Embed Size (px)
Citation preview
Iatrogenic Factors in
Periodontal Disease
Prepared by:
Lobna El Saadawy

OutlineDefinition
Common factors:
1. Margins of the restoration
2. Contour and open contact
3. Restorative material
4. Design of the removable partial denture
5. Restorative dentistry procedure
6. Malocclusion
7. Orthodontic therapy
8. Extraction of impacted third molar
9. Habits and self-inflicted injuries
10. Radiation therapy

Definition
Inadequate dental procedures that contribute to the deterioration of the periodontal tissues are referred to as iatrogenic factors

1. Margins
of the
restorationI. Overhanging restoration
II. Location of the margin
III. Marginal roughness

A) Overhanging
margins
1) Inhibit the
patient’s
access to
remove
accumulated
plaque

Overhanging
margins1) Change the ecologic
balance of the gingival
sulcus to an area that
favors the growth of
disease-associated
organisms (predominately
gram negative anaerobic
species) at the expense of
the health associated
organisms (predominately
gram-positive facultative
species)
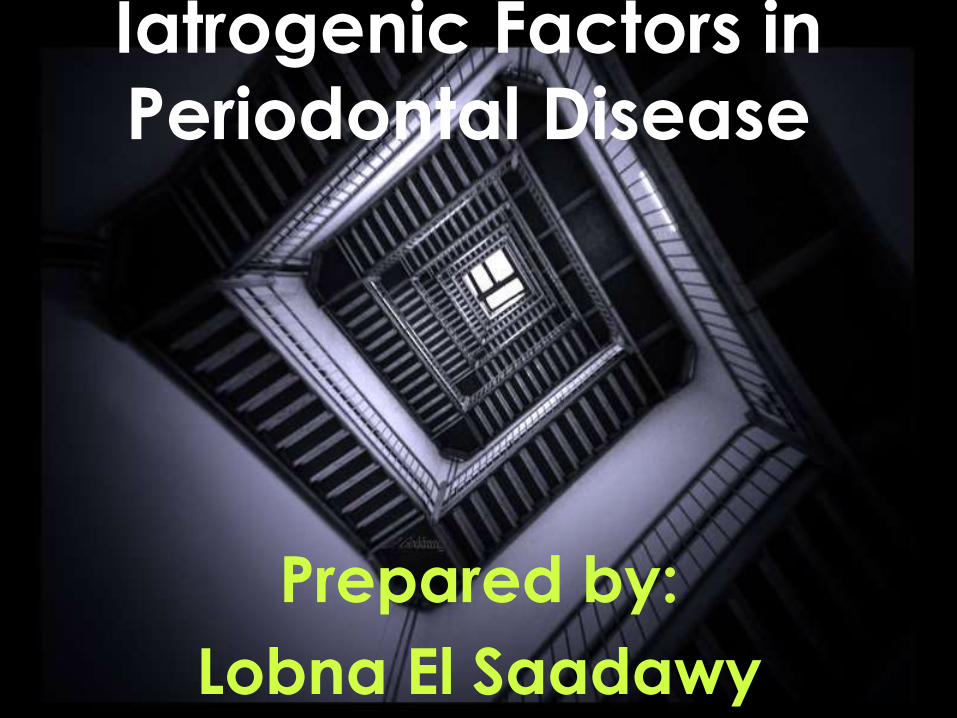
B) Location of the gingival
margin
Subgingival
margins
Equigingival
margins
Supragingiv
al margins
Severe
gingivitis
and deep
pockets
Less
severe
gingivitis
Normal as
in natural
teeth
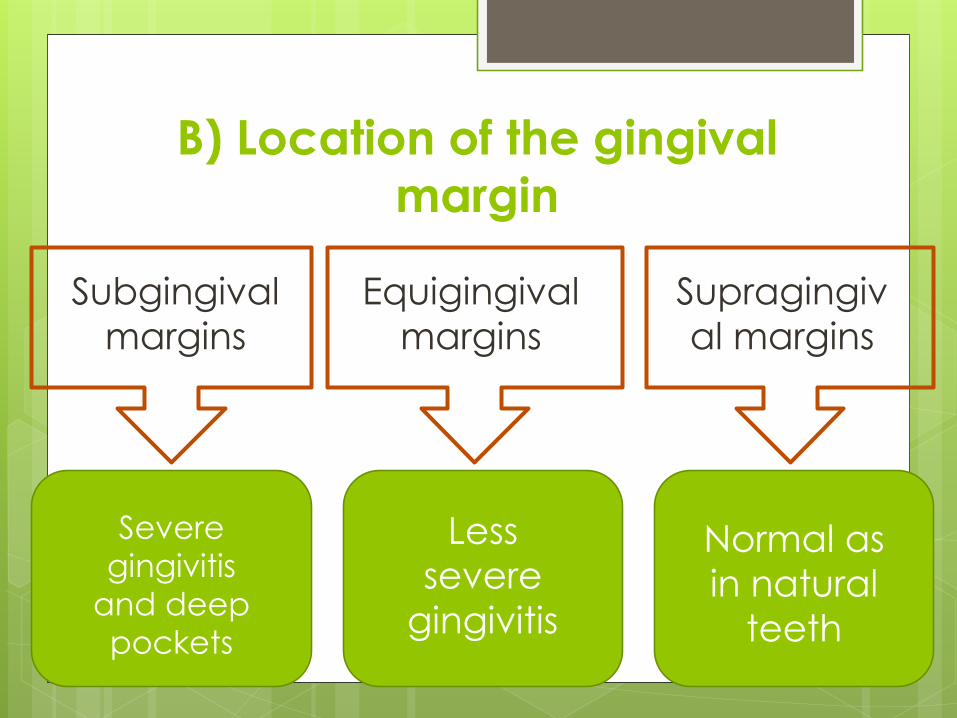
C) Marginal RoughnessSources of marginal roughness include
i. Grooves and scratches in the
surface of even
a carefully
polished
restoration ex:
porcelain or
gold restoratian

