in childrenwho develop MS immunoreactivity to EBV, but not to other viruses,is higher than in controls [20,21]. A history of late EBV infectionand of infectious mononucleosis (IM is often the clinicalmanifestation of a late primary EBV infection) is stronglyassociated to MS [22]. EBV may be a target of oligoclonalcerebrospinal fluid IgG [23], CD8+ T cells [24–26] and CD4response [27], and a vast literature on the cross-reactivity betweenEBV and myelin epitopes was produced over the past two decades[28–30].
Recent works provided further evidences aimed at clarifyinghow EBV contributes to disease development. An inadequatecontrol of EBV at primary infection or at a later stage can lead tolow grade, persistently active EBV infection in CNS infiltrating Bcells [26,31–33]. A ‘‘candidate-interactome’’ aggregate analysis ofgenome-wide association data in multiple sclerosis demonstrateda significant enrichment of potential interactions between thevirus and MS-related genomic regions [34]. The EBV infection ofthe MS brain as cause of CNS damage that remains controversial[35–37], is supported by several recent studies demonstrating aselective enrichment of EBV-specific CD8+ T cells in thecerebrospinal fluid of MS patients [38,39] and the presence ofEBV DNA in brain (Mechelli et al., manuscript submitted).
Besides to role of herpesviruses many studies support apotential contribution for HERV to MS development. Retrovirusesare RNA viruses that may cause a spectrum of diseases of thenervous system. Their genome contains three genetic domains: env
is responsible for the surface glycoproteins and trans-membrane;gag encodes the proteins necessary for viral assembly, includingmatrix proteins and core shell; pol encodes the enzymes needed forviral replication, such as reverse transcriptase, protease, ribonu-clease and integrase [40].
Specific sequences within retroviral genes can lead to thedevelopment of neurovirulence, in particular, the proteins env-associated, which mediates the binding of the virus to the cellmembrane surface. Neurovirulent retroviruses are able to activatethe host immune response that, through pro-inflammatorymolecules and neurotoxic molecules, ultimately leads to neuronaldeath [40].
Table 1INF-b formulations approved for RRMS. For detailed description, see text.
Rebif 22/44
IFN subtype Beta 1a
Production CHO
Aminoacid 166 aa
Glycosylation 1 N-linked complex
Administration SC, 3 times/week
Weekly dose 66/132 mcg
CHO = Chinese hamster ovary cells; SC = subcutaneous; IM = intramuscular.
In 1997, Perron described the isolation and identification of newretrovirus particles from cell cultures of leptomeninges, choroidplexus and peripheral B lymphocytes in MS patients. This studyprovided molecular evidence that the production of extracellularvirions containing MS-associated retroviruses (MSRV) pol se-quence was associated with MS. This virus, previously called LM7,was a new retrovirus which was present in the cerebrospinal fluidof patients with MS [41]. The same group showed the production ofa specific envelope protein with gliotoxic and pro-inflammatoryactions that may be crucial in MS pathogenesis [42]. Furtherstudies have tried to explain and confirm the association betweenMS and the expression of MSRV envelope (Env), providingevidences that the retrovirus appears to be related to MS clinicalprogression [43,44]. Recently, env antigen was detected in theserum of 73% of MS patients with similar prevalence in all clinicalforms, and not in subjects affected by other inflammatory diseases.The different forms of the disease (primary-progressive, RR andclinically isolated syndrome-CIS) show different ELISA (enzyme-linked immunosorbent assay) and/or PCR profiles indicative of anincrease with the evolution of the disease [45].
3. To therapy. . .
Interferons were discovered by Isaacs and Lindenmann [46];they use this term to describe a soluble substance with biologicalactivity able to interfere with viral replication. Due to theirantiviral activities and considering the plausible viral etiology ofMS, IFNs, regardless of their type, were proposed as immunomod-ulatory therapeutic agents in MS patients.
The first trials using IFN-g (a type II IFN) were conducted in thelate 1980s and were interrupted because the treated patientsshowed an increase of severity and frequency of relapses[47,48]. These negative results led to study another type of IFNs(type I), IFN-a and IFN-b, that may act as inhibitors of IFN-g.Different preparations of IFN-a resulted in reduction of clinicalrelapses and activity at magnetic resonance imaging (MRI) in MSpatients, but unacceptable side effects precluded its use in clinicalpractice [49–53]. IFN-b was similarly effective in decreasingdisease activity and showed an acceptable risk profile, thusbecoming the first disease-modifying therapy for MS (Table 1).
Subcutaneous IFN-b 1b (Betaseron1) was the first immuno-modulatory therapy to receive approval for the treatment of RRMSin 1993. It is produced by recombinant DNA technology in thebacterial cell (Escherichia coli) and currently is the only IFN-blicensed for RR and secondary progressive (SP) MS [54]. In theregistration trial 372 patients were randomized to receive placeboor IFN-b 1b (50 or 250 mcg subcutaneously every other day) for2 years. The annualized relapse rate (ARR) was significantly lowerin the IFN-b1b treated groups compared to the placebo group witha dosage effect. Moreover a significative reduction of activity atMRI activity was showed. No difference in disease progressionbetween treatment and placebo groups was demonstrated [55,56].
IFN-b1a IM (Avonex1) is produced in Chinese hamster ovarycells and was approved for treatment in RRMS in 1996. In the
Avonex Betaferon/Betaseron/Extavia
Beta 1a Beta 1b
CHO E. coli
166 aa 165 aa
1 N-linked complex None
IM, 1 time/week SC, every other day
30 mcg 875 mcg

V. Annibali et al. / Cytokine & Growth Factor Reviews 26 (2015) 221–228 223
pivotal study 301 patients with expanded disability status scale(EDSS) score of 1.0–3.5 and at least two relapses in the preceding3 years were randomized to receive placebo or IFN-b 1a (30 mgintramuscularly once weekly) for 2 years [57,58]. The IFN-b 1agroup showed a significant decrease in the disease activitycompared with placebo.
IFN-b 1a SC (Rebif1) is also produced in mammalian Chinesehamster ovary cells using DNA technology. It was approved fortreatment of RRMS in 1998 in Europe and Canada and in 2002 inthe USA. In the PRISM study [59] 560 patients with an EDSS scorebetween 1.0 and 5.0 and at least two relapses in the preceding2 years were randomized to receive placebo or IFN-b 1a (22 or44 mg subcutaneously three times weekly). After 2 years oftreatment, IFN-b 1a showed significant results compared withplacebo in relapse rate and MRI activity with a statisticallysignificant dose-effect.
While the pivotal clinical trials consistently demonstrated thatboth forms of IFN-b reduce ARR by about 1/3 and new brain MRIlesions over periods of 1–3 years in RRMS, four randomized,placebo-controlled trials demonstrated poor or no effects onestablished progressive MS [54,60–63]. IFN-b has a significanteffect in the earlier inflammatory stages of the disease: three largeclinical trials (CHAMPS, ETOMS and BENEFIT) in CIS patients,demonstrated an effect on clinical and MRI measures of diseaseactivity delaying the development to clinically definite (CD) MS[64–66]. Although these studies had limited comparability becauseof different patient populations recruited (BENEFIT and ETOMSenrolled patients with multifocal manifestations at onset, whileCHAMPS enrolled patients with monofocal forms), the risk ofprogression to CDMS was comparably reduced by 40–50%.
