Embed Size (px)
Citation preview

CASE PRESENTATIONDr. M. Qasim Khan,
PGR West Medical Ward,
Mayo Hospital, Lahore.

SIMPLICITY
“Simplicity is the ultimate sophistication.”
Leonardo da Vinci
“There's something really appealing about the simplicity of black-and-white images”
Joseph Gordon-Levitt
“Elegance is achieved when all that is superfluous has been discarded and the human being discovers simplicity and concentration: the simpler and more sober the posture, the more beautiful it will be.”
Paulo Coelho

Patient’s Biodata
Name: Nazir Ahmed Age: 35 YearsSex: MaleOccupation: GardenerAddress: Gullian Chak No 9, PattokiD.O.D: 4/8/14M.O.D: Emergency DepartmentEthnicity: PunjabiLanguage: Punjabi, Urdu Religion: Islam
Presenting complaintsBleeding per rectum 6monthsloose motions 2 monthsweight loss 2 monthsAbdominal Pain 20 days.fever 1 monthHistory of presenting illness:My patient normotensive and normoglycemic was in USOH 6 months back when he started noticing streaks of fresh blood along with stools . Stools were soft in consistency 1 to 2 episodes per day not associated with abdominal or per rectal pain. He took medicine (not known) from a local doctor for 1 month and noted improvement but not total resolution . Then he took medicine from a hakeem for 15 days and complained of loose stools 3-4 episodes soft to watery in consistency yellow to brown in color not associated with abdominal pain or blood. He changed the medicine from other hakeem but noted relapse of stools with fresh blood . –PTO-

For 2 months he has been complaining of loose stools initially 3 -4 episodes per day , watery in consistency dark brown in color, with mixed fresh blood and also complained of occasional watery discharge (mucus) per rectum mixed with fresh blood . He came to Lahore and diagnosed as hemorrhoids for with hemorroidectomy was done 20 days back. After that loose stools increased to 10 to 12 episodes per day associated with tenesmus and abdominal pain pain. Pain was on the lower abdomen, not radiating, increased before defecation and decreased after. He also complained of fever for 1 month remitting relapsing high grade mostly at night associated with chills that relieved on medication for 1 month. H/O anorexia and weight loss for 2 months his weight been decreased from 72 to 51 kg in 3 months . Not associated nausea, vomiting, joint pain.

Past History:A frequent history of lower leg swelling of veins for 10 years. H/O RTA 5 years back.No H/O surgery, allergies or psychiatric illness.Drug History:History of occasional use of hakeem medication since childhood. H/O azathioprine 100mg daily for 2 weeks, H/O mesalamine 2400 mg daily and sulfasalazine tabs 1500mg daily for 2 weeks. IV and oral steroids . Family History:H/O Hepatitis C in motherDiabetes in Father . Hemorrhoids in brother.

Personal History :He is married for 10 years with two children . Currently unemployed . Non smoker, No h/o TB, DM or hypertension.Socioeconomic History : He belongs to poor class . Lives in a joint family of 12 persons in a 10 Marla house .

Systemic Review General : H/O weight loss for 2 months. Anorexia for 2 months, H/O on and off fever high grade associated with chills for 1 month, H/O fatigue and inability to work for 2 months . The patient is using Diaper for 20 days.Skin: H/O Rash, redness and itching of posterior scrotal skin for 5 days. HEENT: No H/O headache or head trauma.Eyes: No H/O Eye pain redness, dryness or recent changes in vision.Ears: No H/O hearing loss, discharge, dizziness or ringing in ear.Nose: No recent H/O runny nose, stuffy nose or nose bleeds.Throat: H/O white & yellow coating of tongue & oral mucosa for 5 days that doesn’t come off on scratching. H/O Brownish-yellow patches on teeth for 10 yrs. No recent H/O sore throat or oral ulcers.

Neck: No H/O soreness, stiffness , enlarged nodes or lumps on neck.Heart: No known H/O of heart problems, hypertension, high cholesterol, chest pain, palpitations, SOB, orthopnea, PND or lower extremity edema.LUNGS: No H/O lung disease, asthma, TB or TB contact, pneumonia. NO recent H/O cough, sputum, wheezing, SOB .GI: H/O bleeding per rectum for 6 months, Loose motion for 2 months, Abdominal pain and tenderness 20 days H/O hemmorhoids for which hemorrhoidectomy was done 20 days back (Discussed in detail in HOPI). No H/O constipation, nausea, vomiting, heart burn or difficulty swallowing.

Urinary: No H/O change in frequency, burning or painful urination and other lower urinary tract symptoms.Genital: Sexually inactive for 3 months . H/O Rash, redness and itching of posterior scrotal skin for 5 days. No H/O penile sores, discharge, testicular pain or enlargement.Peripheral vascular: A frequent history of lower leg swelling of veins for 10 years that come and goes .Musculoskeletal: No H/O muscle or joint pain, cramps or stiffnessNeurologic: No H/O seizures, loss of consciousness, numbness, tingling, shooting pain or tremors

Hematological: H/O fatigue and pallor for last 4 months . H/O 3 blood transfusions in last month.Endocrine: No H/O diabetes, thyroid problems, increased thirst, urination, heat or cold intolerance.Psychiatric: H/O mild depression for last 2 months, No h/o suicidal ideation mood swings, memory problems, personality changes, nervousness or anxiety.

