Embed Size (px)
Citation preview

1. Prolactin
2. TSH
3. FSH & LH
4. Estrogen
5. Progesterone
6. 17 OH progestrone
7. Androgens (Total testosterone, DHEAS)
ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR

It is secreted by:
Mammotropic cells of the anterior pituitary.
It is necessary for initiation & maintenance of lactation
Reference values:
Premenopuasal: <20 ng/ml
Postmenopausal: <12 ng/ml
ABOUBAKR ELNASHAR

Conditions for detection of PRL
Late morning, fasting,
After 60 min rest,
Not in late follicular phase,
2nd blood sample if the first is raised
ABOUBAKR ELNASHAR

Clinical significance:
-Hyposecretion: rare. Pituitary necrosis or infarction
-Hypersecretion:
Idiopathic, Physiologic, pharmacologic, pathologic
ABOUBAKR ELNASHAR
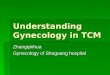
Causes of Hyperprolactinaemia
Physiologic Pharmacologic Pathologic
Pregnancy Metclorpromide Hypothalamic
disorders
Lactation Methyldopa PRL secreting
tumor
Excerise Reserpine Hpothyroidism
Eating Cimetidine Addsion’s
disease
Stress Estrogen Chest wall
disease
Morphine Ch renal failure
Alch cirrhosis ABOUBAKR ELNASHAR
Relation between The level & the cause:
> 100 ng/ml:
60% pituitary tumor.
> 300 ng/ml:
100% pituitary tumor
Modest elevation can be associated with pituitary tumor
ABOUBAKR ELNASHAR

Clinical conditions associate with
hyperprolactinaemia
1. Galactorrhea.
2. Oligomenorhea
3. Hirsutism
4. Anovulation
5. Corpus luteum deficiency
6. Infertility
ABOUBAKR ELNASHAR

Hyperprolactinaemia without galactorrhea: 66%
1. Inadequate detection
2. Hypoestrogenic state.
3. Inadequate estrogenic or progetational priming of the breast
4. High PRL does interact with the breast receptors
ABOUBAKR ELNASHAR

Diagnostic evaluation
History & Examination: Exclude: Recent pregnancy, breast stimulation
Drugs, Breast or chest lesion
Prolactin
>20 ng/ml <20 ng/ml
TSH
Normal High (hypothyroidism)
MRI or CT( Normal or hyperplasia, Microadenoma or Macroadenoma)

ABOUBAKR ELNASHAR

It is secreted by the thyrotrophic cells of the anterior
pituitary .
It stimulates the growth of the thyroid follicular cells
& every step in thyroid hormone synthesis
ABOUBAKR ELNASHAR

Reference values:
Conventional immunoassay: useful in diagnosis of
hypothyroidism.can not dd between normal values
& subnormal values in hyperthyroidism
Sensitive Immunoassay: can dd
Subclinical hypothyroidism: Increase TSH & normal
free T4
ABOUBAKR ELNASHAR

Clinical conditions associated with thyroid
dysfunction:
1. Oligomenorhea
2. Amenorrhea
3. Menorrhagia
4. Anovulation.
5. Inadequate corpus luteum.
4. Subfertility
ABOUBAKR ELNASHAR

Sensitive TSH
High Normal Low
Free T4 Normal thyroid Free T4
Low Normal Normal High
Hypothyroidism Free T3
Subclinical hypothyroidism Normal High
Subclinical hyperthyroidism Hyperthyroidism ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR

They are secreted by the anterior pituitary.
The alpha subunit is identical for all glycoprotein
hormones (TSH, HCG, LH & FSH), but the beta
subunit differs.
The peak of FSH is coincident with the peak of LH,
but it is of lesser magnitude & briefer duration.
Following the midcycle surge of LH & FSH, there is
drop in both.
ABOUBAKR ELNASHAR

