Embed Size (px)
DESCRIPTION
thalassemia
Citation preview

Genetic association studies in �-hemoglobinopathies
Swee Lay Thein1
1Department of Haematological Medicine, King’s College Hospital National Health Service Foundation Trust,
King’s College London School of Medicine, London, United Kingdom
Characterization of the molecular basis of the �-thalassemias and sickle cell disease (SCD) clearly showed thatindividuals with the same �-globin genotypes can have extremely diverse clinical severity. Two key modifiers, an innateability to produce fetal hemoglobin and coinheritance of �-thalassemia, both derived from family and populationstudies, affect the pathophysiology of both disorders at the primary level. In the past 2 decades, scientific research hadapplied genetic approaches to identify additional genetic modifiers. The review summarizes recent genetic studies andkey genetic modifiers identified and traces the story of fetal hemoglobin genetics, which has led to an emergingnetwork of globin gene regulation. The discoveries have provided insights on new targets for therapeutic interventionand raise possibilities of developing fetal hemoglobin predictive diagnostics for predicting disease severity in thenewborn and for integration into prenatal diagnosis to better inform genetic counseling.
IntroductionAmong the hemoglobinopathies, sickle cell disease (SCD) and�-thalassemia have the most impact on morbidity and mortality,affecting millions worldwide.1 Both are prototypical Mendeliansingle gene disorders affecting the �-globin (HBB) gene. Despitethe apparent genetic simplicity, both disorders display extremeclinical heterogeneity.2,3 Major advances have been made in ourunderstanding of the molecular pathology, pathophysiology, andtreatment of these disorders, but predicting the clinical courseremains difficult. This is particularly so for SCD, which presentschallenges in genetic counseling and management. Identification ofthe genetic modifiers could provide more precise estimates ofdisease severity and defining the genetic variation within thepathobiological pathways could provide clues and targets fortherapeutic intervention.
The 2 major modifiers, an innate ability to produce fetal hemoglobin(HbF, �2�2) and coinheritance of �-thalassemia, have been derivedfrom more than 50 years of extensive biochemical and pathophysi-ological studies and were subsequently confirmed by geneticstudies. The mechanisms of the modifying effects of HbF and�-thalassemia in SCD and �-thalassemia could not be moredifferent at the molecular level,yet these genetic modifiers have alarge clinical effect due to their impact on disease pathophysiologyat the primary level. In addition, the genetic variants are commonand their contribution to disease burden is substantial.
Rationale for genetic studies and approaches used todemonstrate genetic modifiersHbF levels and coinheritance of �-thalassemia are unlikely to be theonly major modifiers because they do not completely explain theclinical diversity in either disorder. In SCD, for example, analysis ofsibling pairs suggested a genetic contribution to stroke risk notexplained by HbF levels or coinheritance of �-thalassemia; a childwith sickle cell anemia (SCA) has an increased risk of stroke if theyhave had siblings who have experienced an overt stroke. Studieshave also shown a concordance in response to hydroxyurea therapyamong siblings. Observations of clinical variability between identi-cal twins (who have identical genetic make-up)4 and longitudinallywithin the same individual highlight the important contribution of
environmental factors to the phenotypic variability. Environmentalfactors such as physical activity, diet, and toxins can elicit changesin the gene activity (altering epigenome or “software”) withoutchanging the DNA code (or “hard-drive”). Such epigenetic changesmay account for the discordant clinical phenotypes in identicaltwins and contribute to the complex disease etiology in bothdisorders.5 Due to the complex interaction of the multiple factors, agenetic approach might be the most efficacious way of identifyingthe modifier genes and provide a better understanding of the diseasemechanisms.