SummaryA 35 year old male presented with C/O fresh bleeding per rectum for 6 months, Loose stools for 2 months that increased from 3-4 to 10-12 episodes per day in last 20 days , H/O weight loss from 72 to 51 kg in last 2 months and associated anorexia, C/O high grade fever remitting and relapsing relieving on medication and mostly at night for 1 month .C/O non radiating Lower abdominal pain and tenderness and tenesmus for 1 month . H/O hemorrhoidectomy 20 days back, C/O oral thrush and jock itch for 5 days.

Differential Diagnosis:Inflammatory Bowel DiseaseIntestinal TBInfective enterocolitis (Chronic schistosomiasis, Amebiasis, Cytomegalovirus colitis, salmonellosis ETC ) Cathartic ColonIschemic colitisChronic DiverticulitisToxic megacolonNSAID enteropathyMalignancy

PHYSICAL EXAMINATION

General Survey:The patient is a normal build, young adult Indo-Aryan male who appears his stated age of 35 and is in mild distress. He is alert and oriented to person,place and time. Patient is lying down but can ambulate without difficulty and moves freely. He appears well-groomed, clean, and is dressed in a shalwarqameez. Patient talks freely and is cooperative but appears to be somewhat anxious.HR: 90/mint, BP: 130/80,RR:17/mit, Temp: 99 FPain: Mild abdominal painHeight: 5‘6“, wt: 51 kg

SKIN:Pallor +veJaundice –veCyanosis –vePalmar erythema -veSmooth Texture of skin, slightly warm, humid, normal turgor, . No apparent Skin Lesion in the exposed area from waist upwards and feet.NAILS: Clubbing –veCapillary refill 3 secondsNo Nails deformity or pathology in both hands and feet.

Head - normocephalic, no masses /lesions, cicatrices, malar flushing .Eyes - visual fields intact, PERRLA , conjunctiva palor, sclera white, anicteric, EOMI, no ptosis, Fundoscopy not done.( Normal Fundoscopy: red reflex present. discs flat w sharp margins,vessels present w/o crossing defects, retinal hemorrhages)Ears – Hearing appears Normal. Otoscopy not done (Normal otoscopy: TM's non-injected, good light reflex, no protrusion or retraction; Normal hearing tests: Webermidline, Rinne ac>bc, Whisper test 3:3)Nose - nares patent, no deformity, septal deviation or perforation.
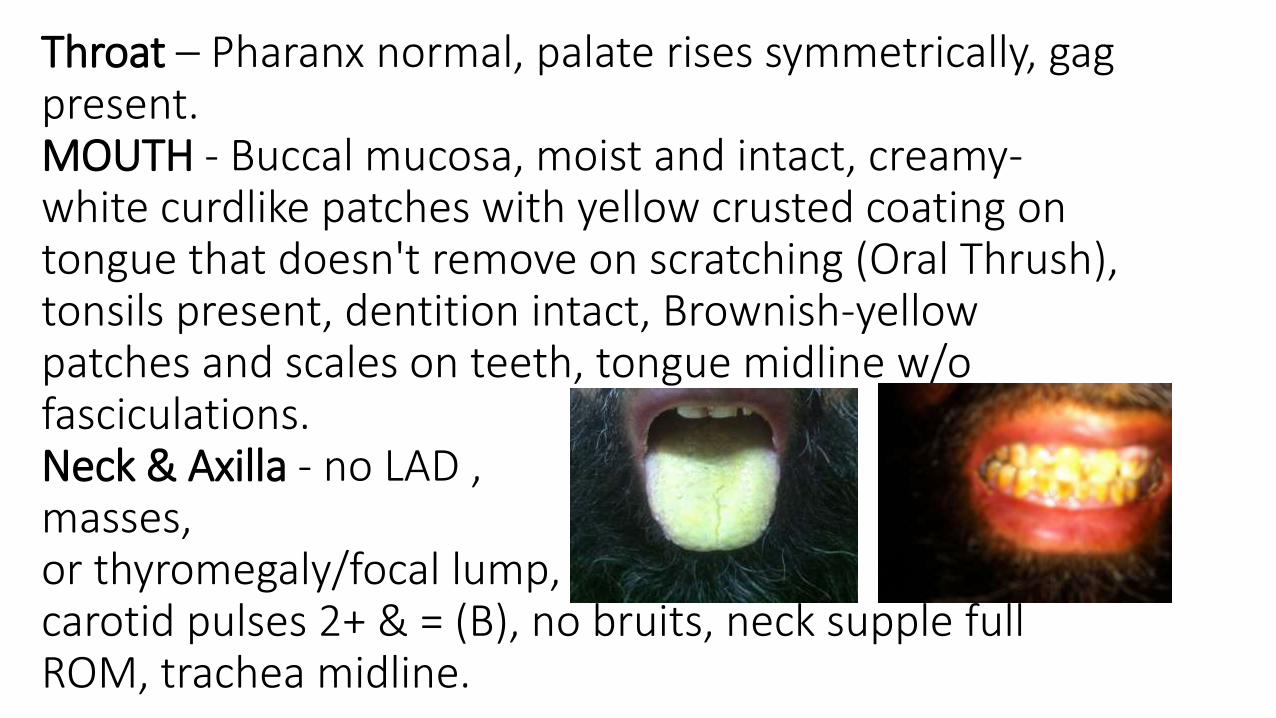
Throat – Pharanx normal, palate rises symmetrically, gag present.MOUTH - Buccal mucosa, moist and intact, creamy-white curdlike patches with yellow crusted coating on tongue that doesn't remove on scratching (Oral Thrush), tonsils present, dentition intact, Brownish-yellow patches and scales on teeth, tongue midline w/o fasciculations.Neck & Axilla - no LAD ,masses,or thyromegaly/focal lump,carotid pulses 2+ & = (B), no bruits, neck supple full ROM, trachea midline.