Normal values:
FSH LH
Adult 5-10 mIU/ml 5-20
mIU/ml
Mid cycle peak 2 times the basal level 3 times
the basal level
ABOUBAKR ELNASHAR
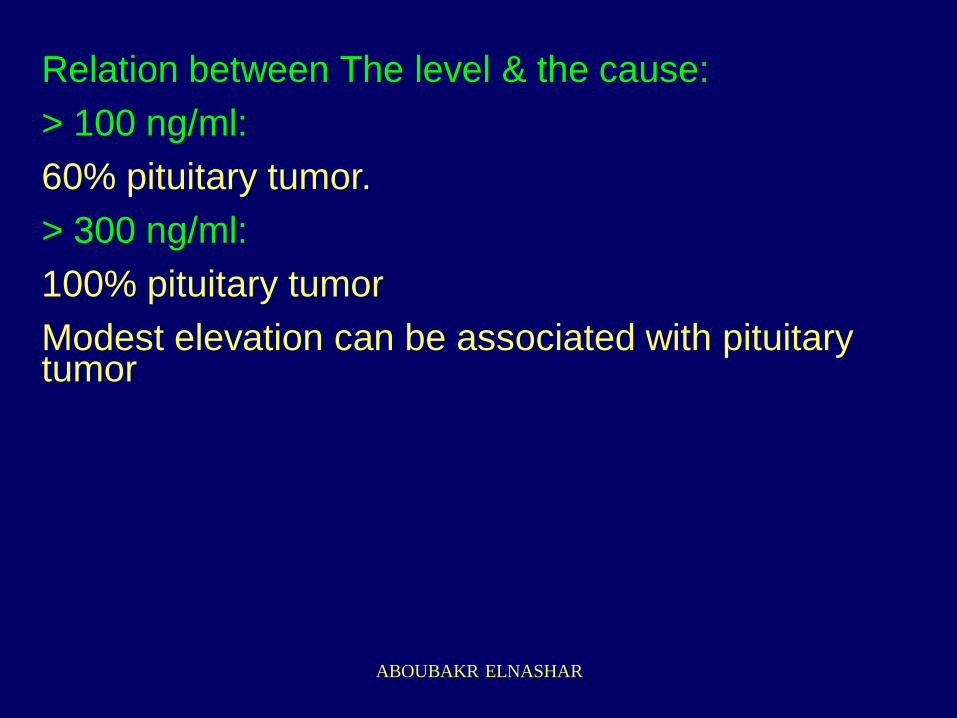
Clinical uses:
FSH LH
1. Hypogonadotrophic < 5 mIU/ml < 5 IU/ml
state e.g. prepubertal
& pituitary disorders
2. Hypergonadotropic > 40 mIU/ml >40 mIU/ml
state e.g.postmenopuse
Ovarian failure
3. PCOS normal or decreased high
Follicular phase ratio 1 2
ABOUBAKR ELNASHAR

4. Testing for ovarian function:
a. Day 3 FSH
< 10 IU/L = normal
< 15 IU/L : conception rate is twice when FSH 15-
25 IU/L
> 25 IU/L ( or age >44) is independently associated
with near zero chance of pregnancy
ABOUBAKR ELNASHAR

b.Clomiphene citrate challenge test (CCCT)
CC 100 mg /day from D5-9
Check FSH on D3 & 10
Sum of FSH >26 IU/L = poor responder
LH can be used for assessment of ovarian reserve
but FSH is better. FSH rises sooner & more
dramatically than LH.
ABOUBAKR ELNASHAR

5. Detection of ovulation
Follicular rupture occurs:
36 h after the onset of serum LH surge &
12 H after LH peak.
A positive urine result is often found only 12 h
after the onset of serum LH. (around the point
of LH peak).
So ovulation is expected to occur 24 h after
the urine LH surge
ABOUBAKR ELNASHAR
LH surge in urine:
Quick, sensitive, relatively inexpensive,
pinpoint the day of ovulation &
has reduced the uncertainty in interpretation of
progesterone levels by better-identifying the
time of peak progestrone secretion at which to
obtain serum
ABOUBAKR ELNASHAR
6. Diagnosis of the cause of precocious
puberty:
(Breast development <8 y or
menstruation <9 y.)
ABOUBAKR ELNASHAR