c) Marginal RoughnessSources of marginal roughness include
ii. Inadequate marginal fit of the restoration
*subgingival margins typically shows a gap of
20-40 um between the margin of the
restoration and the unprepared tooth surface
that favors bacterial plaque colonization

C) Marginal RoughnessSources of marginal roughness include:
iii. The gap that exposes the rough prepared
tooth structure following the dissolution of
the luting cement at the restoration margins
SEM photomicrograph of the
cervical margin of a 5-year old
porcelain veneer (P) showing a
small marginal defect and a border
of roughened porcelain (arrows).
(G, gingiva; C, luting composite)


2.
Contour
and
Open
Contacts
I. Overcontoured Crowns
Buccal and lingual contours
Occlusal contours
II. Inadequate interproximal embrasure

I. Overcontoured Crowns
Overcontoured crowns and restorations tend to accumulate plaqueand possibly prevent the self-cleaning mechanisms of the adjacent cheek, lips, and tongue
Overcontoured
Undercontoured
a) Buccal and Lingual
Contours
Prevent self
cleansing
mechanism of the
cheeks, lips and
tongueDoes not have that
much destructive
effect

But under contoured restorations with
absent or shallow buccal deflection ridge
are said to cause gingival trauma due to
injury by rough food


b) Occlusal Contours
Established by marginal ridges and related developmental
grooves.
Normally they deflect food away
from the inter proximal spaces

Occlusal ContoursInappropriate occlusal contours leads to
Food impaction
Plaque retention
Food impaction is defined as the forceful wedging of the food into the periodontium by occlusal forces
Cusps that tend to forcibly wedge food into interproximal embrasures are known as plunger cusps.

Occlusal Contours
Factors leading to food impaction made by Hirschfeld:
Uneven occlusal wear.
Open contact area as a result of the loss of proximal support or from extrusion
Congenital morphologic abnormalities
Improperly constructed restorations

II. Inadequate interproximal
embrasureassociated with papillary inflammation


3.
Restorative
Material

Restorative materials are not in themselves injurious to the periodontal tissues. One exception to this may be self-curing acrylics
• Plaque retention capacity of different restorative materials is different
but yet can be controlled if the restoration was well polished and was accessibile to oral hygiene measures

The undersurface
of pontics in fixed
bridges should
barely touch the
mucosa.
Access for oral
hygiene is
inhibited with
excessive pontic
to tissue contact.

4. Design of
Removable
partial
denture

Removable partial dentures favor
plaque accumulation resulting in:
gingival inflammation
periodontal pocket formation
mobility of the abutment teeth.