Considering the different formulations of IFN-b, head-to-headtrials were conducted to compare the different licensed IFNs(EVIDENCE and INCOMIN). These studies demonstrated thatincreasing the dose of IFN-b (more frequent dosing schedule orhigher dose) gave greater benefit than lower doses, supporting adose–response relationship [67,68].
The IFNs-b are generally well tolerated, being the mostfrequent side effects injection-site reaction, and a flu-likesyndrome that tends to wanes over time in most patients.Lymphopenia, hepatic failure, hepatitis, and elevated liverenzymes have also been reported especially during IFN-b-1btreatment [69]. Though IFN-b therapy represents a significantadvance in the management of MS, the treatment response is notuniform and clinical experience shows that about 40% of the MSpatients do not or only poorly respond to IFN-b treatment (‘‘non-responders’’) [70]. So far there are no established biologicalmarkers able to predict the response. The development ofneutralizing antibodies (NAbs), which at high titers may blockthe biological response of the drug with a reduced efficacy, cancontribute to treatment failure [71,72]. Persistent high-titers ofNAbs depend on the formulation and dosing regimen, and occurmore commonly with subcutaneous preparations [73].
IFN was tried in MS as a ‘general’ antiviral approach and gavepositive results as disease modifying therapy. This was not the casewith more ‘specific’ antiviral treatment such as those active onherpes viruses. Over the last twenty years several clinical trialshave been carried out especially with acyclovir and valacyclovir[74–76]. Overall, these studies did not obtain significant results infavor of the drug compared to placebo, though positive trends werenoted. An analysis that also took into account the pharmacokineticof acyclovir and valacyclovir suggested an inhibitory effect onsome viruses (Herpes viruses 1, 2, 6 and varicella zoster virus) butnot on others that seem to have a greater correlation with MS (EBV,Herpes virus 6, and MSRV), thus explaining, at least in part, thefailure of this approach [77]. Further studies with new antiviraldrugs having improved pharmacological characteristics and
antiretroviral activity may result in better outcome and arecurrently actively investigated (see Raltegravir in next section).
4. And back. . .
4.1. MS genome-wide association studies and IFN-b pathway
The exact mode of action of IFN-b in MS is likely to be complexand is not yet fully understood. This topic will be not treated in thepresent review, being object of other contributions in this issue. Atthe molecular level IFN-b is recognized by the IFN-a receptor(IFNAR), which is found on many different cell types. The receptoris a heterodimer formed by IFNAR1 and IFNAR2, which assembleinto a functional receptor complex and initiates the signaltransduction pathway that involves the phosphorylation of severalintracellular mediators. Upon assembly of the IFN receptorcomplex, the intracellular domains of IFNAR1 and IFNAR2 activeJanus kinases 1 (JAK1) and tyrosine kinase 2 (TYK2). The JAK1/TYK2along with IFNAR, phosphorylate signal transducers and activatorsof transcription (STAT) 1, and 2, which dimerize and form acomplex with interferon regulatory factor 9 (IRF9). The STA-T1:2:IRF9 complex is a transcription factor (IFN-stimulated genefactor, ISGF3), which translocates to the nucleus and binds to theIFN-stimulated response element (ISRE) of multiple genes[78]. Different kinds of genes are targeted by ISGF3 complex,including early genes such as IFN regulatory factor-1 (IRF-1), theprimary positive regulator of IFN production, and IRF-2, aninhibitor of IFN production. The later genes include the IFN-bitself and antiviral proteins such as 20,50-oligoadenylate synthetase(20,50-OAS) and myxovirus-induced protein A (MxA), which arespecifically induced by type I IFNs. MxA is the established markerof IFN-b biological activity in IFN-b-treated MS patients [79].
Some genes related to the IFN-b signaling pathway showedsingle nucleotide polymorphisms (SNPs) that resulted to be MS-associated in GWAS [5]. To review this, we highlighted the networkthat leads to the connectivity between the IFN-b signalingpathway and genes exceeding the genome-wide significancethreshold in GWAS published from 2007 in MS (http://www.ge-nome.gov/gwastudies/). To perform this analysis it was usedQuigen Ingenuity Pathway Analysis (IPA), which was set to run a‘‘core analysis’’ correlating all MS-associated genes (retrieved on 8/26/2014) with the known interactors of IFN-b (314 moleculespresent in IPA version 21249400); the analysis included onlyexperimental evidence observed in human samples. Among allknown interactors of IFN-b, 18 genes were also MS-associated(Table 2 and Fig. 1, that shows most of these connections and howthey relate to IFN-b). The list includes several genes that controlthe immune responses (including major histocompatibilitycomplex alleles, cytokines and co-stimulator molecules), as wellas direct interactors with IFN signaling such as IRF8, NFKB1 andTYK2 [80,81]. This IPA analysis showed a significant (p-value < 1.18 � 10�7) relationship between the MS-associatedgenes and the IFN-b signaling and confirmed previous resultsobtained by our group with another approach [6]. Overall, thesedata suggest that single unfavorable SNPs (or a combination ofthem) affecting components of IFN-b signaling may determinesome deregulation in MS. Further investigation are needed toclarify the role of these components in MS pathogenesis andpossible corrective effects of exogenous IFN-b on deregulatedpathways (see next section).