X ray of the lower ends of radius & ulna:bone age
a. Retarded: hypothyroidism
b. Normal: Partial
c. Advanced:
FSH: <2 IU/ml: pseudo
> 2 mIU/ml: true:
CT or MRI--------Normal: idiopathic
Abnormal: CNS lesion
ABOUBAKR ELNASHAR
7. Diagnosis of the cause of amenorrhea
Primary A.:
absence of menstruation by the age of 16 yr
regardless of SSC or by the age of 14 yr in absence
of SSC
Secondary A.:
Cessation of menstruation > 6 months
ABOUBAKR ELNASHAR

1. Pregnancy test.
2. TSH &PRL.
3. Progestin challenge test:
(MPA 5mgX2X5d)
+ve: Anovulation
ABOUBAKR ELNASHAR
-ve: E + P :
-ve: outflow or uterine failure
HSG, hysteroscopy, IVP & laparoscopy.
+ve: Ovarian failure or pituitary-hypothalamic
dysfunction.
ABOUBAKR ELNASHAR
3. FSH:
high: Ovarian failure.
If 1ry: Karyotyping.
If 2ndry: premature menopause
Low or Normal: CT of Pituitary-hypothalamic
region.
. Abnormal: pituitary disease
. Normal: hypothalamic dysfunction.
ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR
More than 30 estrogens have been identified,
but only 3 estrogens are used in clinical
practice: estrone (E!), estradiol (E2), estriol
(E3).
In contrast to E2 which is secreted almost
entirely by the ovary, most E1 is derived from
peripheral conversion of androstenedione &
from E2 metabolism.
ABOUBAKR ELNASHAR

E2 is the most abundant E in premenopausal
females
E1 is the E in highest concentration in
postmenopausal females.
E2 is the most potent E
E1, E2 & E3 are bound to SHBG.
E2 & not total E is used for clinical purposes.
ABOUBAKR ELNASHAR

Normal values of E2 (pg/ml)
Follicular phase: 25-27
Midcycle peak: 200-600
Luteal phase: 100-300
Postmenopausal: 5-25
ABOUBAKR ELNASHAR

E2 rises during the 2nd half of the follicular
phase & reach a peak 24 h before LH surge &
36 h before ovulation.
Following LH surge E2 drops to preovulatory
levels, but then rises slightly to 100-300 pg/ml
during luteal phase
ABOUBAKR ELNASHAR
Clinical applications:
1. E increases in E secreting tumors e.g.
granulosa theca cell tumors
2. To classify hypogonadism:
E is usually interpreted with gonadotropin
measurements
ABOUBAKR ELNASHAR

3. Test for ovarian reserve:
Low D3 E2 (<75 pg/ml) combined with normal
FSH: good ovarian reserve
Evaluation of both E2 & FSH is better
predictor of ovarian reserve than using either
measurement alone.
ABOUBAKR ELNASHAR
4. An indication of down regulation in the long
protocol for superovulation in ART. E2: < 50 pg/ml
5. Monitoring Superovulation in ART:
The goal is an E2 level of 200 pg/ml per large
(>14mm) follicle
The risk of OHSS is significant if E2 is >4000 pg/ml
(Sperof,2002)
The number of follicles & the type of patient should
be considered.
ABOUBAKR ELNASHAR

6. Monitoring of induction of ovulation with HMG (Sperof,2002).
E2 1000-1500 pg/ml is optimal
1500-2000 pg/ml: increase risk of OHSS
>2000 pg/ml: high risk of OHSS, consider cycle
cancellation
ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR

In the serum:
18% is bound to cortisol binding globulin
79% is bound to albumin
3% is free
ABOUBAKR ELNASHAR