Partial dentures that are worn during
both night and day induce more
plaque formation than those worn
only during the daytime
The presence of removable partial
dentures induces both quantitative
and qualitative changes in dental
plaque promoting the emergence of
spirochetal microorganisms

Spirochetes are gram-negative bacteria that are
long, thin and spiral-shaped. some of them are
pathogenic to humans.
There is one species of spirochete that is part of the
natural environment of the human mouth called
Treponema denticola.
Although T. denticola is typically not harmful,but
under certain conditions , it may play a role in the
progression of periodontal disease
It is one of the red complex pathogens .

5.
Restorative
Dentistry
Procedures

The use of rubber dam clamps,
matrix bands, and burs in such a manner as to lacerate the gingiva
results in varying degrees of
mechanical trauma producing
transient injuries that generally
undergo repair
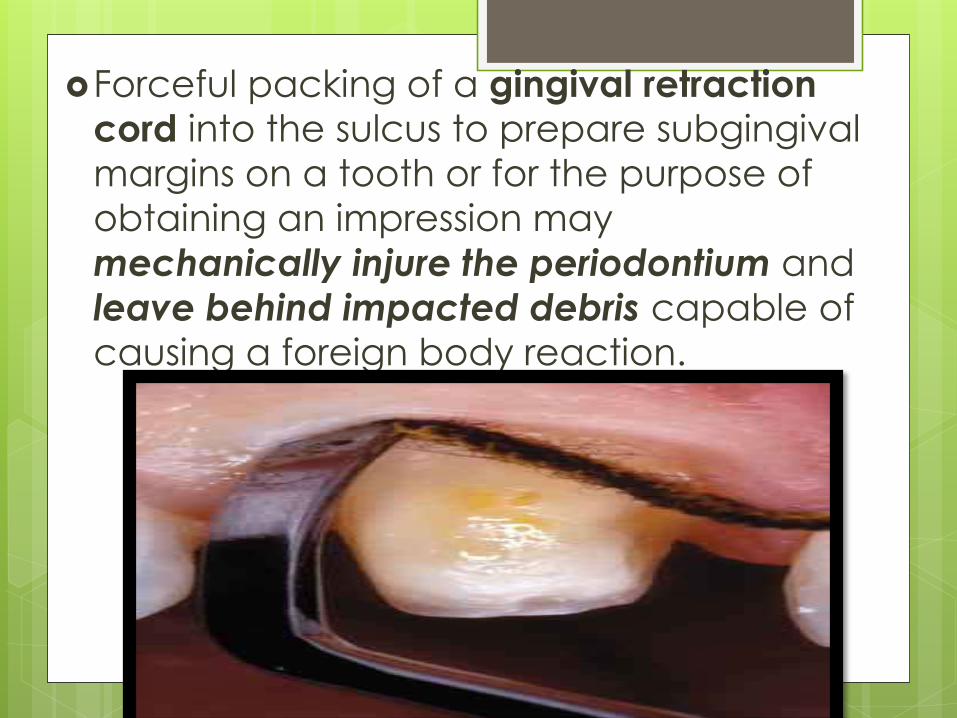
Forceful packing of a gingival retraction
cord into the sulcus to prepare subgingival
margins on a tooth or for the purpose of
obtaining an impression may
mechanically injure the periodontium and
leave behind impacted debris capable of
causing a foreign body reaction.
6. Malocclusion
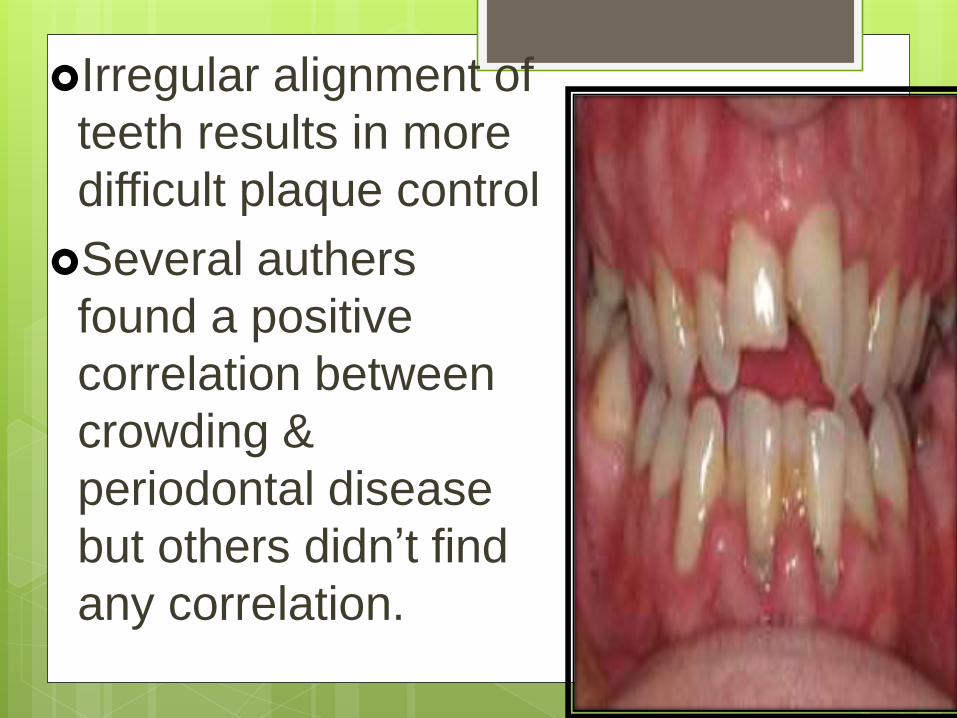
Irregular alignment of
teeth results in more
difficult plaque control
Several authers
found a positive
correlation between
crowding &
periodontal disease
but others didn’t find
any correlation.