All 3 approaches that are generally used to unravel genetic modifiersin human disorders have been applied to the �-hemoglobinopathies:mouse models, family and epidemiological studies, and geneticassociation studies. Although mouse models of �-thalassemia andSCD2 have been very important in providing proof-of-principle forglobin gene regulation along with development and testing oftherapeutic compounds, no novel genetic modifiers have beendiscovered using this approach. In part, this may be due to a lack ofmouse models that replicate the complications encountered in SCD(eg, stroke). Insights into the 2 major genetic modifiers, HbF levelsand �-globin genotype, were derived from an understanding of thedisease pathophysiology and were subsequently validated by familyand population genetic association studies (Tables 1, 2). Associationof serum bilirubin levels and predisposition to gallstones withpolymorphisms in the promoter of the UGT1A1 gene (Gilbertsyndrome) have been consistently demonstrated in many studies inpatients with �-thalassemia and SCD of all ages and differentpopulations.6,7 A recent single study suggested that the MYH9-APOL1 locus, an important genetic risk factor for renal failure innon-SCD population of African ancestry, is also associated withsickle cell nephropathy.8 These association studies were based oncandidate genes selected according to one’s understanding of thedisease pathophysiology or prompted by association with the samephenotypes in non-SCD populations.9
Candidate gene association studies look for differences in thefrequencies of genetic variants in targeted genes between cases andcontrols. If a variant is more common in cases than controls, thenassociation can be inferred. The more recent genome-wide genetic
HEMOGLOBINOPATHIES: FRESH IDEAS FOR MANAGEMENT
354 American Society of Hematology

association studies (GWAS) involve an unbiased scan of the wholehuman genome and, by design, are more likely to reveal unsus-pected interactions. GWAS will also confirm previous candidategenes if the association is robust.10,11 A case in point is theapplication of GWAS in the highly successful discovery of BCL11A(an oncogene that hitherto was not known to have a role inerythropoiesis) as a quantitative trait locus (QTL) controllingHbF.10,12 GWAS also confirmed association of the other 2 loci,Xmn1-HBG2 (rs782144) on chromosome 11p and HBS1L-MYB(HMIP) on chromosome 6q, which were previously discoveredthrough candidate and genetic linkage studies, with HbF production.Similarly, GWAS confirmed the association between bilirubin leveland UGT1A1 polymorphism in SCD.11
It has become clear from the genetic association studies of HbF andother common diseases and traits that GWAS can work13 but thatsample size matters, that clearly defined and well harmonizedphenotypes are critical, that replication and collaboration (interdisci-plinary in addition to increasing sample size) matters, that currenthypotheses regarding candidate genes and pathways may not matter
so much, and that several genes can influence more than one diseaseor trait. It has also become evident that simpler phenotypes such asHbF, which are reproducible, measurable, and disease related, aremuch more robust and successful in genetic association studies thanclinical end points. Such intermediate end points or endophenotypesare often quantitative traits and thus provide more power in geneticstrategies. For quantitative continuous traits, one could focus onextremes of the trait as a strategy to reduce genotyping or sequencingcosts, as was successfully applied in the GWAS for HbF and F cells.10
The brain is one major site of morbidity in children with SCD.Increased velocity in the middle cerebral artery as detected bytranscranial Doppler (TCD) screening is a biomarker of earlycerebrovascular disease. Studies have shown that chronic bloodtransfusion therapy at this stage can prevent overt stroke. Trueprimary stroke prevention, however, should prevent vascular dam-age before TCD velocity becomes abnormal. TCD velocity wouldtherefore be an extremely attractive endophenotype in studies fordetecting genetic variants associated with sickle vasculopathy andstroke risks.