4.2. EBV and IFN-b
EBV is a kind of ‘‘one man band’’ in its ability to control theantiviral immune response of infected cells both in lytic and latentphase. IFN pathway is no exception, being sabotaged by multiple
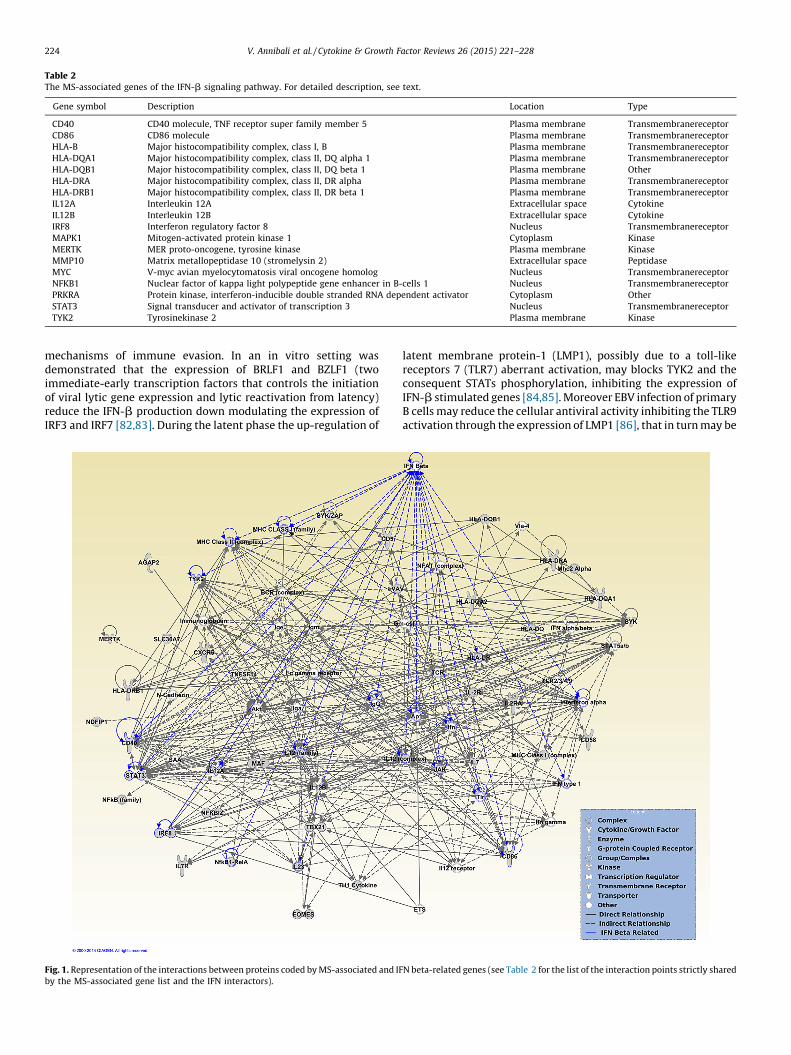
Table 2The MS-associated genes of the IFN-b signaling pathway. For detailed description, see text.
Gene symbol Description Location Type
CD40 CD40 molecule, TNF receptor super family member 5 Plasma membrane Transmembranereceptor
CD86 CD86 molecule Plasma membrane Transmembranereceptor
HLA-B Major histocompatibility complex, class I, B Plasma membrane Transmembranereceptor
HLA-DQA1 Major histocompatibility complex, class II, DQ alpha 1 Plasma membrane Transmembranereceptor
HLA-DQB1 Major histocompatibility complex, class II, DQ beta 1 Plasma membrane Other
HLA-DRA Major histocompatibility complex, class II, DR alpha Plasma membrane Transmembranereceptor
HLA-DRB1 Major histocompatibility complex, class II, DR beta 1 Plasma membrane Transmembranereceptor
IL12A Interleukin 12A Extracellular space Cytokine
IL12B Interleukin 12B Extracellular space Cytokine
IRF8 Interferon regulatory factor 8 Nucleus Transmembranereceptor
MAPK1 Mitogen-activated protein kinase 1 Cytoplasm Kinase
MERTK MER proto-oncogene, tyrosine kinase Plasma membrane Kinase
MMP10 Matrix metallopeptidase 10 (stromelysin 2) Extracellular space Peptidase
MYC V-myc avian myelocytomatosis viral oncogene homolog Nucleus Transmembranereceptor
NFKB1 Nuclear factor of kappa light polypeptide gene enhancer in B-cells 1 Nucleus Transmembranereceptor
PRKRA Protein kinase, interferon-inducible double stranded RNA dependent activator Cytoplasm Other
STAT3 Signal transducer and activator of transcription 3 Nucleus Transmembranereceptor
TYK2 Tyrosinekinase 2 Plasma membrane Kinase
V. Annibali et al. / Cytokine & Growth Factor Reviews 26 (2015) 221–228224
mechanisms of immune evasion. In an in vitro setting wasdemonstrated that the expression of BRLF1 and BZLF1 (twoimmediate-early transcription factors that controls the initiationof viral lytic gene expression and lytic reactivation from latency)reduce the IFN-b production down modulating the expression ofIRF3 and IRF7 [82,83]. During the latent phase the up-regulation of
Fig. 1. Representation of the interactions between proteins coded by MS-associated and IF
by the MS-associated gene list and the IFN interactors).
latent membrane protein-1 (LMP1), possibly due to a toll-likereceptors 7 (TLR7) aberrant activation, may blocks TYK2 and theconsequent STATs phosphorylation, inhibiting the expression ofIFN-b stimulated genes [84,85]. Moreover EBV infection of primaryB cells may reduce the cellular antiviral activity inhibiting the TLR9activation through the expression of LMP1 [86], that in turn may be
N beta-related genes (see Table 2 for the list of the interaction points strictly shared

V. Annibali et al. / Cytokine & Growth Factor Reviews 26 (2015) 221–228 225
up-regulated by Epstein–Barr nuclear antigen 2 (EBNA2). Thisprotein is able to control gene expression of viral and cellulargenes, mainly during the first phase of the infection [87]. Someevidences suggest its potential implication in MS pathology:EBNA2 expressing cells have been observed in affected brains [31]and specific EBNA2 genotypes associate with disease status [88].
It seems plausible that IFN-b therapy may compensate forsome of the EBV-induced dysfunctions in the antiviral immuneresponses: CD8+ T cells specific for lytic-phase antigens aredetected with high frequency in the peripheral blood of patientswith active disease and are reduced by IFN-b treatment [26], aswell as CD4+ T cell response to EBNA1 peptides pool [89]; indendritic cells obtained from MS patients under IFN-b treatment areduced TLR9 activation (that promote pro-inflammatoryresponses) was observed [90]; a recent work demonstrated animpaired activation of TLR7 in MS subjects, that decrease theability of B cells to mature in plasma cells and that is restored byIFN-b treatment [91].
4.3. MSRV and IFN-b
IFN-b appears to be capable of interfering with MSRV biology.An in vitro study showed that IFN-b inhibits the release of MSRVfrom peripheral blood mononuclear cells derived from MS patients[92]. These data were confirmed through a longitudinal evaluationof patients with MS, during one year of therapy with IFN-b: theMSRV load in the blood was directly related to the duration of MSand underwent a considerable reduction to below the limits ofdetection within 3 months of IFN therapy; this work suggested toconsider the evaluation of MSRV in plasma as a prognostic markerto monitor the progression of the disease and the outcome oftherapy [43].
At variance with several trials conducted with anti-herpesdrugs, and notwithstanding evidences of retroviral contribution todisease pathogenesis, no major attempt has been performed withanti-retroviral therapy in MS, except for a humanized monoclonalantibody against the envelope of MSRV, that was tried in a phase Istudy [93]. A pilot study, that is ongoing, may herald such anapproach, investigating raltegravir (RAL) in relapsing remitting MS(ClinicalTrials.gov Identifier: NCT01767701).
RAL is an inhibitor of human immunodeficiency virus (HIV)integrase, approved in 2007 for clinical use as antiretroviral agentin HIV infected adults. Clinical studies and subsequent clinicalexperience have shown durable virologic suppression, low rates ofadverse effects and long-term safety. Not interacting with thecytochrome P450 system, RAL may be a good option forpolytherapy. As an inhibitor of retroviral integrase, RAL can beactive against the MSRV that is transactivated by several viruses,EBV being one of these. RAL is also able to inhibit recombinase andterminase, two key proteins for EBV [94]. Altogether, RAL seems tobe a good candidate to tackle plausible etiologic agents for MS andmight also add to the effects of IFN.
