Embed Size (px)
Citation preview

HEMORRHAGIC FEVER WITH RENAL FAILURE
SYNDROME (HFRS)
Presented by :ARIF KHAN
GROUP: 4TH
COURSE: 5TH

Hemorrhagic fever with renal failure syndrome (HFRS) occurs mainly in Europe and Asia and is characterized by fever and renal failure associated with hemorrhagic manifestations. Hemorrhagic fever with renal failure syndrome is caused by an airborne contact with secretions from rodent hosts infected with the group of viruses belonging to the genus Hantavirus of the family Bunyaviridae. In Europe, hemorrhagic fever with renal failure syndrome is caused by 3 hantaviruses: Puumala virus (PUUV), carried by the bank vole (Myodes glareolus); Dobrava virus (DOBV), carried by the mouse (Apodemus flavicollis); and Saaremaa virus (SAAV), carried by the striped field mouse (Apodemus agrarius).

Hemorrhagic fever with renal failure syndrome was initially recognized between 1913 and 1930 by Soviet scientists, who described sporadic outbreaks of fever with renal failure in the eastern Soviet Union. The disease came to the attention of the Western world in 1950, when the North American soldiers serving with the United Nations forces in Korea developed a febrile illness associated with shock, hemorrhage, and renal failure.

Pathogenesis
the pathogenesis is largely unknown, but findings from several studies have suggested that immune mechanisms play an important role. After the infection, marked cytokine production, kallikrein-kinin activation, complement pathway activation, or increased levels of circulating immune complexes occur. These components play an important role during the febrile and hypotensive stages. Damage to the vascular endothelium, capillary dilatation, and leakage are clinically significant features of the disease.

Transmission Hantaviruses are carried and transmitted by rodents.
People can become infected with these viruses and develop HFRS after exposure to aerosolized urine, droppings, or saliva of infected rodents or after exposure to dust from their nests. Transmission may also occur when infected urine or these other materials are directly introduced into broken skin or onto the mucous membranes of the eyes, nose, or mouth. In addition, individuals who work with live rodents can be exposed to hantaviruses through rodent bites from infected animals. Transmission from one human to another may occur, but is extremely rare.

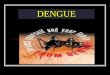
Transmission of Hantaviruses
Chronically infected rodent
Virus is present in aerosolized excreta,
particularly urine
Horizontal transmission of infection by intraspecific aggressive behavior
Virus also present in throat swab and feces
Secondary aerosols, mucous membrane contact, and skin breaches are also sources of
infectionCourtesy of CDC

HFRS
A group of clinically similar diseases that occur throughout Europe and Asia
Includes several diseases that formerly had other names, including Korean hemorrhagic fever, epidemic hemorrhagic fever and nephropathia epidemica
~15% fatality

The clinical features The clinical features in hemorrhagic fever with
renal failure syndrome (HFRS) consist of a triad of fever, hemorrhage, and renal insufficiency.
Other common symptoms during the initial phase of the illness include headache, myalgia, abdominal and back pain, nausea, vomiting, and diarrhea.
Other symptoms include chills, dizziness, increased thirst, costovertebral tenderness, and flank pain.

Stages of Hemorrhagic Fever with Renal Syndrome (HFRS)
1)Incubation (4-40 days)
2)Febrile Phase (3-5 days)
3)Hypotensive Phase (hours to days)
4)Oliguric Phase (3-7 days)
Recovery:
5)Diuretic Phase (2-21 days)
6)Convalescent Phase (2-3 months)

Febrile Phase 3-5 days Characterized by fever, chills Headache, severe myalgia
(muscle pain), nausea Blurred vision, photophobia,
eye pain caused by movement Flushing of face, V-area of the
neck and back Petechiae (small red spots on
skin) Abdominal pain and back pain. Thirst, edema,
hemoconcentration, postural hypotension

Hypotensive phase
Hours to days Blood pressure decrease, hypovolemia (decreased
blood volume), shock Worsening of bleeding manifestations: petechiae,
epistaxis (nosebleed), gastrointestinal and intracranial bleeding
Levels of urea and creatinine in blood rise, proteinuria (excessive protein in urine)
Leukocytosis, thrombocytopenia (decreased # of platelets)

Oliguric Phase• 3-7 days• Marked by decreased urine production due to
renal (kidney) dysfunction• Hypervolemia (high blood volume) leading to
hypertension• Blood electrolyte imbalance• Continuation of hemorrhagic symptoms• Severe complications: cardiac failure pulmonary
edema (swelling of lungs), and cerebral bleeding


Diuretic Phase Several days to several weeks Beginning of recovery 3-6 liters of urine/ day; return to normal
renal activity Anorexia, fatigue due to dehydration

Convalescent Phase
2-3 months Progressive improvement in glomerular
filtration, renal blood flow, and urine concentrating ability

Laboratory Studies Enzyme-linked immunosorbent assay (ELISA) is useful in
detecting antihantaviral-specific immunoglobulin M (IgM) early in the course of the illness.
Antihantaviral immunoglobulin G (IgG) titers may be elevated for prolonged periods (as long as 10 y).
Blood findings usually reveals clinically significant leukocytosis, an elevated or normal hematocrit level, and thrombocytopenia.
Elevated levels of liver enzymes, BUN, and serum creatinine can be observed.
Hyponatremia, hyperphosphatemia, and hyperkalemia may occur during the oliguric phase.
Complement (C3) levels may be decreased; therefore, hemorrhagic fever with renal failure syndrome should be included in the differential diagnosis of hypocomplementemic acute nephritic syndrome.

Imaging Studies Advances in cross-sectional imaging have
allowed early diagnosis of the sequelae of HFRS. In the kidneys, MRI T1-weighted imaging shows a well-defined zone of low-signal intensity (blood product deposition) in the subcortical medulla in 33% of cases, and, in 80% of cases, T2-weighted images correlated with renal histopathological findings of HFRS.

Radiographs of the abdomen may show ascites (74%), paralytic ileus with intestinal wall thickening (69%), retroperitoneal edema (obscured psoas shadow [68%] and obscured renal shadow [53%]), and kidney enlargement (23%). In patients with pulmonary involvement, chest radiography findings include interstitial edema (14-44%), subsegmental atelectasis (38%), pleural effusion (6-32%), and cardiomegaly (6-21%).

Clinical Testing for HFRS
Thrombocytopenia (low platelet count) is a signifier
Urine tests for albuminuria (abnormally high amounts of the plasma protein albumin in the urine)
Urine tests for microhematuria (microscopic amounts of blood in the urine)

Treatment Treatment depends on the stage of the disease and
on the patient's hydration status and hemodynamic condition.
Supportive therapy is the mainstay of care for patients with hantavirus infections. Care includes careful management of the patient’s fluid (hydration) and electrolyte (e.g., sodium, potassium, chloride) levels, maintenance of correct oxygen and blood pressure levels, and appropriate treatment of any secondary infections. Dialysis may be required to correct severe fluid overload. Intravenous ribavirin, an antiviral drug, has been shown to decrease illness and death associated with HFRS if used very early in the disease.