Table 1. Genetic modifiers of SCD
A. Primary at level of HbS polymerization and sicklingModifier Mechanism
1. Sickle genotype; HbSS, HbSC, HbS�-thalassemia Affects HbS polymerization2. Coinheritance of HbF QTLs Hybrid tetramer (�2�S�) does not take part in HbS polymerization and HbF dilutes
intracellular HbS concentration3. Coinheritance of �-thalassemia �-thalassemia reduces intracellular HbS concentration, decreases HbS
polymerization and hemolysisB. Secondary at level of subphenotypes and complications
Modifier Complication and mechanism1. UGT1A1 promoter (TA)n polymorphism Hyperbilirubinemia and gallstones2. MYH9–APOL1 locus Proteinuria and sickle cell nephropathy3. ADYC9, ANXA2, TEK and TGFBR3 Ischemic stroke risk, mechanisms unclear4. GOLGB1 and ENPP1 Ischemic stroke risk, mechanisms unclear5. TGF�-/SMAD /BMP pathway Multiple subphenotypes including osteonecrosis, acute chest syndrome, pulmonary
hypertension, leg ulceration, renal impairment, infection, priapism6. KLOTHO (KL) Priapism, mechanisms unclear7. NPRL3 on Chr16p Reduces hemolysis, �-thalassemia effect suggested
Most modifiers that affect SCD at the secondary level of subphenotypes and complications have not been replicated.
Table 2. Genetic modifiers of �-thalassemia
A. Primary at level of �: non-�-globin chain imbalanceModifier Mechanism
1. �-globin genotype (one or two, and severity of�-thalassemia alleles)
Directly affects output of �-globin and chain imbalance
2. �-globin genotype�-thalassemia Reduces chain imbalance and �-globin excessCoinheritance of extra �-globin genes (���/, ����/,or HBA cluster duplication)
Increases �-globin excess and chain imbalance
3. Co-inheritance of HbF QTLs, eg, SNPs in BCL11A,HMIP, Xmn1-HBG2
Increased � chains combine with excess �-reducing chain imbalance
4. Potential modifiers include variants in ubiquitinproteolytic pathway
Promotes proteolysis of excess �-globin
5. �-hemoglobin stabilizing protein (AHSP) Chaperones excess �-globin (studies inconclusive)B. Secondary at level of complications related to disease and therapy
Modifier Complication and mechanism1. UGT1A1 promoter (TA)n polymorphisms Hyperbilirubinemia and gallstones2. HFE–eg.H63D variants Iron loading due to increased GI absorption3. Variants in VDR, COL1A1, COL1A2, TGFB1 genes Osteopenia and osteoporosis, modification of bone mass4. Apolipoprotein (APOE) �4 Cardiac disease, risk factor for left ventricular heart failure,
mechanism unknown5. Glutathione-S-transferase M1 Increase risk of cardiac iron loading, mechanism unknown
Hematology 2013 355

Whole genome or exome sequencing using next-generation sequenc-ing technology in combination with well-defined phenotypes offersthe possibility of identifying new genetic variants. GWAS incombination with exome sequencing identified mutations inGOLGB1 and ENPP1 with stroke protection in SCA.14 In this study,overt stroke was the clinical marker, but these variants have yet tobe independently validated in a different population group.
Review of genetic modifiers in �-hemoglobinopathiesFor both SCD and �-thalassemia, factors that affect the primaryevent of the disease process will have a global effect on the diseasephenotype. These include the causative genotype, coexisting �-thala-ssemia, and the innate ability to produce HbF.
SCD should be considered as both a qualitative and quantitativegenetic disorder in that it is caused by the presence of an abnormalHb variant (HbS, �2�2
S, HBB glu6val, GAG �6 GTG), yet thelikelihood of HbS polymerization and sickling is highly dependenton the intra-erythrocyte HbS concentration. Homozygosity for HbS(SCD-SS) or SCA is the most common genotype; the othercausative genotypes include compound heterozygous states of HbSwith HbC (SCD-SC) or �-thalassemia variants (SCD-S�0 thalasse-mia and SCD S�� thalassemia).2 Individuals with SCD-SS orSCD-S�0 thalassemia, in whom the intracellular hemoglobin compo-sition is almost all HbS, have the most severe disease, followed bySCD-SC and SCD S�� thalassemia. Simple heterozygotes for HbS(HbAS) who have 30% to 40% intracellular HbS, with HbA inexcess of HbS, are asymptomatic. Under exceptional circumstances,however, such as intense physical activity and dehydration, theconsequent increased intracellular HbS concentration can inducevasoocclusive pain.