Back, Thorax & Lungs - Chest expansion symmetric, Clear to A&P, Normal vesicular breathing, eupnoea, no adventitioussoundsCardiovascular – JVP at 450 not raised, carotid arteries nl
upstroke & amplitude bilaterally, Inspection: no lifts or heaves, PMI not visible. Palpation: no palpable
parasternal impulses, heaves or thrills .PMI palpable in 5th ICS, MCL, nl size.Auscultation: S1- heard best at apex, nl intensity S2- heard best at base, nl splitting, A2 > P2 no m/r/g

ABDOMENObservation: Normal boat shaped abdomen, umbilicus inverted and situated centrally, no stria, scar marks.Auscultation: bowel sounds 2 cycles/min, no bruits Palpation: Superficial- tenderness in Left lower quadrant, hypogastrium and right lower quadrant, guarding –ve, no masses. Deep- Tenderness more in left lower quadrant, then hypogastrium and right lower quadrant, rebound tenderness
negative, Liver Palpation- liver edge not palpablePercussion - Size-12 cm in R midclavicular line Spleen not palpable, B/L Kidneys not palpableFemoral Pulses: 4 / 4 bil equal, no bruit

musculoskeletal - gait normal, able to tandem walk, no Rhomberg's sign; joints and muscles symmetric, noswelling, masses, deformity or tenderness to palpation; no heat or swelling of joints; full ROM; musclestrength 5/5- able to flex against resistance & w/o tenderness.genitalia/rectum - Rash, redness and itching of posterior scrotal skin and groin folds. no lesions, inflammation or discharge from penis, mucous discharge mixed with blood apparent from anus:No fistula or lesions in perianal area. PR not done. Stool dark brown watery mixed with blood, guaiac +ve .


Nervous - CN II-XII grossly intact, alert oriented, cooperative, sensory - pinprick, light touch & vibration intact; proprioception normal, motor - no atrophy, weakness, tremors or clonus; RAM, finger-to-nose/heel-to-shin intact; Rhomberg negative .DTR's - all 2+ & = (B); Babinski; toes downgoing. Naming & repetition intact; memory 3:3; (B) Pronator drift nl, gaze normal; extinguishesL side to direct sen. stim.Cranial Nerves:All cranial nerves are Intact

Summary:A 35 year old normal build, young adult Indo-Aryan male with following Vitals HR:90/mint, BP: 130/80,RR:17/mit,Temp: 99 F Pain: Mild abdominal pain.He is Pallor, has Abdominal tenderness; more in the left lower quadrant then hypogastrium and right lower quadrant. Has mucous discharge mixed with blood apparent from anus & diaper filled with dark brown watery stool mixed with blood. Has oral thrush and jock itch .

Differential Diagnosis:Inflammatory Bowel DiseaseIntestinal TBInfective enterocolitis (Chronic schistosomiasis, Amebiasis, Cytomegalovirus colitis, salmonellosis ETC ) Cathartic ColonIschemic colitisChronic DiverticulitisToxic megacolonNSAID enteropathyMalignancy

LABORATORY FINDINGS

CBC:wbc 6.2*103/ ulHb 8.2 mg/dlHCT 28.4 %MCV 92.2 fLMCH 26 pgMCHC 28.9 g/dlPLT 259 *103/ ulLymp 7.5 %Neut 90.4 %RDW 70.6 fLPDW 9.1 fL

LFT’s:Ast: 58ALT: 54Bil: 0.9T.P: 6.5Alb: 2.8RFT’S:urea: 34Creat: 1.2S/E :Na+ : 133K+ : 3.3Cl- : 97

TFT’sT3: 97 ng/dL (NR : 58-159)T4: 89 nmol/L (NR : 66-181) TSH: 1.6 mIU/L (NR : 0.27-4.2)U/E : unremarkableCxray: NormalUltrasound Abdomen : NormalStool Cytology: WBC numerous, RBC Numerous, No Ova, Cyst or Parasite seenStool Culture: No Growth of Salmonella, Shigella or vibrio species after 48 hours incubation at 370 C

PR Proctoscopy :2nd degree hemorrhoids at 3,7 and 11 ‘o Clock .There is also altered blood from higher Up.COLONOSCOPY:PR exam Blood stained. Colonoscopy seen uptosplenic flexure of Colon; Erythematous and friable mucosa with multiple ulcerations and pseudopolys. Multiple biopsies taken for histopathological exam.