5. Conclusions
Though two decades have passed since IFN-b was introduced inthe management of MS, it remains a valid approach because of itsgood benefit/risk profile. The persisting interest is witnessed bynew efforts that pharmaceutical industry has produced to improvethis line.
Recently, a PEGylated form of subcutaneous IFN-b 1a (Ple-gridy1) with a longer half-life (injection frequency every 2 weeks)has been approved in RRMS. Conjugation of IFN-b 1a with amolecule of polyethylene glycol (PEG; PEGylation) increases thesize of the product resulting in more solubility, half-life andefficacy the drug. Compared to placebo, PEG INF has reduced ARR
by about one-third (0.397 in the placebo group versus 0.256 in theevery 2 weeks group). A slight reduction in sustained disabilityprogression and in several MRI activity measures has also beendemonstrated. The drug was generally well tolerated: the mostcommon adverse events were influenza-like illness, injection-sitereactions and headache [95]. Due to its frequency of administra-tion (every 2 weeks), PEG IFN-b1a may have a better safety profilethan other IFNs-b formulations. Moreover, results from theextension of the phase III study showed that the therapeuticeffects of PLEGRIDY may reach a size that was not attained byincreasing doses of non-pegylated IFN-b and may become evenmore relevant over time, suggesting that prolonged treatment withPLEGRIDY may induce therapeutic effects that go beyond theimmunomodulatory action of IFN-b.
Given the potent antiviral effects of type-1 IFN, the added valueof PLEGRIDY treatment might be related to its ability to target moreefficiently the non-heritable (i.e. viral) cause(s) of MS. This hints atfuture therapeutic approaches based on type 1 interferon alone orin association with specific antiviral drugs that might act as anetiologic treatment for MS.
The main fields of investigation regard:
(a) etiopathogenesis of multiple sclerosis;(b) the identification of the world’s largest twin registry in Italian
population; the registry is currently exploited for concordancestudies and for laboratory investigations (studies on twin pairsdiscordant for disease); and
(c) clinical trials (especially phase II independent studies) inpatients with multiple sclerosis, Huntington disease andcerebellar ataxia.
Conflict of interest
MS receives research support and has received fees as speakerfrom Sanofi-Aventis, Biogen, Bayer Schering, and Merck Serono.
Acknowledgements
MS is supported from: Italian Multiple Sclerosis Foundation(Fondazione Italiana Sclerosi Multipla grant number: 2011/R/31)and Italian Ministry of Health (Ministero della Salute, grantnumber: RF-2010-2321254).
References
[1] Amato MP, Ponziani G, Bartolozzi ML, Siracusa G. A prospective study on thenatural history of multiple sclerosis: clues to the conduct and interpretation ofclinical trials. J Neurol Sci 1999;168:96–106.
[2] Scalfari A, Neuhaus A, Degenhardt A, Rice GP, Muraro PA, Daumer M, et al. Thenatural history of multiple sclerosis, a geographically based study: relapsesand long-term disability. Brain 2010;133:1914–29.
[3] Bordi I, Umeton R, Ricigliano VA, Annibali V, Mechelli R, Ristori G, et al. Amechanistic, stochastic model helps understand multiple sclerosis course andpathogenesis. Int J Genomics 2013;2013:910321.
[4] Koch-Henriksen N. The Danish multiple sclerosis registry: a 50-year follow-up.Mult Scler 1999;5:293–6.
[5] International Multiple Sclerosis Genetics Consortium (IMSGC), Beecham AH,Patsopoulos NA, Xifara DK, Davis MF, Kemppinen A, et al. Analysis of immune-related loci identifies 48 new susceptibility variants for multiple sclerosis. NatGenet 2013;45:1353–60.
[6] Ricigliano VA, Umeton R, Germinario L, Alma E, Briani M, Di Segni N, et al.Contribution of genome-wide association studies to scientific research: apragmatic approach to evaluate their impact. PLOS ONE 2013;8:e71198.
[7] Kakalacheva K, Lunemann JD. Environmental triggers of multiple sclerosis.FEBS Lett 2011;585:3724–9.
[8] Pender MP. The essential role of Epstein–Barr virus in the pathogenesis ofmultiple sclerosis. Neuroscientist 2011;17:351–67.
[9] Almohmeed YH, Avenell A, Aucott L, Vickers MA. Systematic review and meta-analysis of the sero-epidemiological association between Epstein Barr virusand multiple sclerosis. PLOS ONE 2013;8:e61110.
[10] Simon KC, Munger KL, Ascherio A. Vitamin D and multiple sclerosis: epidemi-ology, immunology, and genetics. Curr Opin Neurol 2012;25:246–51.
V. Annibali et al. / Cytokine & Growth Factor Reviews 26 (2015) 221–228226
[11] Handel AE, Williamson AJ, Disanto G, Dobson R, Giovannoni G, RamagopalanSV. Smoking and multiple sclerosis: an updated meta-analysis. PLoS ONE2011;6:e16149.
[12] Sutkowski N, Conrad B, Thorley-Lawson DA, Huber BT. Epstein–Barr virustransactivates the human endogenous retrovirus HERV-K18 that encodes asuperantigen. Immunity 2001;15:579–89.
[13] Antony JM, Deslauriers AM, Bhat RK, Ellestad KK, Power C. Human endogenousretroviruses and multiple sclerosis: innocent bystanders or disease determi-nants. Biochim Biophys Acta 2011;1812:162–76.
[14] Lunemann JD. Epstein–Barr virus in multiple sclerosis: a continuing conun-drum. Neurology 2012;78:11–2.
[15] Cohen JI. Epstein–Barr virus infection. N Engl J Med 2000;343:481–92.[16] Haahr S, Hollsberg P. Multiple sclerosis is linked to Epstein–Barr virus infec-
tion. Rev Med Virol 2006;16:297–310.[17] Levin LI, Munger KL, Rubertone MV, Peck CA, Lennette ET, Spiegelman D, et al.
Temporal relationship between elevation of Epstein–Barr virus antibody titersand initial onset of neurological symptoms in multiple sclerosis. JAMA2005;293:2496–500.
[18] DeLorenze GN, Munger KL, Lennette ET, Orentreich N, Vogelman JH, AscherioA. Epstein–Barr virus and multiple sclerosis: evidence of association from aprospective study with long-term follow-up. Arch Neurol 2006;63:839–44.
[19] Wagner HJ, Munger KL, Ascherio A. Plasma viral load of Epstein–Barr virus andrisk of multiple. Eur J Neurol 2004;11:833–4.
[20] Alotaibi S, Kennedy J, Tellier R, Stephens D, Banwell B. Epstein–Barr virus inpediatric multiple sclerosis. JAMA 2004;291:1875–9.
