Embed Size (px)
Citation preview

HISTORY AND PHYSICAL
EXAMINATION OF CVS
Dr. Md. Mostafizur Rahman BhuiyanMedical officer, Paediatric Cardiology
Bangabndhu Sheikh Mujib Medical University (BSMMU)

Congenital heart disease is the single most common major congenital anomaly, responsible for 3-5% of death during 1st week of life and up to 33% of death during the entire neonatal period.Despite major advance in noninvasive diagnosis the history and physical examination remain important in –
1) Detection of heart disease in infant and children
2) Evaluation of severity

IDENTIFICATION OF FUNCTIONALLY IMPORTANT HEART DISEASE IN INFANT AND CHILDREN:
Symptoms associated with congenital heart disease in small infant include
1)Cyanosis2)Tachypnea3)Laboured breathing4)Feeding difficulties5)Failure to gain weight adequately6)Sweating7)Irritability or lethargy
In childhood –
1)Pt may complaints of –2)Shortness of breath with exercise3)Fatigue4)Dizziness5)Palpitation

IDENTIFICATION OF FUNCTIONALLY IMPORTANT HEART DISEASE IN INFANT AND CHILDREN:Cyanosis - It is a blue discoloration of skin, mucous membrane caused by
deoxygenated blood (4-6 gm/dl) within capillary network. ▪ Sp02 – 75-85%▪ Pa02- 32-42 mmHg in neonate for fetal Hb▪ 42-54 mmHg in older infant as Fetal Hb is declining with age
Central cyanosis: is physiologic up to 20 minutes after birth, but after that it implies to cardiac or pulmonary disease.
Differential cyanosis – cyanosis is more prominent either in upper or lower extremities. SpO2 difference between extremities is 10-20% Example –1) PDA – cyanosis is more in lower extremities (upper half of body receive blood from Lt ventricle &
lower half from Rt ventricle), Pulmonary hypertension 2) Large VSD with mixing at ventricle level –difference in O2 saturation between brachial and femoral
artery may be measurable only by O2 analysis3) TGA with pulmonary hypertension with large PDA

Acrocyanosis: Physiologic prominence of diffuse vein around eye, nose or lips
It reflect intermittent vasomotor change in the skin Pathologic cause cutaneous arterial constriction due to low
cardiac output, to conserve blood flow for protection of vital organs
Cutis marmorata: Purple marble like mottling of the skin that appears on exposure
to cold in children Cutaneous small arterial constriction leaving visisble small
cutaneous blue venules
IDENTIFICATION OF FUNCTIONALLY IMPORTANT HEART DISEASE IN INFANT AND CHILDREN:
CYANOSIS (CONTINUED)

PAROXYSMAL HYPOXEMIC SPELL: in cyanotic attack Infants breathe quickly with audible and visible distress, characterized by –
1) ↓SpO22) ↓BP3) Pallor is more prominent than cyanosis
Cyanotic spell – Occur more frequently in the morning and after a feeding in early infancy or develop at 6-12 month, there is spontaneous improvement in 18 m –
2 yr It usually resolves spontaneously after 1-5 min but may last for 20-30 min
Spell may occur in –1) PS or atresia with an intracardiac communication2) TOF (most common)3) Tricuspid atresia4) TGA5) At rest In infant with mild to moderate arterial desaturation (Pink Tet)6) Cyanotic child with iron deficiency
IDENTIFICATION OF FUNCTIONALLY IMPORTANT HEART DISEASE IN INFANT AND CHILDREN:

1) Initial ↓ systemic arterial resistance2) ↑ Rt to left ventricular shunt blood flow3) ↓ arterial O2 saturation to critically low level4) ↓↓ systemic vascular resistance &
progression of Hypoxemia5) Metabolic acidosis6) Respiratory center is stimulated (↓Pao2,
↓Ph)7) Hypercapnia8) Infant becomes restless and agitated9) Cyanosis increases10)Rarely clonic seizure may occur
IDENTIFICATION OF FUNCTIONALLY IMPORTANT HEART DISEASE IN INFANT AND CHILDREN:
PAROXYSMAL HYPOXEMIC SPELL (CONTINUED): Sequence of events:

SQUATTING its is a protective response to extreme hypoxemia in
children with an intracardiac Rt-Lt shunt Children with TOF who can walk may squat to rest
after exertion Infant who cant walk may pull up the legs to the
chest when tired Squatting increases systemic vascular resistance and
systemic blood pressure, which reduces the Rt-Lt shunt & improves pulmonary blood flow. The transient increase in BP stimulates the baroreceptors and the heart rate slows via the Vagus nerve
IDENTIFICATION OF FUNCTIONALLY IMPORTANT HEART DISEASE IN INFANT AND CHILDREN:

CONGESTIVE HEART FAILUREHeart failure occurs in 30% of infants and children with congenital heart defects, among these 90% occurs during the 1st year of life Earliest manifestation of congestive failure in infant is change
in the pattern of respiration – Tachypnea Labored respiration or dyspnea with grunting and intercostal retraction
In infant with congestive heart failure Tachypnea is a reflex response to an increase in pulmonary venous pressure or volume – Increase in pulmonary blood flow ▪ Large lt to rt shunt▪ Anatomical obstruction to return of pulmonary venous blood flow to lt heart
It may result from the increased hemodynamic resistance to left ventricular filling because of lt ventricular failure and raised lt ventricular end diastolic pressure
IDENTIFICATION OF FUNCTIONALLY IMPORTANT HEART DISEASE IN INFANT AND CHILDREN:

Tachypnea
Respiratory rate: upper limitBirth to 6
week6 week – 2
yr2-6 yr 10.yr > 10 yr
45-60/m 40/m 30/m 25/m 20/m
Tachypnea is rapid shallow respiration with a persistently fast rate of 60 breaths or more per minute in the fasting quiet newborn infant
After feeding or crying hard the healthy infant may transiently have a RR of 80-100/m
Modest elevation of pulmonary venous pressure to 8-10 in infant may be associated with tachypnea
IDENTIFICATION OF FUNCTIONALLY IMPORTANT HEART DISEASE IN INFANT AND CHILDREN:
IDENTIFICATION OF FUNCTIONALLY IMPORTANT HEART DISEASE IN INFANT AND CHILDREN:

IDENTIFICATION OF FUNCTIONALLY IMPORTANT HEART DISEASE IN INFANT AND CHILDREN: Dyspnea Feeding difficulty and failure to
thrive Sweating and pallor Exercise tolerance Sudden death Arrhythmias Chest pain

MEDICAL HISTORY
History of – Important illness –
Diabetes mallitus SLE
Medications – Exposure to potentially cardiotoxic drugs Alcohol
Exposure to Radiation Fever with Rash Rheumatic fever Still birth Spontaneous abortion

HISTORY OF IMMUNIZATIONS Except for the critically ill infant with
heart disease immunization should not be delayed, because Pertussis and Rubeola are especially dangerous for such patients.

DEVELOPMENT AND THE CENTRAL NERVOUS SYSTEM Majority of children with congenital heart disease
display normal development, a few have coexisting intellectual, perceptual or motor handicaps
Stroke – Neurologic complication may occur in association with
cyanotic heart disease Most common in children under 2 yrs of age Most likely accompanies –▪ Iron deficiency▪ SaO2 < 50%
Headache – Polycythemia due to intravascular plethora Persistent severe headache in a child with coarctation of the
aorta may rarely occur due to cerebral arterial aneurysm

History of the pregnancy, especially the first 3 months
Viral infection Rubella PDA, PBS, VSD CMV Coxsackie virus acute myocarditis
Drug exposure Teratogenic drug Sex hormones Alcohol fetal alcohol syndrome (VSD, ASD)
Maternal disease – Diabetes (VSD, TGA, Cardiomyopathy) SLE (Complete AV block)
2% of congenital heart disease is environmental in origin

Family historyFamily history of – Congenital heart disease –
Offspring has 10-15% risk if mother has congenital heart disease If an older sibling is affected risk of recurrence is 1-5% If there are 2 first degree relatives affected risk is tripled Risk of recurrence is higher with more common defects
Syndromes in parents and their immediate relatives about 8% of congenital heart defects have a genetic or chromosomal basis dominant inheritance▪ Marfan syndrome▪ Holt-Oram syndrome
Recessive inheritance▪ Friedreich’s ataxia▪ Cutis laxa▪ Pseudoxanthoma elasticum
Stillbirths Spontaneous abortion

Birth historyHistory of – Progress of labor Method of delivery Apgar score Asphyxia during labor or delivery may be associated with persistence
of fetal circulation, this may be manifested clinically as – Transient tachypnea Very cyanotic infant Persistent pulmonary hypertension Transient myocardial ischemia Myocardial dysfunction Congestive cardiac failure
Delay in clamping the umbilical cord or fetal-to-fetal transfusion in the case of twin may give rise to – Polycythemia Volume overload Congestive cardiac failure

Birth weight Congenital heart disease has a low birth wt
distribution Infants of low birth weight have a poorer survival
rate than infants of normal birth wt with heart defects
The premature infant has an increased incidence of – PDA Ventricular septal defect
Baby with large for gestational age (baby of diabetic mother) has a 3/4 times risk of congenital heart disease