Biopsy Report :Immunohistichemistry : Cytokeratin positive in epithelial cellsDiagnosis: Extensive ulcerations and inflamed granulation tissue. Focus of Large Bowel Mucosa Shows Reactive Changes.No definite Dysplasia or Malignancy Seen


Final DiagnosisSevere Ulcerative Colitis

Treatment Given in the ward:Azathioprine 50mg BDmesalamine 800 mg TDSSulfasalazine tabs 500mg TDSMesalamine Enema BDInj Hydrocortisone 250 mg TDSInj CiprofloxacinInj MetronidazoleInj Omeprazole

Further Evaluation:pANCACT AbdomenBarium Enema ….
Ehhheewww .. Take a breath !!

Discussion

Inflammatory Bowel Disease

Overview
DefinitionsHistoryEpidemiology PathophysiologyClinical featuresDiagnosis with differentialsComplicationsManagement of disease Ongoing research

IBD
Inflammatory bowel disease is an idiopathic inflammatory intestinal disease resulting from an inappropriate immune activation to host intestinal microflora.
Types of IBD are
Ulcerative colitis
Crohn’s disease
Indeterminate colitis

History
Morgagni provided a description of intestinal inflammation characteristic of Crohn's disease in 1761.
After the identification of the tubercle bacillus by Koch in 1882 it was possible to describe persons with ileocecal disease similar to intestinal tuberculosis but lacking the organism.
In 1932, the landmark publication of Crohn, Ginzburg, and Oppenheimer called attention to “terminal ileitis” as a distinct entity and chronic disease.

History
The term “Regional enteritis” embraced the focal nature of the process, but failed to incorporate knowledge of the possibility of disparate sites of involvement within the GI tract and multisystemic nature.
The term “Granulomatous enterocolitis” lost acceptance when it became clear that granulomas were not a sine qua non of the diagnosis.

History
The name “Crohn's disease” has been adopted to encompass the many clinical presentations of this pathologic entity. But for the alphabetic priority these authors chose Crohn's disease.
IT might well have been Ginzburg's or Oppenheimer's disease.

Epidemiology
The incidence of UC is 3 times higher than that of CD. But recent data suggest that the incidence of CD is increasing.
The highest rates of IBD are seen in developed countries, and the lowest in the developing regions;

Racial, sexual, and age-related differences
Highest rates are seen in the Jewish populations
The M:F ratio is approximately 1:1 for UC and females having a slightly greater incidence in CD
The age distribution of newly diagnosed IBD cases has double peak, the 1st peak in people aged 15-40 years. A 2nd smaller peak in patients aged 55-65 years

Two major types of IBD
Crohn’s disease
Incidence – 5.8 per 100,000 persons
Prevalence - 116 per 100,000 persons
Ulcerative colitis
Incidence – 7.8 per 100,000 persons
Prevalence - 156 per 100,000 persons
Minnesota study, 2009

South Asia perspective
Probert CS and colleagues found out that the minimum incidence on CD is 0.14/1lakh persons-years,
Hindus have a much lower incidence of CD than Europeans
In Pakistan, there is much less extraintestinal disease in both UC and CD than is reported from the West (where up to 25% of patients have extraintestinalmanifestations if arthralgia's are included). In Pakistan, few patients have perianal or fistulizing disease.

Etiopathogenisis
Genetic susceptibility
Environmental factors
Host immunity

Genetics
Increased risk among first-degree relatives is 14 to 15 times higher than that of the general population
Jews are at a 2-4 fold higher risk of developing IBD than non-Jews of the same geographic location
Studies in twins suggest that genetics is a more powerful determinant of disease for CD(67%) than for UC(13%).

Genetics Crohn’s disease Ulcerative colitis
anti-OmpC ab is more common among healthy family members of CD probands
3 imp. pathways in pathogenesis of CD
NOD2/CARD15
Autophagy-related genes
Interleukin (IL)-23
MDR 1
HLA-DR1
HLA-DR3,DQ2

ENVIRONMENTAL FACTORS
Rising incidence of Crohn's disease
Associated with higher socioeconomic status
Breast-feeding to be protective for IBD
Increased risk among women who use OCPs
Increased intake of refined sugars and a paucity of fresh fruits and vegetables

ENVIRONMENTAL FACTORS
UC is more common among nonsmokers than current smokers, whereas CD is more prevalent among smokers
UC is more common in current light smokers than in heavy smokers
Several infectious organisms, including mycobacteria and viruses, have been implicated in the pathogenesis of IBD

Humoral Immunity
A marked increase in the number of plasma cells
Proportional increase occurs in immunoglobulin IgG synthesis
IgG synthesis in UC is in the IgG1 and IgG3 subclasses, whereas in CD it is IgG2
Autoantibody in UC patients is pANCA, whereas in CD, Anti-CBir1, Anti-OmpCor Anti I2 antibodies are seen.