Occlusal DisharmoniesRestorations that doesn’t conform to the
occlusal pattern of the dentition may cause injury to the supporting periodontal tissues (traumatic occlusion – T.F.O.)
Histological features of the periodontium of atooth
subjected to T.F.O. :widened PDL space,
Reduction in the number of collagen content in oblique and horizontal fibers
increase in vascularity and leukocyteinfiltration,
increase in the number of osteoclasts on bordering alveolar bone.

Failure to replace posterior teeth
After the extraction of mandibular 1st
molar with the failure to replace :
1) the initial change is a mesial drifting and tilting of the mandibular second and third molars
2) extrusion of the maxillary first molar

Failure to replace posterior teeth3) As the mandibular second molar tips
mesially, its distal cusps extrude and act as
plunger
4) The distal cusps of the mandibular second
molar wedge between the maxillary first and
second molars and open the contact by
deflecting the maxillary second molar
distally.


7. Periodontal
complications
associated
with
orthodontic
therapyI. Direct effect
II. Indirect effect

I. Indirect
Effecti. Favoring plaque
retention and food debris.

ii. Modifying the gingival
ecosystem resulting in
gingivitis
An increase in Prevotella OdontolyticusPrevotella Intermedia Actinomyces OdontolyticusAggregatibacter
actinomycetemcomitans
*With the decrease in facaulitative microorganisms

II. direct effecti. Creating excessive and/or
unfavourable forces on teeth and
supporting structures
Excessive force produce:
necrosis of PDL and adjacent alveolar bone
increase the risk of apical root resorption
Risk factors for root resorption include :
magnitude of force ,duration of treatment ,continous
versus intermittent force .
Direction of tooth movement ??????

ii. Orthodontic bands placed on
newly erupted permanents with still attached junctional epithelium on
enamel will result in apical
migration & proliferation of the junctional epithelium and an
increased incidence of gingival
recession

The mean alveolar bone loss for adolescents who under went 2 years of orthodontic treatment ranges from 0.1- 0.5 mm (this is found to be of little significance)
as that also noted for the control groups
The degree of bone loss during adultorthodontic care may be higher than that observed in adolescents,
especially if
the periodontal condition is not treated before initiating orthodontic therapy.