Sex
Common in boys Common in girls •Coarctation of the aorta•Aortic valve stenosis•Transposition of the great arteries
•Atrial septal defect•Patent ductus arteriosus

IDENTIFICATION OF FUNCTIONALLY IMPORTANT HEART DISEASE IN INFANT AND CHILDREN: Review of other systems – is very important as
Extracardiac malformation was detected in about 25% of pt with congenital heart disease Syndrome identification – Down syndrome – ▪ 4% of infants with congenital heart disease▪ 40% have congenital heart disease, among them 40% have an ▪ endocardial cushion defect▪ Atrioventricular septal defect
Skeletal abnormalities – 32.5% of the anomalies has association with congenital heart disease VATER (vertebral defect, anal atresia, tracheo-oesophageal fistula, esophageal atresia,
radial and renal anomalies) VACTERL (anomalies of vartebrae, anus, cardiovascular tree, trachea, esophagus, renal
system, limb buds) Klippel –Feil syndrome – congenital heart disease+cervical vertebral fusion
Scoliosis – is associated with In most instances is idiopathic 15% have associated vertebral anomalies 2% of acyanotic congenital heart disease 6% of cyanotic disease

IDENTIFICATION OF FUNCTIONALLY IMPORTANT HEART DISEASE IN INFANT AND CHILDREN:
Pyrexia
A presenting complaint or history of an inflammatory illness in the pt with cardiac findings following disease should be suspected – Kawasaki’s disease if age is < 2 yr Rheumatic fever Myocarditis Endocarditis – the following history should be taken ▪ State of dental health▪ Dental therapy▪ Any other operative procedure
A history of headache, vomiting and undue somnolence with fever in the cyanotic child suggest brain abscess

IDENTIFICATION OF FUNCTIONALLY IMPORTANT HEART DISEASE IN INFANT AND CHILDREN: Straight-Back syndrome Palmar creases Polydactyly Thumb abnormalities with or without
anomalies of the radius Archnodactyly Gastrointestinal tract Genitourinary anomalies

PHYSICAL EXAMINATION:
Clubbing Pulse Pulse volume Pulsus paradoxus Pulsus alternans Pulsus bisferiens

BLOOD PRESSURE – Clinical methods of recording blood pressure –1) Palpation2) Auscultation3) Ultrasound Doppler 4) Oscillometric method5) Flush technique
PHYSICAL EXAMINATION:

Jugular venous pressuresEdemaHepatomegalyPulmonary congestion
PHYSICAL EXAMINATION:

EXAMINATION OF THE HEART:THE APEX BEAT

EXAMINATION OF THE HEART:THE APEX BEAT
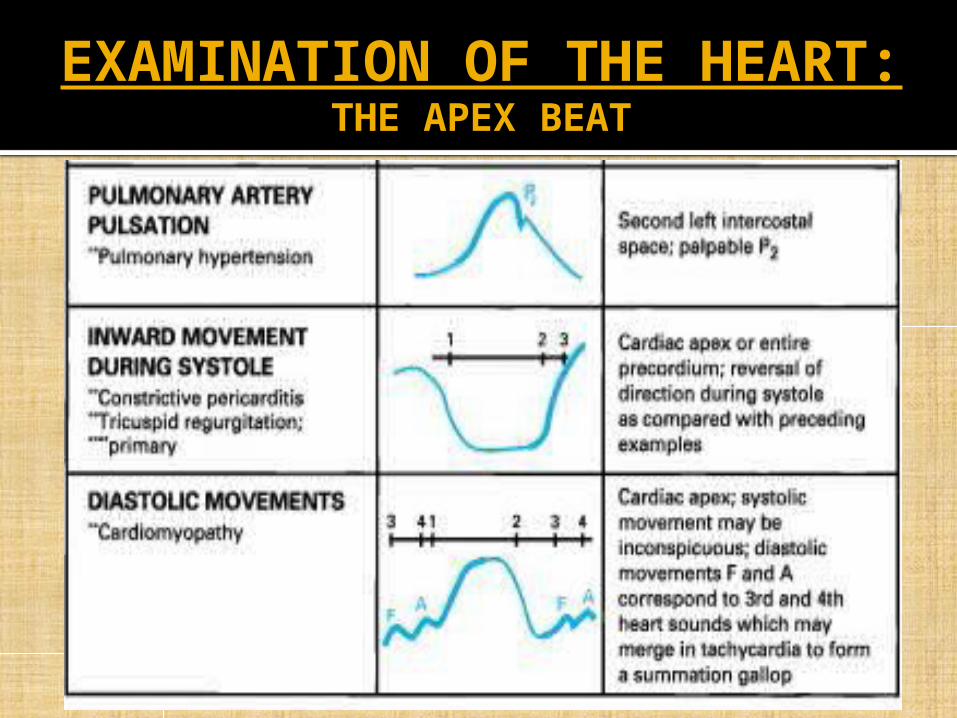
EXAMINATION OF THE HEART:THE APEX BEAT

Palpation Thrill Palpation of heart sounds Percussion Auscultation of the heart
EXAMINATION OF THE HEART:

EXAMINATION OF THE HEART: Conditions for auscultation Second heart sound Third heart sound Fourth heart sound Ejection sounds Mid systolic click and mitral leaflet
prolapse Click associated with an aneurysm of
the ventricular septum Murmur

EXAMINATION OF THE HEART:Components of auscultation of the
cardiovascular system1) Stethoscope – Use in each site
a) Bell b) Diaphragm c) Short tubing (16-18 in.)d) Use familiar (personal) and
comfortable instrument
2) Auditory conditions – Insist on quiet
a) Patient b) Parentsc) Attendantsd) Examining roome) Adjacent areas
3) Areas to examine routinely a) Primary aortic (2nd intercostal space, rt sternal edge)b) Pulmonary (2nd i.c space, lt sternal edge)c) Tricuspid (4th i.c space, lt sternal edge)d) Mitral /apex (5th i.c space, midclavicular line or at apex if displaced)e) Rt and lt infraclavicular areaf) Rt and lt axillaeg) Rt and lt interscapular areas (especially if pulmonary or aortic collaterals are suspected)h) Rt andlt carotids (especially if thrill present)i) Cranium (rt and lt temporal areas) (especially in newborn with heart failure)j) Rt and lt lumbar region (especially if high blood pressure)k) Abdominal aorta (especially if abdominal coarctation or aneurysm suspected)l) Rt and lt femoral arteries (especially if evaluating wide pulse pressure)

EXAMINATION OF THE HEART:Components of auscultation of the
cardiovascular system
4) Patient position – Examine each valve area with patient in –a) Supineb) Sittingc) Standing (brings out click of mitral leaflet prolapse)d) Squatting (to reduce murmur of aortic stenosis with hypertrophic
cardiomyopathy and exaggerating or eliciting murmur of mitral regurgitation)
5) Effect of respiration during basal conditionse) Quiet, deep, unforced, continuous respiratory excursionf) Deep-held inspiration, the expiration
6) Effect of varying cardiac outputg) Basal (or quiet, resting) stateh) During increased cardiac output (exaggerates most murmurs nad
elicits somei) After exerciseii)After a large feeding in an infant

EXAMINATION OF THE HEART:HEART SOUNDS
Sound Variation Example
S1 Decreased Depressed ventricular contractility, e.g. myocarditis, prolonged PR interval
S1 Increased Increased cardiac output, e.g., exercise, fever, excitement, mitral stenosis, short PR interval
S2 Single, increased Transposition, tetralogy of fallot, pulmonary hypertension, truncus arteriosis
S1 & S2 Decreased Decreased ventricular ejection rate and volume (low cardiac output) e.g. myocarditis, large pericardial effusion
S2 Splitting, wide, usually ‘’fixed’’
Atrial septal defect, right bundle branch block
S2 Splitting, wide, moves with respiration
Pulmonary stenosis, ventricular septal defect or patent ductus arteriosus with large shunt, idiopathic dilatation of pulmonary artery
S2 Splitting, reversed Wolff Parkinson white syndrome type B, LBBB, severe AS

WIDE PHYSIOLOGIC SPLITTING OF THE SECOND HEART SOUND:
1) Delayed pulmonic closure a) Delayed electrical activation of the right ventricle
i) Complete RBBB (proximal type)ii) Left ventricular paced beatsiii)Left ventricular ectopic beats
b) Prolonged right ventricular mechanical systolei) Acute massive pulmonary embolusii) Pulmonary hypertension with right heart failureiii)Pulmonary stenosis with intact septum (moderate to severe)
c) Decreased impedance of the pulmonary vascular bed (increased hangout)i) Normotensive atrial septal defectii) Idiopathic dilation of the pulmonar arteryiii)Pulmonic stenosis (mild)iv)Atrial septal defect, post operative (70%)v) Unexplained AES (audible expiratory splitting) in normal subjects
2) Early aortic closurea) Shortened LVET (lt ventricular ejection time)
i) Mitral regurgitationii) Ventricular septal defect