Cellular Immunity
Bacteria prompt immune responses through PRRs
Activation of the PRRs results in downstream activation of NF-κB, which then stimulates the transcription of various proinflammatory cytokines
Based on the cytokines they produce, CD4+ T cells have been divided into three major immune phenotypes:
T helper 1 – CD (IL-12)
T helper 2 - UC
T helper 17 (IL-23)

Pathology of CD
Focal intestinal inflammation is the pathologic hallmark of CD
Characterised by presence of aphthae on a background uninvolved bowel
Minute superficial ulcers, ranging from barely visible to 3 mm, and are surrounded by a halo of erythema
Coalesce into Linear or serpiginous ulcers with a stellate appearance.
Cobblestoned appearance

Crohn’s Disease

Crohn’s Disease

Intestinal inflammation in CD is a transmural process
The location of disease,
35 – 50 % - both ileum and colon.
35 % - small intestine
15- 30% - isolated colonic disease
Large ulcers, sinus tracts, and strictures, adhesion of bowel loops are late features of CD
fat wrapping - creeping of mesenteric fat onto the serosal surface of the bowel.

Microscopic findings
Granulomas are highly characteristic of CD
Prevalence of granulomas in CD
15% in endoscopic series
70% in surgical series
Pyloric metaplasia
The presence of lymphoid aggregates in the submucosa and external to the muscularis propria is a reliable sign of CD even when granulomas are not seen
TNF is the key cytokine in the formation of granulomas.

Granuloma

Ulcerative colitis
At the time of initial presentation, approximately
45% -limited to the rectosigmoid,
35% - extending beyond the sigmoid
20% of patients have pancolitis
Continuous and symmetrical involvement
Mucosa appears hyperemic, edematous, and granular in mild disease becomes hemorrhagic, with visible punctate ulcers as it progresses.

•In long-standing UC.
Epithelial regeneration with recurrent attacks results in the formation of pseudopolyps
Atrophic and featureless colonic mucosa, associated with shortening and narrowing of the colon



Microscopy
Inflammation in UC characteristically is confined to the mucosa
Neutrophilic infiltration of colonic crypts leads to cryptitis & crypt abscesses
Cryptitis is associated with discharge of mucus from goblet cells. Results in the characteristic histopathology of goblet cell mucin depletion, formation of exudates, and epithelial cell necrosis.
Crypt architectural distortion or dropout of glands.


Clinical features

Manifestations of inflammatory bowel disease
Recurrent abdominal pain and diarrhoea.
Cramping
Irregular bowel habits, passage of mucus without blood or pus
Grossly bloody stools, occasionally with tenesmus: Typical of UC, less common in CD
Growth retardation and delayed or failed sexual maturation in children
Perianal disease in 50% of patients with CD

Patients with UC
Rectal bleeding
Frequent stools- Mucous discharge from the rectum
Tenesmus (occasionally)
Lower abdominal pain and severe dehydration from purulent rectal discharge (in severe cases, especially in the elderly)

WHO- symptoms suggestive of inflamed GIT
Diarrhea: mucus or blood may be present in the stool; can occur at night; incontinence may occur.
Constipation: this may be the primary symptom in UC limited to the rectum; obstipation may occur and may proceed to bowel obstruction
Bowel movement abnormalities: pain or rectal bleeding may be present, as well as severe urgency and tenesmus
Abdominal cramping and pain: commonly present in the right lower quadrant in CD; occur periumbilically or in the left lower quadrant in moderate to severe UC
Nausea and vomiting: occurs more often in CD than in UC

Systemic symptoms
Weight loss
Fever
Sweats
Malaise
Arthralgias
A low-grade fever may be the first warning sign of a flare.

Signs
Fever
Tachycardia
Dehydration
Toxicity
Pallor, anemia
Toxic megacolon: patients appear septic, high fever with chills tachycardia & increasing abdominal tenderness & distention
Mass in the right lower abdominal quadrant: May be present in CD

Perianal disease of CD
.1Skin lesions- include maceration, superficial ulcers, abscesses, and skin tags
type 1 (elephant ears) are typically soft and painless and large
type 2 are typically edematous, hard, and tender.
.2Anal canal lesions - fissures, ulcers, and stenosis
.3Perianal fistulas.

Unusual Presentations of CD
•Gastroduodenal - H-pylori-negative peptic ulcer disease, dyspepsia or epigastricpain as the primary symptoms
•Esophageal - < 2% of patients.
•Dysphagia, odynophagia, substernal chest pain, and heartburn
•Mouth ulcers
•Esophageal stricture and esophagobronchial fistula
•acute granulommatous appendicitis -

DISEASE BEHAVIOR IN CD
Aggressive fistulizing disease
anti-OMPC
pANCA
25% of pts present with an intra-abdominal abscess
Indolent cicatrizing disease
NOD2 variants
anti-CBir1
Anti I2

Aggressive fistulizing disease
Fistulas are manifestations of the transmural nature of CD
Perianal fistulas are common and occur in 15% to 35% of patients.
Enterovaginal fistulas occur in women
Enterovesicular - recurrent polymicrobial UTI or as frank pneumaturia and fecaluria.
Enterocutaneous fistula after appendectomy
Other types- enteroenteric, enterocolonic, and colocolonic fistulas


Stricture
Stricture is another characteristic complication of long-standing inflammation
Symptoms can include colicky, postprandial abdominal pain and bloating, punctuated by more-severe episodes, and often culminating in complete
obstruction.
String sign - markedly narrowed bowel segment amid widely spaced bowel loops