III. Other effects
($) Surgical exposure of impacted teeth and orthodontic-assisted eruption has the potential to compromise the periodontal attachment on adjacent teeth .
However , those teeth have more than 9o% of their attachment remains intact

($) It has been reported that the dentoalveolargingival fibers that
are located within the marginal and attached gingiva are stretched
when teeth are rotated during orthodontic therapy
Surgical removal of these gingival fibers in combination with a brief
period of retention
may reduce the incidence of relapse after orthodontic treatment intended to realign rotated teeth

8)
Extraction
of
impacted
third
molars

Extraction of impacted third molars often results in
1) the creation of vertical defects distal to the second molars
However this iatrogenic effect is unrelated to flap design
*But it’s related to presence of plaque , bleeding on probing , pathologically widened follicle , inclination of third molar , root resorption of 2nd molar
* it appears to occur more often when third
molars are extracted in individuals older than 25 years.
2) Another consequence of removal
of third molars include permanent
paresthesia (numbness of the lip,
tongue, and cheek), d.t injury of the
lingual nerve passing distal to third
mandibular molar

9. Habits
and Self
Inflicted
Injuries

I. Tooth brush trauma1. Acute
Erosions & diffuse erythema
Ulcers
Acute gingival abscess d.t.forcefully embeded tooth brush bristle
history : Signs of acute gingival
abrasion are frequently noted when the patient first uses a new brush
2. Chronic
Buccal and lingual recession and attachment loss
Cervical abrasion

II . Chemical Injury 1) allergic inflammatory states, the gingival
changes range from simple erythema to painful vesicle formation and ulceration.
E.x. mouthwashes, dentifrices, or denture
materials are often explain
2) nonspecific injurious effect of chemicals on the gingival tissues.
* topical application of
corrosive drugs such as aspirin , phenol or silver nitrate

III. Tobacco use
It results in :
1) oral leukoplakia
2) Increased incidence of gingival recession,
3) cervical root abrasion, and root caries
4) high incidence of severe periodontitis

10.
Radiation
Therapy

Radiation Therapy
Radiation therapy has cytotoxic effects on both
normal and malignant cells
The typical total dose of radiation for head and
neck tumors is in the range of 5000 to 8000
centiGrays (cGy = 1rad)
The total dose of radiation is given in partial
incremental doses (Fractionation where the typical
dose administrated is in the range of 100 to 1000
cGys per week).
this helps to minimize the adverse effects of the
radiation while maximizing the death rate of the
tumor cells.

Radiation therapy induces
Obliterative Endarteritis resulting in:
i. Soft tissue ischemia and fibrosis
ii. Hypo vascular and hypoxic bone
iii. Osteoradionecrosis
iv. Dermatitis and mucositis
v. muscle fibrosis and trismus (restricting access to oral cavity)
vi. Xerostomia (greater plaque accumulation)
vii. Caries
viii. periodontal attachment loss and teeth loss
ix. Greater risk to periodontal infections

How to prevent the
complications of radiotherapy?
1. The severity of themucositis can be reduced by asking the patient to avoid secondary sources of irritation to the mucous membrane, such as smoking, alcohol, and spicy foods.

2. Use of a chlorhexidine
digluconate mouthrinse may help reduce the mucositis. However,
chlorhexidine mouthrinses having
a high alcohol content that may
act as an astringent, which dehydrates the mucosa, thereby
intensifying the pain.
3. Fluoride application, effective oral hygiene
measures and frequent dental
examination.
4. Consult the oncologist before any surgical
or periodontal procedure to decrease
incidence of osteoradionecrosis
5. Prophylactic antibiotics to avoid
osteomyilitis
6. Restricted use of local anesthetic with vasoconstrictor.
7. Hyperbaric oxygen therapy for treatment
of osteoradionecrosis


Complications
of the Use of
Laser in
Periodontology

1. Pitting and crater formation in cementum
2. Exposure of dentinal tubules, and cementum “peeling”
3. A reduced attachment offibroblasts to Nd:YAG laser treated cementum was observed
Nd:YAG (neodymium-doped yttrium
aluminum garnet; Nd:Y3Al5O12)

In conclusion the use of the
Nd:YAG laser in periodontal
treatment is restricted to the area
of the soft tissue management. No safe removal of calculus is possible
using a Nd:YAG laser.

Erbium:YAG laser
Roughness of the enamel surface after
Er:YAG laser irradiation

After irradiation with the Er:YAG laser
enamel prisms at the rugged surface are
clearly visible, the border between lased
and non lased surface can be seen

Calculus is removed from cementum
using an Er:YAG laser, the irradiated
track is visible, the upper layer of
cementum
is removed, too
calculus
cementum
dentine