Normal values (ng/ml):
P level is low prior to the mid cycle gonadotrophin
surge.
Shortly after that, P begin to rise rapidly reaching
peak levels during the middle of the luteal phase
(8days after LH peak).
Thereafter, a progressive fall occurs with barely
detectable P levels reached prior to menses.
Follicular phase: <1
Luteal phase: 5-20
Post menopause: <1
ABOUBAKR ELNASHAR

Clinical applications
1. Diagnosis of ovulation:
in cases of infertility & DUB
midluteal phase serum level of 5 ng/ml
2. Diagnosis of corpus luteal dysfunction:
Midluteal phase level of 10 ng/ml.
Sum of 3 progesterone levels from D11-4 before
menses: 15 ng/ml
ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR

It is an intermediate metabolite in steroidogenesis in
the adrenals
It is used for diagnosis of enzymatic deficiency in
the adrenals.
Increased 17 OH progesterone indicates congenital
adrenal hyperplasia
Clinical application
1. Hirsutism
2. Ambigous genitalia
ABOUBAKR ELNASHAR

17 oh P(ng/dl) morning
< 200 > 200
Rules out adrenal hyperplasia ACTH stimulation test (0.25
21-hydroxylase defiency mg ACTH I.V.& 17 oh P at time
zero & after 1 hour)
Normal Abnormal
Rules out adrenal hyperplasia Adrenal hyperplasia
ABOUBAKR ELNASHAR
ABOUBAKR ELNASHAR