CDAI
In remission <150
Mild-moderate 150-220
Moderate-severe 220-450
Fulminant >450

Ulcerative Colitis: Disease Presentation
Mild Moderate Severe
Bowel movements <4/day 4-6/day >6/day
Blood in stools Small Moderate Severe
Tachycardia None <90/min >90/min
Fever None <99.5F >99.5F
Anemia Mild Moderate Severe
ESR <30 >30
Endoscopy Erythema, decreased vascular
pattern, fine granularity
Marked erythema, coarse granularity,
absent vascular markings, contact
bleeding, no ulcerations
Spontaneous bleeding,
ulcerations

EXTRAINTESTINAL MANIFESTATIONS

Musculoskeletal
Clubbing
Arthritic manifestations
Peripheral arthropathy - 16% to 20%
Pauciarticular arthropathy (type I, affecting four or fewer joints)
Polyarticular arthropathy (type II, with five or more joints affected)
Axial arthropathies - 3% to 10%
Metabolic bone disease
Granulomatous vasculitis, periostitis and amyloidosis.

Mucocutaneous
Pyoderma gangrenosum
Erythema nodosum
Granulomatous inflammation of the skin
Aphthous ulcers of the mouth
Angular cheilitis

Pyoderma Gangrenosum

ErythemaNodosum

Ocular
Occur in 6% of patients .
Episcleritis
Scleritis
Uveitis - the posterior segment
Keratopathy and night blindness

Hepatobiliary
Gallstones
Asymptomatic and mild elevations of liver biochemical tests
PSC more often is associated with UC
autoimmune hepatitis.
Vascular
venous thromboembolism
arterial thrombosis.

Renal and Genitourinary
Inflammatory entrapment of the ureter
Uric acid and oxalate stones.
Membranous nephropathy &Glomerulonephritis
Renal amyloidosis.
. Penile and vulvar edema

DIFFERENTIAL DIAGNOSIS
Intestinal tuberculosis
Irritable bowel syndrome
Anorexia Nervosa &Bulimia
Ischemic bowel disease
Neoplasia, including carcinoma and lymphoma
Infectious diarrheas & Clostridium Difficile Colitis
Celiac Sprue
Collagenous and Lymphocytic Colitis

Abdominal pain, gastrointestinal bleeding, and/or intestinal ulceration
Ischemic colitis
Intestinal tuberculosis
Radiation-induced colitis
Arteriovenous malformations
NSAID enteropathy
Behcet disease
Colorectal malignancy

Diarrhea
AIDS
Celiac disease
Microscopic colitis
Irritable bowel syndrome
Lactose intolerance
Functional diarrhea
Gastrointestinal infections
Behcet disease
Colorectal malignancy

Investigations

Investigations
CBC
Nutritional evaluation: Vitamin B12 , iron studies, folate & other nutritional markers
ESR and CRP levels
Fecal calprotectin level
Serologic studies: pANCA, ASCA, anti-CBir1
Stool studies: Stool R/M, C/S, evaluation for Clostridium difficile toxin

Imaging studies
Upright chest and abdominal radiography
Barium double-contrast enema radiographic studies
Abdominal ultrasonography
Abdominal/pelvic computed tomography scanning/magnetic resonance imaging with enterography
Colonoscopy, with biopsies of tissue/lesions
Upper gastrointestinal endoscopy
Capsule enteroscopy/double balloon enteroscopy

Plain radiograph
In severe disease, the luminal margin of the colon becomes edematous and irregular.
Thickening of the colonic wall often is apparent on a plain film
Plain films also are useful for detecting the presence of fecal material.
The presence of marked colonic dilatation suggests fulminant colitis or toxic megacolon.


Toxic megacolon


Barium studies
Aphthous ulcers, a coarse villus mucosal pattern, and thickened folds.
Pseudo sacculation of the antimesenteric border
Cobblestone appearance
Fistulas, sinus tracts, and fixed strictures
The earliest radiologic change of UC seen is fine mucosal granularity

Crohn’s colitis

String sign

lead-pipe or stove-pipe appearance

CT Enterography
The sensitivity - 82%
specificity - 89%
accuracy - 85%.
Mural enhancement
Mesenteric fat stranding
The comb sign
Pseudosacculations

Comb sign

MR enterography
Intestinal wall thickening, submucosal edema, vasa recta engorgement, and lymphadenopathy are signs of active diseas
FIESTA images can add information regarding the functional status of fibrotic segment
MRI images yield a diagnostic accuracy of 91%.


Enteroscopy
Aphthous ulcers
Mucosal edema
Cobblestoning
Luminal narrowing
Rectal sparing is more specific before treatment has been initiated.
Skip lesions - Crohn’s does not affect the intestinal mucosa in a continuous fashion


Colonoscopy
The hallmark of UC is continuous inflammation that begins in the rectum.
The earliest endoscopic sign of UC is a mucosal erythema and edema
As disease progresses, the mucosa becomes granular and friable.
In severe inflammation, the mucosa may be covered by yellow-brown mucopurulentexudates associated with mucosal ulcerations.