[21] Banwell B, Krupp L, Kennedy J, Tellier R, Tenembaum S, Ness J, et al. Clinicalfeatures and viral serologies in children with multiple sclerosis: a multina-tional observational study. Lancet Neurol 2007;6:773–81.
[22] Handel AE, Williamson AJ, Disanto G, Handunnetthi L, Giovannoni G, Rama-gopalan SV. An updated meta-analysis of risk of multiple sclerosis followinginfectious mononucleosis. PLoS ONE 2010;5(9).
[23] Cepok S, Zhou D, Srivastava R, Nessler S, Stei S, Bussow K, et al. Identification ofEpstein–Barr virus proteins as putative targets of the immune response inmultiple sclerosis. J Clin Invest 2005;115:1352–60.
[24] Jilek S, Schluep M, Meylan P, Vingerhoets F, Guignard L, Monney A, et al. StrongEBV-specific CD8+ T-cell response in patients with early multiple sclerosis.Brain 2008;131:1712–21.
[25] Jilek S, Schluep M, Harari A, Canales M, Lysandropoulos A, Zekeridou A, et al.HLAB7-restricted EBV specific CD8+ T cells are dysregulated in multiplesclerosis. J Immunol 2012;188:4671–80.
[26] Angelini DF, Serafini B, Piras E, Severa M, Coccia EM, Rosicarelli B, et al.Increased CD8+ T cell response to Epstein–Barr virus lytic antigens in theactive phase of multiple sclerosis. PLOS Pathog 2013;9:e1003220.
[27] Lunemann JD, Edwards N, Muraro PA, Hayashi S, Cohen JI, Munz C, et al.Increased frequency and broadened specificity of latent EBV nuclear antigen-1-specific T cells in multiple sclerosis. Brain 2006;129:1493–506.
[28] Ufret-Vincenty RL, Quigley L, Tresser N, Pak SH, Gado A, Hausmann S, et al. Invivo survival of viral antigen-specific T cells that induce experimental auto-immune encephalomyelitis. J Exp Med 1998;188:1725–38.
[29] Lunemann JD, Jelcic I, Roberts S, Lutterotti A, Tackenberg B, Martin R, et al.EBNA1-specific T cells from patients with multiple sclerosis cross react withmyelin antigens and co-produce IFN-gamma and IL-2. J Exp Med2008;205:1763–73.
[30] Lang HL, Jacobsen H, Ikemizu S, Andersson C, Harlos K, Madsen L, et al. Afunctional and structural basis for TCR cross-reactivity in multiple sclerosis.Nat Immunol 2002;3:940–3.
[31] Serafini B, Rosicarelli B, Franciotta D, Magliozzi R, Reynolds R, Cinque P, et al.Dysregulated Epstein–Barr virus infection in the multiple sclerosis brain. J ExpMed 2007;204:2899–912.
[32] Serafini B, Severa M, Columba-Cabezas S, Rosicarelli B, Veroni C, Chiappetta G,et al. Epstein–Barr virus latent infection and BAFF expression in B cells in themultiple sclerosis brain: implications for viral persistence and intrathecal B-cell activation. J Neuropathol Exp Neurol 2010;69:677–93.
[33] Serafini B, Muzio L, Rosicarelli B, Aloisi F. Radioactive in situ hybridization forEpstein–Barr virus-encoded small RNA supports presence of Epstein–Barrvirus in the multiple sclerosis brain. Brain 2013;136:e233.
[34] Mechelli R, Umeton R, Policano C, Annibali V, Coarelli G, Ricigliano VA, et al. Acandidate-interactome aggregate analysis of genome-wide association data inmultiple sclerosis. PLOS ONE 2013;8:e63300.
[35] Aloisi F, Serafini B, Magliozzi R, Howell OW, Reynolds R. Detection of Epstein–Barr virus and B-cell follicles in the multiple sclerosis brain: what you finddepends on how and where you look. Brain 2010;133:e157.
[36] Lassmann H, Niedobitek G, Aloisi F, Middeldorp JM, NeuroproMiSe EBV WorkingGroup. Epstein–Barr virus in the multiple sclerosis brain: a controversial issue—report on a focused workshop held in the Centre for Brain Research of theMedical University of Vienna, Austria. Brain 2011;134:2772–86.
[37] Tzartos JS, Khan G, Vossenkamper A, Cruz-Sadaba M, Lonardi S, Sefia E, et al.Association of innate immune activation with latent Epstein–Barr virus inactive MS lesions. Neurology 2012;78:15–23.
[38] Jaquiery E, Jilek S, Schluep M, Meylan P, Lysandropoulos A, Pantaleo G, et al.Intrathecal immune responses to EBV in early MS. Eur J Immunol2010;40:878–87 [Erratum in: Eur J Immunol 2011; 41:1501].
[39] Lossius A, Johansen JN, Vartdal F, Robins H, Jurate Saltyte B, Holmøy T, et al.High-throughput sequencing of TCR repertoires in multiple sclerosis revealsintrathecal enrichment of EBV-reactive CD8(+) T cells. Eur J Immunol 2014,August [Epub ahead of print].
[40] Power C. Retroviral diseases of the nervous system: pathogenic host responseor viral gene-mediated neurovirulence? Trends Neurosci 2001;24:162–9.
[41] Perron H, Garson JA, Bedin F, Beseme FG, Paranhos-Baccala G, Komurian-Pradel F, et al. Molecular identification of a novel retrovirus repeatedly isolatedfrom patients with multiple sclerosis. Proc Natl Acad Sci U S A 1997;94:7583–8.
[42] Rieger F, Amouri R, Benjelloun N, Cifuentes-Diaz C, Dobransky T, Lyon-Caen O,et al. Gliotoxic factor and multiple sclerosis. C R Acad Sci 1996;319:343–50.
[43] Mameli G, Serra C, Astone V, Castellazzi M, Poddighe L, Fainardi E, et al.Inhibition of multiple-sclerosis-associated retrovirus as biomarker of inter-feron therapy. J Neurovirol 2008;14:73–7.
[44] Antony JM, van Marle G, Opii W, Butterfield DA, Mallet F, Yong VW, et al.Human endogenous retrovirus glycoprotein-mediated induction of redoxreactants causes oligodendrocyte death and demyelination. Nat Neurosci2004;7:1088–95.
[45] Perron H, Germi R, Bernard C, Garcia-Montojo M, Deluen C, Farinelli L, et al.Human endogenous retrovirus type W envelope expression in blood and braincells provides new insights into multiple sclerosis disease. Mult Scler 2012;18:1721–36.
[46] Isaacs A, Lindenmann J. Virus interference: I. The interferon. Proc R Soc Lond B:Biol Sci 1957;147:258–67.
[47] Pantich HS, Hirsch RL, Schindler J, Johnson KP. Treatment of multiple sclerosiswith gamma-interferons: exacerbations associated with activation on im-mune system. Neurology 1987;37:1097–102.