Androgen production Androstenedione
Testosterone
Adrenal DHEA Ovary
DHEAS
50% 50% 50%
25% 25%
90% 10%
100%
ABOUBAKR ELNASHAR
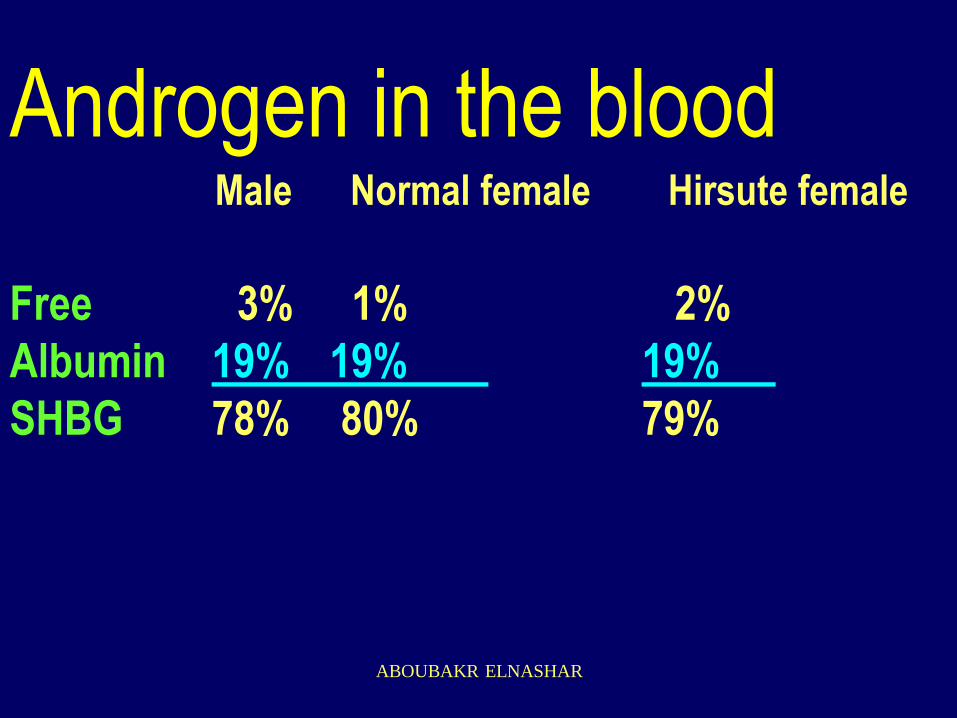
Androgen in the blood Male Normal female Hirsute female
Free 3% 1% 2%
Albumin 19% 19% 19%
SHBG 78% 80% 79%
ABOUBAKR ELNASHAR
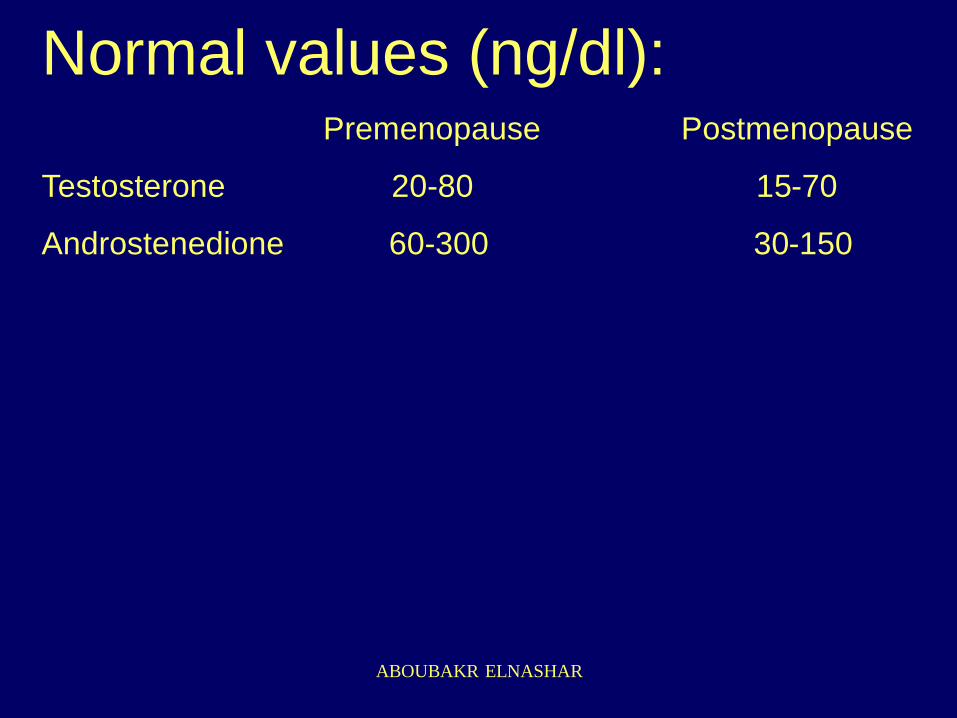
Normal values (ng/dl): Premenopause Postmenopause
Testosterone 20-80 15-70
Androstenedione 60-300 30-150
ABOUBAKR ELNASHAR

Free testosterone
Good correlation with total production rate (= secretion
rate + peripheral conversion rate) which correlate well
with degree of virilization
Normal level: 1.5-11.4 pg/ml
Not done routinely in presence of hirsutism
•Free androgen index (FAI)=
TX 100 / SHBG if > 4.5 : PCOS
ABOUBAKR ELNASHAR

•Dehydoepiandrosterone sulphate
(DHEAS)
The principal contribution of 17 ketosteroids
(KS) is from DHES.
It correlates with urinary 17 KS. It is more
reliable indicator of adrenal androgen than 24
h 17 KS.
ABOUBAKR ELNASHAR

Clinical application
In PCOS: DHEAS > 2ug/ml
CC + Corticosteroid (ACOG,2002)
In hirsutism: DHEAS: >2 ug/ml
COCs + Corticosteroids
DHEAS: not essential
(Sperof,2002)
ABOUBAKR ELNASHAR