Ulcerative Colitis

Uses of colonoscopy
Determine the extent and severity of colitis
Provide tissue to assist in the diagnosis.
Therapeutic use is stricture dilation

Tablet Enteroscopy
Swallows encapsulated video camera
Transmits an image to a receiver outside the pt.
It is most commonly used for finding obscure sources of GI blood loss,
The images can find ulcerations associated with CD if endoscopy and colonoscopy are unrevealing
The major risk is the potential to get lodged at the point of a stricture

Complications of CD
Perforation
Abscess formation
Stricture & small bowel obstruction
Nutritional deficiencies
Cancer: small bowel adenocarinoma
Cancer: colon???

Complications of UC
Toxic Megacolon:
Defined as a transverse or right colon with a diameter of >6 cm, with loss of haustration in patients with severe attacks of UC.
It occurs in about 5% of attacks and
It can be triggered by electrolyte abnormalities and narcotics.
About 50% of acute dilations will resolve with medical therapy alone
Urgent colectomy is required for those that do not improve

Complicatins of UC
Colon adenocarcinoma
After 8–10 years of colitis, annual or biannual surveillance colonoscopy with multiple biopsies at regular intervals should be performed
extensive mucosal involvement (pancolitis)
family history of carcinoma of the colon.
Perforation
Massive hemorrhage

IBD - Treatment
Medications used in treatment
5- ASA
Antibiotics
Glucocorticoids
Immune modulators
Biologics


5- ASA
Mainstay of therapy for mild to moderate UC and CD
Effective at inducing remission in both UC and CD( ?)
Maintains remission in UC
No role in maintenance of CD


Side effects
Sulfasalazine Anorexia, dyspepsia, nausea and vomitingHemolysis
Neutropenia-AgranulocytosisFolate deficiency
Reversible male infertilityNeuropathy
Sulfa-free 5-ASAs (mesalamine, olsalazine, balsalazide)
Headache; drug fever; rash; paradoxical disease exacerbation; pancreatitis; hepatitis;
pericarditis; pneumonitis; nephritis; secretory diarrhea (olsalazine)

Antibiotics
To treat perianal disease, fistulas, and active luminal Crohn's disease.
Beneficial in healing perianal fistulas.
Metronidazole demonstrated a prophylactic effect on endoscopic and clinical recurrence at one year
Ciprofloxacin 1 g/day to be equivalent to mesalamine 4 g/day in achieving remission of mild to moderately active CD at week 6
Combination was comparable with glucocorticoids in achieving remission over 12 weeks

Glucocorticoids
•Moderate-to-severe cases benefit from glucocorticoids.
•Oral prednisone is started at doses of 40–60 mg/d
•Parenteral glucocorticoids
•Hydrocortisone- 300mg/d
•Methylprednisolone - 40–60 mg/d
•Topically applied glucocorticoids are also beneficial for distal colitis
•Budesonide is used for 2–3 months at a dose of 9 mg/d, then tapered.(entocort)
•No role in maintenance therapy in either UC or CD.

Pearls of glucocorticoid use
Use an effective dose
Do not overdose.
Do not treat for excessively short periods.
Do not treat for excessively long periods.
Anticipate side effects.

Patients are candidates for immunomodulators or anti-TNF agents
If flares are frequent (>1-2 times),
If the duration of steroid use is prolonged
If reduction of the steroid dose causes recurrence of symptoms(steroid dependent),
If steroids do not appear to be working (steroid refractory)

AZATHIOPRINE AND 6-MERCAPTOPURINE
Purine analogs that interfere with nucleic acid metabolism
Azathioprine - 2.0 to 2.5 mg/kg/day
6-MP -1.0 to 1.5 mg/kg/day
Used in patients with IBD in whom remission is difficult to maintain with the ASA alone
Used as glucocorticoid- sparing agents in upto 2/3rds of pts
Patients who failed with antibiotics for a fistula

Selection of Pt. for Azathioprine
AGA recommends that Pts should undergo an assessment of the thiopurinemethyltransferase genotype before starting therapy with AZA or 6-MP.
Individuals who have low enzyme activity or are homozygous deficient in the TPMT mutation are at risk of very severe leukopenia, with potential septic complications, and are not be good candidates for therapy with these drugs.

how long to continue?
A randomized, controlled trial demonstrated a clinical relapse rate of 21%, 18 months after withdrawal of azathioprine in patients who had been in remission for at least 3.5 years on the drug, compared with a relapse rate of only 8% in the group who continued azathioprine.`

Side effects
Abnormal liver biochemical test results- LFT
Bone marrow suppression- CBC
Hypersensitivity reactions (fever, rash, arthralgia)
Infections
Lymphoma
Nausea, abdominal pain, diarrhea
Pancreatitis

Methotrexate
Dihydrofolate reductase inhibitor
IM or SC MTX (25 mg/week) is effective in inducing remission and reducing glucocorticoid dosage;
15 mg/week is effective in maintaining remission in active CD.
Potential toxicities include leukopenia, hepatic fibrosis and Hypersensitivity pneumonitis

CYCLOSPORINE
Lipophilic peptide with an inhibitory effects on both the cellular and humoralimmune systems.
Dose is 2–4 mg/kg per day IV, in severe UC that is refractory to IV glucocorticoid
Hypertension, gingival hyperplasia, hypertrichosis, paresthesias, tremors, headaches, and electrolyte abnormalities are common side effects.
Renal function and seizures are dose limiting side effects

BIOLOGIC THERAPIES

Anti-TNF therapy
•Infliximab, Adalimumab & certolizumab pegol
Treatment of moderate to severe active CD or UC.
Effective in CD patients with refractory perianal and enterocutaneous fistulas
If a patient does not have an initial response , currently it is considered futile to try another.