[48] Pantich HS, Hirsch RL, Haley AS, Johnson KP. Exacerbations of multiplesclerosis in patients treated with gamma-interferon. Lancet 1987;1:893–5.
[49] Knobler RL, Panitch HS, Braheny SL, Sipe JC, Rice GP, Huddlestone JR, et al.Systemic alpha-interferontherapy of multiple sclerosis. Neurology 1984;34:1273–9.
[50] Panitch HS. Systemic alpha-interferon in multiple sclerosis. Long-term patientfollow-up. Arch Neurol 1987;44:61–3.
[51] Camenga DL, Johnson KP, Alter M, Engelhardt CD, Fishman PS, Greenstein JI,et al. Systemic recombinant alpha-2 interferon therapy in relapsing multiplesclerosis. Arch Neurol 1986;43:1239–46.
[52] Durelli L, Bongioanni MR, Cavallo R, Ferrero B, Ferri R, Ferrio MF, et al. Chronicsystemic high-dose recombinant interferon alfa-2a reduces exacerbation rate.MRI signs of disease activity, and lymphocyte interferon gamma production inrelapsing–remitting multiple sclerosis. Neurology 1994;44(3 Pt 1):406–13.
[53] Durelli L, Bongioanni MR, Ferrero B, Ferri R, Imperiale D, Bradac GB, et al.Interferon alpha-2a treatment of relapsing–remitting multiple sclerosis: dis-ease activity resumes after stopping treatment. Neurology 1996;47:123–9.
[54] European Study Group on Interferon Beta-1b in Secondary Progressive MS.Placebo-controlled multicentre randomised trial of interferon beta-1b intreatment of secondary progressive MS. Lancet 1998;352:1491–7.
[55] The IFNB Multiple Sclerosis Study Group. Interferon b-1b is effective in relaps-ing–remitting multiple sclerosis: I. Clinical results of a multicenter, randomized,double-blind, placebo-controlled trial. Neurology 1993;43:655–61.
[56] Paty DW, Li DK. Interferon beta lb is effective in relapsing–remitting multiplesclerosis: II. MRI analysis results of a multicenter, randomized, double-blind,placebo-controlled trial. Neurology 1993;43:662–7.
[57] Rudick RA, Goodkin DE, Jacobs LD, Cookfair DL, Herndon RM, Richert JR, et al.Impact of interferon beta-1a on neurologic disability in relapsing multiplesclerosis. The Multiple Sclerosis Collaborative Research Group (MSCRG). Neu-rology 1997;49:358–63.
[58] Simon JH, Jacobs LD, Campion M, Wende K, Simonian N, Cookfair DL, et al.Magnetic resonance studies of intramuscular interferon beta-1a for relapsingmultiple sclerosis. The Multiple Sclerosis Collaborative Research Group. AnnNeurol 1998;43:79–87.
[59] PRISMS (Prevention of Relapses Disability by Interferon beta-1a Subcutane-ously in Multiple Sclerosis) Study Group. Randomised double-blind placebo-controlled study of interferon beta-1a in relapsing/remitting multiple sclero-sis. Lancet 1998;352:1498–504.
[60] Panitch H, Miller A, Paty D, Weinshenker B, North American Study Group onInterferon beta-1b in Secondary Progressive MS. Interferon beta-1b in sec-ondary progressive MS: results from a 3-year controlled study. Neurology2004;63:1788–95.
[61] Secondary Progressive Efficacy Clinical Trial of Recombinant Interferon-beta-1ain MS (SPECTRIMS) Study Group. Randomized controlled trial of interferon-beta-1a in secondary progressive MS: clinical results. Neurology 2001;56:1496–504.
[62] Li DK, Zhao GJ, Paty DW, University of British Columbia MS/MRI AnalysisResearch Group The SPECTRIMS Study Group. Randomized controlled trial ofinterferon-beta-1a in secondary progressive MS: MRI results. Neurology2001;56:1505–13.
[63] Cohen JA, Cutter GR, Fischer JS, Goodman AD, Heidenreich FR, Kooijmans MF,et al. Benefit of interferon beta-1a on MSFC progression in secondary progres-sive MS. Neurology 2002;59:679–87.
[64] Jacobs LD, Beck RW, Simon JH, Kinkel RP, Brownscheidle CM, Murray TJ, et al.Intramuscular interferon-beta-1a therapy initiated during a first demyelinat-ing event in multiple sclerosis. N Engl J Med 2000;343:898–904.
[65] Comi G, Filippi M, Barkhof F, Durelli L, Edan G, Fernandez O, et al. Effect of earlyinterferon treatment on conversion to definite multiple sclerosis: a random-ized study. Lancet 2001;357:1576–82.
[66] Kappos L, Polman CH, Freedman MS, Edan G, Hartung HP, Miller DH, et al.Treatment with interferon beta-1b delays conversion to clinically definite andMcDonald MS in patients with clinically isolated syndromes. Neurology2006;67:1242–9.

V. Annibali et al. / Cytokine & Growth Factor Reviews 26 (2015) 221–228 227
[67] Panitch H, Goodin DS, Francis G, Chang P, Coyle PK, O’Connor P, et al.Randomized, comparative study of interferon b-1a treatment regimens inMS. The EVIDENCE Trial. Neurology 2002;59:1496–506.
[68] Durelli L, Verdun E, Barbero P, Bergui M, Versino E, Ghezzi A, et al. Every-other-day interferon beta-1b versus once-weekly interferon beta-1a for multiplesclerosis: results of a 2-year prospective randomized multicentre study(INCOMIN). Lancet 2002;359:1453–60.
[69] McGraw CA, Lublin FD. Interferon beta and glatiramer acetate therapy. Neu-rotherapeutics 2013;10:2–18.
[70] Rudick RA, Lee JC, Simon J, Ransohoff RM, Fisher E. Defining interferonbeta response status in multiple sclerosis patients. Ann Neurol 2004;56:548–55.
[71] Ross C, Clemmesen K, Svenson M, Sørensen PS, Koch-Henriksen N, SkovgaardGL, et al. Immunogenicity of interferon-beta in multiple sclerosis patients:influence of preparation, dosage, dose frequency, and route of administration.Ann Neurol 2000;48:706–12.
[72] Calabresi PA, Kieseier BC, Arnold DL, Balcer LJ, Boyko A, Pelletier J, et al. Pegylatedinterferon b-1a for relapsing–remitting multiple sclerosis (ADVANCE): a ran-domised, phase 3, double-blind study. Lancet Neurol 2014;13:657–65.
[73] Kappos L, Clanet M, Sandberg-Wollheim M, Radue EW, Hartung HP, Hohlfeld R,et al. Neutralizing antibodies and efficacy of interferon beta-1a: a 4-yearcontrolled study. Neurology 2005;65:40–7.
[74] Lycke J, Svennerholm B, Hjelmquisit E, Frisen L, Badr G, Andersson M, et al.Acyclovir treatment of relapsing–remitting multiple sclerosis a randomized,placebo-controlled, double-blind study. J Neurol 1996;243:214–24.