Approximately one-third of SCD patients of African descent havecoexisting �-thalassemia due to the common deletional variant(��3.7/).2 The majority are heterozygous (��/��), with 3% to 5%homozygous for the deletion (��/��). Coexisting �-thalassemiareduces intracellular hemoglobin concentration, thereby reducingHbS polymerization, reducing sickling, and decreasing hemolysis.Although the coexisting �-thalassemias have a protective effectagainst complications associated with severe hemolysis, such aspriapism, leg ulceration, and albuminuria, the increased hematocritand blood viscosity may account for the increase in other complica-tions associated with microvascular occlusion, such as increasedacute pain, acute chest syndrome, osteonecrosis, and retinopathy.15
Coexisting �-thalassemia also reduces bilirubin with a quantitativeeffect that is independent to that of the UGT1A1 promoter polymor-phism.7 In Jamaicans, the absence of �-thalassemia and higher HbFlevels predict a benign disease. A subsequent analysis of 40 elderlyJamaican patients (� 60 years of age), however, suggested thatcoexisting �-thalassemia may promote longevity (51% had coexist-ing �-thalassemia), but the trend failed to reach significance.16
Coinheritance of �-thalassemia blunts the response to hydroxyureatherapy in SCD, which may be explained by its effect on HbF levelsand mean cell volume, 2 key parameters associated with hy-droxyurea response.17 It is quite likely that �-thalassemia carrierscould have a poorer response to RBC membrane channel blockersthat aims to reduce sickling through preservation of cell hydration.
HbF reduces the propensity for HbS polymerization; the hybridtetramers (�2�2�) inhibit HbS polymerization and the presence ofHbF dilutes down the intracellular HbS concentration. In view of itsimpact at the primary level of disease pathology, one would expectHbF levels to have a global beneficial effect. Indeed, HbF levels are
a major predictor of survival in SCD, and low levels of HbF havebeen associated with increased risk of brain infarcts in youngchildren.18 At the subphenotype level, apart from the clear benefit ofhigh HbF levels with acute pain and leg ulceration, there aredisparities and less conclusive evidence for its effects on othercomplications such as stroke, renal impairment, retinopathy, andpriapism.15 These disparate conclusions are likely to arise fromsmall sample sizes, even smaller numbers of end complications, anddisparities in ascertainment of phenotypes. The uneven beneficialeffect of HbF on sickle-related complications could also be relatedto the different pathobiology of large and small vascular disease.
HbF levels vary considerably, from 1% to as high as 25% inindividuals with SCD-SS, and behave as a quantitative genetic traitas in healthy individuals. Three QTLs, one in cis to the HBB genecluster represented by the Xmn1-HBG2 site (rs7482144), HBS1L-MYB intergenic polymorphisms (HMIP) on chromosome 6q, andBCL11A on chromosome 2p, are major regulators of common HbFvariation.10,12,19-22 Their effect on HbF levels varies with thefrequency of the HbF boosting (minor) alleles in different popula-tion groups. In patients of African descent with SCD, the 3 lociaccount for 16% to 20% of the variation in HbF levels with acorresponding reduction in acute pain rate.23,24 The favorable effectof HbF and its modifiers (BCL11A and Xmn1-HBG2) variants onpain and TCD velocities is measurable even in young infants, asdemonstrated in the recently completed BABY HUG study.25
Several studies have investigated the association of candidate genesimplicated in pathophysiology of vasoocclusion and vasculopathy,such as those encoding factors modifying inflammation, oxidantinjury, nitric oxide biology, vasoregulation, and cell adhesion, withsickle-related complications, including stroke, priapism, leg ulcers,avascular necrosis, renal disease, acute chest syndrome, gallstones,and susceptibility to infection.15,26,27 The majority of the reportedassociations have not been replicated or validated and are likely tobe false positives. Of the numerous association studies reported, themost robust is the association between serum bilirubin levels andpredisposition to gallstones with the 6/7 or 7/7 (TA) repeats in theUGT1A1 promoter.11 UGT1A1 polymorphism continued to have astrong influence even during hydroxyurea therapy; in one study,children with the 6/6 UGT1A1 genotype achieved normal bilirubinlevels, whereas children with 6/7 or 7/7 UGT1A1 genotypes didnot.6