Infliximab
INDUCTION- 3 separate infusions of 5 mg/kg for moderate to severe IBD at weeks 0, 2, and 6
MAINTENANCE- infusions every 8 weeks
Before anti-TNF agents are administered, screening should be done for coexistent infection with perianal and abdominal abscess (includingMycobacteriumtuberculosis), and caution is advised if a patient is a carrier for the hepatitis B virus.

Risk factors for relapse include
male sex
leukocyte count > 6.0 × 109/L
CRP > 5.0 mg/L
Fecal calprotectin > 300 µg/g.

Side effects
The FDA reviewed 147 postmarketing reports of leukemia and 69 cases of new-onset psoriasis
Other morbidities
acute infusion reactions
severe serum sickness.
infections.
optic neuritis,
seizures,
new-onset or exacerbation of MS

Novel therapies
CDT-cell marker therapies
mesenchymal stem cells
Thalidomide
Interleukin (IL)-11
•UC -Anti-inflammatory proteins
Nicotine patch
butyrate enema
Heparin

Step up approach
Step I – Aminosalicylates -For treating flares and maintaining remission; more effective in UC than in CD
Step IA – Antibiotics:
Used sparingly in UC (limited efficacy, increased risk for antibiotic-associated pseudomembranous colitis);
In CD, most commonly used for perianal disease, fistulas, intra-abdominal inflammatory masses

Step II – Corticosteroids (intravenous, oral, topical, rectal): For acute disease flares only
Step III – Immunomodulators: Effective for steroid-sparing action in refractory disease; primary treatment for fistulas and maintenance of remission in patients intolerant of or not responsive to aminosalicylates
Step IV – : Tend to be disease-specific (ie, an agent works for CD but not for UC, or vice versa)

Management of remission
A general rule of thumb is that once remission is achieved, the medications used to achieve remission should be continued, except steroids, which should be tapered off, because they have no role in maintaining remission

Adjunctive Therapies
Antidiarrheal (diphenoxylate and atropine, loperamide, cholestyramine)
anticholinergic agents(eg, dicyclomine, hyoscyamine)
Vitamin supplementation
Iron supplementation
Smoking cessation in CD pts
Patients with active CD respond to bowel rest, along with TPN, but does not reduce inflammation in UC.
Probiotics, Prebiotics, and Synbiotics

Surgery
Indications for urgent surgery
Toxic megacolon refractory to medical management
Fulminant attack refractory to medical management
Uncontrolled colonic bleeding
Indications for elective surgery
Long-term steroid dependence
Dysplasia or adenocarcinoma found on screening biopsy
Disease present 7-10 years

Surgical intervention in IBD includes the following:
UC: Proctocolectomy with ileostomy, total proctocolectomy with ileoanalanastomosis, UC is surgically curable
Fulminant colitis: Surgical procedure of choice is subtotal colectomy with end ileostomy and creation of a Hartmann pouch
CD: Surgery (not curative) most commonly performed in cases of disease complications;

Pouchitis
Patients who undergo the IPAA procedure may develop an idiopathic inflammation termed “pouchitis,”
which typically presents with variable symptoms of increased stool frequency, rectal bleeding, abdominal cramping, rectal urgency, tenesmus, incontinence & fevers.
Patients who develop typical symptoms and signs of pouchitis after the IPAA should be treated with a short course of antibiotics (Evidence A)

Factors influencing disease relapse and remission
The use of NSAIDs and antibiotics
Bacterial and viral infections
Smoking
Psychosocial stress.
Both the severity and extent of disease are important prognostic factors after the first attack of UC.



Thank you

PG Quiz
•Extraintestinal manifestation of IBD are all except?
.1Uveitis
.2Sclerosing cholangitis
.3Osteoarthritis
.4Skin nodules

•Drugs effective in CD are all except
.15 ASA
.2Cyclosporine
.3Steroids
.4Antibiotics

•A 41 yr old male present wit recurrent episodes of bloddy diarrhea for 3 yrs, despite adequate doses of sulfasalzine. He had several exacerbations requiring
steroids to control the flares. What would be the next line of treatment
•Methotrexate
•Azathioprine
•Cyclosporine
•Cyclophosphomide

•Which of the following features is more commonly associated with ulcerative colitis than with Crohn’s disease?
•(A) Fistulas
•(B) Rectal bleeding
•(C) Segmental involvement
•(D) An abdominal mass
•(E) Mesenteric lymph node involvement

A 20-year-old woman with a family history of IBD presents with a history of intermittent right lower quadrant pain and diarrhea. Colonoscopy shows no evidence of rectal involvement but does show aphthous ulcerations in the proximal colon. Of the following serologic markers, which has a 50% likelihood to be elevated in this situation?
1.Anti-goblet cell autoantibody
2.Elevated titre against Entamoeba histolytica
3.Anti-Saccharomyces cerevisiae antibody
4.pANCA





