[75] Bech E, Lycke J, Gadeberg P, Hansen HJ, Malmestrom C, Andersen O, et al. Arandomized, double-blind, placebo-controlled MRI study of anti-herpes virustherapy in MS. Neurology 2002;58:31–6.
[76] Friedman JE, Zabriskie JB, Plank C, Ablashi D, Whitman J, Shahan B, et al. Arandomized clinical trial of valacyclovir in multiple sclerosis. Mult Scler2005;11:286–95.
[77] Lycke J, Andersen O, Svennerholm B, Appelgren L, Dahllof C. Acyclovir con-centrations in serum and cerebrospinal fluid at steady state. J AntimicrobChemother 1989;24:947–54.
[78] Ivashkiv LB, Donlin LT. Regulation of type I interferon responses. Nat RevImmunol 2014;14:36–49.
[79] Killestein J, Polman CH. Determinants of interferon b efficacy in patients withmultiple sclerosis. Nat Rev Neurol 2011;7(4):221–8.
[80] Taniguchi T, Takaoka A. A weak signal for strong responses: interferon-alpha/beta revisited. Nat Rev Mol Cell Biol 2001;2:378–86.
[81] Li P, Wong JJ, Sum C, Sin WX, Ng KQ, Koh MB, et al. IRF8 and IRF3 cooperativelyregulate rapid interferon-b induction in human blood monocytes. Blood2011;117:2847–54.
[82] Bentz GL, Liu R, Hahn AM, Shackelford J, Pagano JS. Epstein–Barr virus BRLF1inhibits transcription of IRF3 and IRF7 and suppresses induction of interferon-beta. Virology 2010;402:121–8.
[83] Hahn AM, Huye LE, Ning S, Webster-Cyriaque J, Pagano JS. Interferon regula-tory factor 7 is negatively regulated by the Epstein–Barr virus immediate-earlygene, BZLF-1. J Virol 2005;79:10040–52.
[84] Valente RM, Ehlers E, Xu D, Ahmad H, Steadman A, Blasnitz L, et al. Toll-likereceptor 7 stimulates the expression of Epstein–Barr virus latent membraneprotein 1. PLoS ONE 2012;7:e43317.
[85] Ning S, Hahn AM, Huye LE, Pagano JS. Interferon regulatory factor 7 regulatesexpression of Epstein–Barr virus latent membrane protein 1: a regulatorycircuit. J Virol 2003;77:9359–68.
[86] Fathallah I, Parroche P, Gruffat H, Zannetti C, Johansson H, Yue J, et al. EBVlatent membrane protein 1 is a negative regulator of TLR9. J Immunol2010;185:6439–47.
[87] Zhao B, Zou J, Wang H, Johannsen E, Peng CW, Quackenbush J, et al. Epstein–Barr virus exploits intrinsic B-lymphocyte transcription programs to achieveimmortal cell growth. Proc Natl Acad Sci U S A 2011;108:14902–07.
[88] Mechelli R, Manzari C, Policano C, Annese A, Picardi E, Umeton R, et al. Epstein-Barr virus genetic variants associated with multiple sclerosis. Neurology 2014.Manuscript submitted.
[89] Comabella M, Kakalacheva K, Rıo J, Munz C, Montalban X, Lunemann JD. EBV-specific immune responses in patients with multiple sclerosis responding toIFNb therapy. Mult Scler 2012;18:605–9.
[90] Balashov KE, Aung LL, Vaknin-Dembinsky A, Dhib-Jalbut S, Weiner HL. Inter-feron-b inhibits toll-like receptor 9 processing in multiple sclerosis. AnnNeurol 2010;68:899–906.
[91] Giacomini E, Severa M, Rizzo F, Mechelli R, Annibali V, Ristori G, et al. IFN-btherapy modulates B-cell and monocyte crosstalk via TLR7 in multiple sclero-sis patients. Eur J Immunol 2013;43:1963–72.
[92] Serra C, Mameli G, Arru G, Sotgiu S, Rosati G, Dolei A. In vitro modulation of themultiple sclerosis (MS)-associated retrovirus by cytokines: implications forMS pathogenesis. J Neurovirol 2003;9:637–43.
[93] Curtin F, Lang AB, Perron H, Laumonier M, Vidal V, Porchet HC, et al. GNbAC1, ahumanized monoclonal antibody against the envelope protein of multiplesclerosis-associated endogenous retrovirus: a first-in-humans randomizedclinical study. Clin Ther 2012;34:2268–78.
[94] Dreyfus DH. Autoimmune disease: a role for new anti-viral therapies. Auto-immun Rev 2011;11:88–97.
[95] Sorensen PS, Ross C, Clemmesen KM, Bendtzen K, Frederiksen JL, et al. Clinicalimportance of neutralising antibodies against interferon beta in patients withrelapsing–remitting multiple sclerosis. Lancet 2003;362:1184–91.
Viviana Annibali graduated in biological sciences fromRoma Tre University of Rome (Italy) in 2001. In 2006 sheobtained her PhD in cell sciences and technologies andafter a postgraduate master degree in methodologies forresearch and development of new therapies fromSapienza University of Rome, where she recently earneda clinical pathology specialty. From 2002 she is a re-search scientist at the CENTERS, S. Andrea Hospital,Department of Neuroscience, Mental Health and Senso-ry Organs (NESMOS), Sapienza University of Rome. Dur-ing her research activities on neurodegenerativediseases she gained experience in gene expression anal-ysis at the RNA and protein level in peripheral T cell
subsets. Dr. Annibali has also gained relevant experience in studying molecularpathways and gene function via genetic and pharmacological approaches. Mostrecently, she is investigating the involvement of B cells transcriptome dysfunctionsin multiple sclerosis disease, with particular attention to the role of the cellular andextracellular microRNAs. She is a member of Italian Association of Neuroimmunol-ogy (AINI).
Rosella Mechelli received her master degree in Biologi-cal Sciences in 2000, PhD in genetic and molecularbiology in 2003 from Sapienza University of Romewhere she also earned a postgraduate master degreein methodologies for the research and development ofnew therapies in 2007. During her PhD training shestudied the structure of telomeric chromatin and itsepigenetic modifications. From 2004 she is a researchscientist at the CENTERS, S. Andrea Hospital, Depart-ment of Neuroscience, Mental Health and SensoryOrgans (NESMOS), Sapienza University of Rome. Herresearch interests lie in etiopathogenesis of multiplesclerosis in monozygotic twins discordant for the dis-
ease. Currently most of her studies are focused on the interaction between heritableand environmental risk factors, in particular on Epstein–Barr virus genetic variantsand virus–host interactions. She is a member of Italian Association of Neuroim-munology (AINI).