Suggestions of a familial predisposition to stroke and its devastatingconsequences has prompted numerous genetic and clinical associa-tion studies on cerebrovascular complications involving either largeor small vessels.14,28,29 Of the 38 published single nucleotidepolymorphisms (SNPs) associated with stroke, the effects of�-thalassemia and SNPs in four genes (ADYC9, ANXA2, TEK, andTGFBR3) could be replicated, although only nominally significantassociation results were obtained.30 More recently, GWAS incombination with whole-exome sequencing have identified muta-tions in 2 genes, GOLGB1 and ENPP1, which are associated withreduced stroke risk in pediatric patients, but, again, this needsvalidation in independent studies.14 To overcome the small samplesize in end point complications, a study used a compound phenotypethat included one or more sickle-related complications (see reviewby Thein27). Patients with complications had a higher frequency ofthe platelet glycoprotein allele HPA-5B. In this small study, most ofthe complications were osteonecrosis and only 4 individuals hadmore than one complication. Because traditional methods are ofteninadequate in association studies of complex traits, methods of
356 American Society of Hematology

evaluating multilocus data are promising alternatives. A GWAS wasapplied to SCD based on a disease severity score that was derivedfrom a Bayesian network that integrates 25 different clinical andlaboratory variables.31 Several genes not known to be related to thepathogenesis of SCD were identified, including KCN6 (a potassiumchannel protein) and TNK5 (a gene encoding tankyrase-1, a possibletelomere length regulator). However, it is important to rememberthat results from such analytical techniques are dependent on thestructure of a model assuming certain causalities and probabilitiesof the different variables. More recently, GWAS identified an SNP(rs7203560) in NPRL3 on chromosome 16p that was independentlyassociated with hemolysis (using a score derived by principlecomponent analysis).32 rs7203560 is in perfect linkage disequilib-rium with SNPs within the �-globin gene regulatory elements(HS-48, HS-40, and HS-33). rs720356 is also in linkage disequilib-rium with ITFG3 that is associated with RBC mean cell volume andmean cell hemoglobin in several GWAS of different populationgroups.33 It is proposed that NPRL3 reduces hemolysis through anindependent thalassemic effect on the HBA1/HBA2 genes.
Hydroxyurea remains a major treatment option for SCD; its maineffect is mediated primarily through induction of HbF. Clinicalresponse to hydroxyurea therapy, however, is variable with variableHbF response; a main determinant of response appears to be thebaseline HbF levels. Numerous genetic association studies on HbFresponse to hydroxyurea have been reported, of which the associa-tion with Xmn1-HBG2 seems to be the most robust. In the recentlycompleted BABY HUG trial, however, the HbF genetic modifierswere not able to identify the “high” and “low” responders tohydroxyurea.25 Table 1 summarizes the genetic modifiers of SCD.
In �-thalassemia, as in SCD, the causative genotype, coinheritanceof �-thalassemia and HbF, are the main modifiers of clinicalseverity. These genetic factors have a major impact because theyaffect the central mechanism underlying disease pathophysiology(ie, the degree of globin chain imbalance and the excess of �-globinchains). Almost 300 mutations (deletions and point mutations) thatdown-regulate the �-gene have been described (http://globin.bx.psu.edu/hbvar/menu.html). Functionally, the mutations range fromnull mutations (�0 thalassemia) that cause a complete absence of�-globin production to those that cause a minimal deficit: ���
thalassemia (sometimes referred to as silent �-thalassemia becauseof the minimally reduced RBC indices and normal HbA2 levels inheterozygotes).34 The causative �-globin genotype has the largestimpact on disease severity. Homozygotes or compound heterozy-gotes for 2 �0 thalassemia alleles cannot produce any HbA (�2�2);such individuals generally have the most severe anemia and dependon blood transfusions for life (thalassemia major).