REVERSED SPLITTING OF THE SECOND HEART SOUND:
1) Delayed aortic closurea) Delayed electrical activation of the left ventricle
i) Complete LBBB (proximal type)ii) Right ventricular paced beatsiii)Right ventricular ectopic beats
b) Prolonged left ventricular mechanical systolei) Complete LBBB (peripheral type)ii) Left ventricular outflow tract obstructioniii)Hypertensive cardiovascular diseaseiv)Arteriosclerotic heart disease
(1)Chronic ischaemic heart disease(2)Angina pectoris
c) Decreased impedance of the systemic vascular bed (increased hangout)i) Poststenotic dilation of the aorta secondary to aortic stenosis or regurgitationii) Patent ductus arteriosus
2) Early pulmonary closure3) Early electrical activation of the right ventricle4) Wolf parkinson white syndrome, type B

Hemodynamic determinants of the S3: Ability of the ventricle to accept flow during the rapid
phase of diastolic filling Rate of relaxation of the ventricle End-systolic or residual volume of the ventricle Compliance of the relaxed ventricle Non obstructed atrioventricular valve
Atrial pressure head Atrial blood volume Atrial compliance
Dynamic impact of the heart with the chest wall Architecture of the thorax Cardiac size Cardiac motion within the thorax Phase of respiration Position of he patient

OPENING SNAPS:EARLY DIASTOLIC SOUNDS:1. Opening snaps2. S33. Pulmonary component of a widely split S24. Pericardial knock OPENING SNAPS: Opening of normal AV valve is almost always a silent event Generated at early diastole, (due to thickening and deformity of the
valve leaflets) following A2 Is a crisp, sharp sound heard in the mid precordial location, usually
best in the area from the left sternal border to just inside the apex, often at the base of the heart
There is no variation in the intensity or timing of the mitral opening snap with respiration
Heard in –1. MS2. High flow across AV valves large ASD

PHYSIOLOGIC CLASSIFICATION OF CONTINUOUS MURMUR:
1) Continuous murmurs caused by rapid blood flowa) Venous humb) Mammary soufflec) Hemangiomad) Hyperthyroidisme) Acute alcoholic hepatitisf) Hypermia of neoplasm (hepatoma, renal cell carcinoma, paget
disease)2) Continuous murmurs caused by high to low pressure shunts
a) Systemic artery to pulmonary artery i) Patent ductus arteriosusii)Aortopulmonary window,iii)Truncus arteriosusiv)Pulmonary atresiav)Anomalous left coronaryvi)Bronchiectasisvii)Sequestration of the lung

PHYSIOLOGIC CLASSIFICATION OF CONTINUOUS MURMUR:
b) Systemic artery to right heart a) Ruptured sinus of Valsalvab) Coronary artery fistula
c) Lt to Rt atrial shunting c) Lutembacher syndromed) Mitral atresia plus ASD
d) Venovenous shuntse) Anomalous pulmonary veinsf) Porto-systemic shunts
e) Arteriovenous fistula (systemic or pulmonic)3) Continuous murmurs secondary to localized arterial obstruction
a) Coarctation of the aortab) Branch pulmonary stenosisc) Carotid occlusiond) Celiac mesenteric occlusione) Renal occlusionf) Femoral occlusiong) Coronary occlusion

EXAMINATION OF THE HEART:
Description of a murmur:Intensity Grades I barely audible
Grades II medium intensityGrades III loud but no thrillGrades IV loud with a thrillGrades V very loud but still requiring positioning of
the stethoscope at least partly on the chest
Grades VI so loud that the murmur can be heard with the stethoscope off the chest
Phase Systole, diastole, continuous

Shape Crescendo Crescendo murmurs progressively increase in intensity
Decrescendo • Starts out at a high intensity and decreases in intensity• The turbulence begins with S2 and declines as the ventricle fills and the pressure difference between the artery and the ventricle decreases• Characteristic of early diastolic murmurs of aortic and pulmonic regurgitation
Diamond • starts out at a low intensity, steadily increases in amplitude until it reaches a peak and then steadily decreases.• murmur starts shortly AFTER S1• This shape is characteristic of midsystolic murmurs caused by stenotic valves, e.g. aortic or pulmonic stenosis
Plateau Plateau murmurs maintain a relatively constant intensity
Description of a murmur:

Description of a murmur:
Timing Early, mid, late Length Short, medium, long, panPitch Low, medium, highQuality Vibratory, harsh, rumblingLocation of maximum intensityRadiation of murmur Effect of maneuvers Inspiration, standing, squattingEponym Still’s, Austin Flint, Carey Coombs,
Graham Steell

THANK YOU


