Silvia Romano obtained a doctor of medicine degreefrom Sapienza University of Rome in 2000 and a spe-cialization degree in Neurology at Sapienza Universityof Rome in 2006. She was also a Research Fellow atClinical and Behavioral Neurology Laboratory, S. LuciaFoundation, Rome (2008–2009, project on neurocogni-tive pattern of multiple sclerosis patients). She obtaineda PhD in Experimental Neurological Sciences in2010 and then undertook post-doctoral work at theCenter of Experimental Neurological Therapies (CEN-TERS), a Department Unit of S. Andrea Hospital,Sapienza University of Rome (2012–2013) working ondemyelinating and hereditary neurodegenerative dis-
ease. Her current position is Researcher of Neurology at Department of Neuros-ciences, Mental Health and Sensory Organs (NESMOS), at S. Andrea Hospital,Sapienza University of Rome. Her research activity is focused on (1) etiopathogen-esis, cognitive impairment and treatment of multiple sclerosis; (2) clinical featuresand treatment of patients with hereditary cerebellar ataxias and Huntingtondiseases.
Maria Chiara Buscarinu graduated in medicine andsurgery in 2006 and specialized in neurology in2012 at the University of Sassari. From 2005 to2011 she worked at the Neurological Clinic of Sassari.She moved to Rome and she began her PhD in experi-mental neurology at Sapienza University of Rome. Shecarries out ambulatory activity and research at the S.Andrea Hospital in Rome, with increased interest inmultiple sclerosis and etiopathogenetic factors relatedto the disease. She is a member of the Italian Society ofNeuroimmunology (AINI) and the Italian Society ofNeurology (SIN).
Arianna Fornasiero obtained a doctor of medicine de-gree from Sapienza University of Rome in 2004 and aSpecialization degree in Neurology at Sapienza Univer-sity of Rome in 2009. From 2010 to 2014 she wasresearch fellow in experimental neurology at SapienzaUniversity of Rome. From 2009 to today she work at theCenter of Experimental Neurological Therapies (CEN-TERS) a Department Unit of S. Andrea Hospital, SapienzaUniversity of Rome working on demyelinating disease.Her research activity is focused on etiopathogenesis andtreatment of multiple sclerosis.

V. Annibali et al. / Cytokine & Growth F228
Renato Umeton obtained his bachelor’s and master’sdegrees in computer science from University of Calabria.He earned his PhD in mathematics and informaticsfocusing his research on optimization and ontologystudies that found their application in solving problemsin the area of medicine and biology. His experienceincluded working at Microsoft and at MassachusettsInstitute of Technology, as well as collaborating withother major institutions such as the Harvard MedicalSchool and the University of Cambridge in the UK. Hecarried out his most recent Postdoc at Sapienza Univer-sity of Rome – S. Andrea Teaching Hospital, where heapplied his informatics and bioinformatics skills to un-ravel the genetic and environmental components of thepathogenesis of multiple sclerosis and other neurology-related diseases.
Vito AG Ricigliano obtained his medical degree at‘‘Sapienza’’ University of Rome, Italy, in 2013. He iscurrently a MD at Center for Experimental NeurologicalTherapies (CENTERS), S. Andrea hospital, Rome, and inthe present year he has been Academic visitor at theUniversity of Oxford, UK, Nuffield Department of Clini-cal Neurosciences (NDCN). His research investigates therole of gene–environment interactions in the etiology ofmultiple sclerosis, especially focusing on the character-ization of the interplay between EBV and the host net-works, functional interpretation of GWAS data and useof next-generation techniques (e.g. RNA-sequencing,exome sequencing).
Francesco Orzi has spent several years dedicated to labresearch, in animal models of neurological diseases, andin exploiting methods for assessment of brain functionalparameters. Following a 3 years stage (1979–1982) inthe Lab of Dr. L. Sokoloff at NIH, in Bethesda, he becamespecifically interested in mapping local cerebral func-tional changes in animal models. A few studies havecontributed to define the functional circuitry of theBasal Ganglia in relation to their role in movementdisorders and in motivated behavior. Other studies,since the early experiences in the laboratory of Dr Klatzoat NIH, have been carried out in the field of the braindamage maturation following temporary brain ische-
mia, and in the field of neuroprotection in animal models of brain ischemia. In thelast 15 years he has been fully involved in clinical neurology. Fields of interest arecerebrovascular diseases and dementias. The focus is on mechanisms that underlieneuronal degeneration associated with energy defects, dysfunction of the neuro-muscular unit, and implications for neuroprotection.
Eliana Marina Coccia is head of the Anti-InfectiousImmunity Unit at the Department of Infectious, Parasiticand Immunomediated Diseases, Istituto Superiore diSanita, Rome-Italy. She received her Ph.D. in biologicalsciences in 1984 from University of Rome, working on theeffect of type I IFN on the growth and differentiation ofFriend erythroleukemia cells. From 1984 to 1985, she wasa post-doctoral fellow at the Weizmann Institute of Sci-ence (Rehovot, Isreal) in Dr. Michel Revel’s group whereshe cloned the mouse 2-5A synthetase. In 1991–1992 shemoved at the Pasteur Institute (Paris, France) in thelaboratory of Dr. Ara Hovanessian to investigate the roleof type I IFN on HIV replication. The group lead by E.
Coccia is interested in understanding how type I IFN contribute to the induction of theimmune response against several pathogens, such as HIV, Mycobacterium tuberculosis,Aspergillus fumigatus and Epstein–Barr virus. In particular the long-term objectives ofher projects is to investigate IFN-driven immune-regulation and aberrant activationof IFN pathways in microbial infection and autoimmunity, with specific regard to Blymphocytes and primary dendritic cells.
Marco Salvetti obtained his primary medical qualifica-tion in 1986 from the Sapienza University of Romewhere he also trained as a clinical neurologist. Hewas a postdoctoral fellow at the Max Planck Societyfor Multiple Sclerosis in Prof. Hartmut Wekerle’s lab.Following studies on the fine specificity of the T cellresponse to putative autoantigens in multiple sclerosis,he instituted the world largest twin registry in1997. From then on, epidemiological, gene expressionand virological studies in twins with multiple sclerosisbegun. At present much of the studies are focused on theinteraction between heritable and environmental fac-tors in the etiology of multiple sclerosis. This informa-
tion, combined with data from the in vitro screening of off-label activities ofregistered drugs (on oligodendrocyte precursors), is exploited for the design ofexploratory clinical trials. These studies are carried out in the context of the clinicalresearch activity of CENTERS, an institution devoted to nonprofit, phase II trials inmultiple sclerosis and orphan neurological diseases.
Giovanni Ristori obtained in 1985 the degree in medi-cine, at ‘Universita Cattolica del Sacro Cuore’, Rome,Italy and in 1989 the specialization in neurology atthe same University. In 1995 he obtained a PhD inNeuroscience at Sapienza University of Rome, Italy.The present position is at Neuroimmunology laboratoryand Neurogenetic Unit, Faculty of Medicine and Psy-chology, Sapienza University of Rome, Italy.
actor Reviews 26 (2015) 221–228





