DHES is not essential (Speroff,2002)
1. If 17 OHP is normal: adrenal enzyme defect can
be excluded .
2. Moderate elevations of DHES can be suppressed
by suppression of ovulation.
3. DHES > 700 ug/dl is rare & is associated with high
levels of testosterone
4. Imaging of the adrenals is more cost-effective than
measuring DHES.
N.B:Hyperprolactinaemia can cause an increase in
DHEAS. Treatment with Bromocriptin will decrease
prolactin & DHEAS ABOUBAKR ELNASHAR
Total teststerone
Clinical application:
1. Initial laboratory investigation of hirsutism
Total testosterone: measures the ovarian & adrenal
activity.
ABOUBAKR ELNASHAR

Testosterone (ng/dl)
>200 <200
U/S of the ovary Anovulation
( FG/I. PRL, endom biopsy)
Adenxal mass Nothing
Laparotomy CT of the adrenala & ovaries
Laparotomy ABOUBAKR ELNASHAR

2. Evaluation of infant with ambiguous
genitalia
ABOUBAKR ELNASHAR
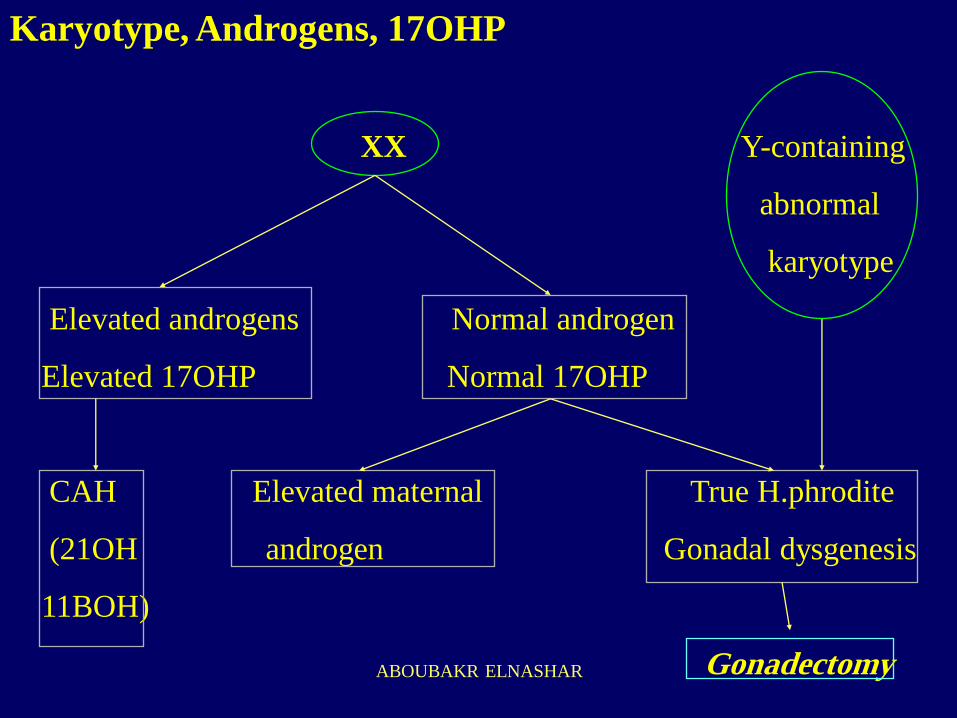
Karyotype, Androgens, 17OHP
XX Y-containing
abnormal
karyotype
Elevated androgens Normal androgen
Elevated 17OHP Normal 17OHP
CAH Elevated maternal True H.phrodite
(21OH androgen Gonadal dysgenesis
11BOH)
Gonadectomy ABOUBAKR ELNASHAR

Karyotype, Androgens, 17 OHP
XY
Normal androgens Normal androgens
signs of adrenal failure Normal 17OHP
normal 17 OHP
CAH with 3B IAIS, 5reductase def, true hph,
. Dehydogenase mixed gonadal dysgenesis,
block in male. abnormal androgen synthesis
Gonadectomy ABOUBAKR ELNASHAR

ABOUBAKR ELNASHAR