In many populations in which �-thalassemia is prevalent, �-thalassemia also occurs at a high frequency. Individuals who havecoinherited �-thalassemia have less redundant �-globin and tend tohave less severe anemia. The degree of amelioration depends on theseverity of the �-thalassemia alleles and the number of functional�-globin genes. At one extreme, patients who have coinherited theequivalent of only one functioning �-globin (�/��, HbH genotype)with homozygous �-thalassemia have less severe anemia (thalasse-mia intermedia) if the �-thalassemia alleles are ��, but a moresevere phenotype if they have �0 thalassemia.3
In heterozygous individuals with one �-thalassemia allele, coinheri-tance of �-thalassemia normalizes the hypochromia and microcyto-sis, but the elevated HbA2 levels remain unchanged. Increased
�-globin production through coinheritance of extra �-globin genes(triplicated, ���/��� or ���/���; quadruplicated, ����/��; orduplication of the whole �-globin gene cluster, ��/��/��) withheterozygous �-thalassemia tips the globin chain imbalance further,converting a typically clinically asymptomatic state to thalassemiaintermedia. The severity of anemia depends on the number of extra�-globin genes and the severity of the �-thalassemia alleles.
Increased HbF response as an ameliorating factor becomes mostevident in non-transfusion-dependent �0 thalassemia patients whohave a mild disease despite the complete absence of HbA.35 In thiscase, the increased �-chains combine with the redundant �-globin toform HbF (�2�2), reducing the chain imbalance. Again, the degreeof amelioration depends on the severity of �-thalassemia alleles (��
or �0) and the number of coinherited HbF genetic determinants(common QTLs including BCL11A, Xmn1-G� -158 C3T and SNPsin HMIP on chromosome 6q.12,36-39
At the primary level of chain imbalance, the proteolytic capacity ofthe erythroid precursors in catabolizing the excess �-globin hasoften been suggested, but this effect has been difficult to define.�-hemoglobin–stabilizing protein, a molecular chaperone of �-glo-bin, has also been suggested as another genetic modifier, but itsimpact on disease severity has been inconclusive.40
Genetic variants could also modify the different complications of�-thalassemia that are directly related to the anemia and ineffectiveerythropoiesis or to therapy, such as iron chelation treatment. Thesecondary complications include jaundice and predisposition togallstones, osteopenia, and osteoporosis; iron overload; and cardiacdisease (see Table 2 for modifiers of �-thalassemia). The degree ofiron loading, bilirubin levels, and bone mass are quantitative genetictraits and thus will be modified by genetic variants regulatingexpression of these traits.
HbF concentration is a major modifier of disease severity for both�-thalassemia and SCD, prompting decades of study into itsregulation in adults.41 The study of HbF quantitative genetics andmolecular control of hemoglobin switching mirrors the rapidlyevolving focus of genomics research in humans, from the study ofnatural mutants, gene mapping, and GWAS to applications of theother “-omics” technologies such as comprehensive gene expressionprofiling and DNA-protein interactions. Studies of the deletions inthe HBB cluster associated with heterocellular persistence of fetalhemoglobin (HPFH)2 indicated a “repressive” element in theintergenic region between the A�-globin (HBG1) and �-globin(HBD) genes and enhancer elements downstream of the HBB gene.Point mutations associated with HPFH are clustered in regions ofthe �-globin gene promoters that subsequently proved to be bindingsites for ubiquitous and erythroid-specific transcription factors.Although the HPFH phenotypes could be reproduced in transgenicmice carrying the human �-globin locus and the mutations shown toalter in vitro binding patterns, unambiguous identification ofproteins directly involved in globin switching remained elusive. Avariety of transcription factors with roles in globin gene regulation,such as GATA-1, KLF1, and SCL/TAL, were identified, but howthey regulate the switch from fetal to adult hemoglobin was still notevident.41
Nonetheless, studies of these HPFH mutants and discovery of theupstream regulatory elements (�-locus control region) triggered aseries of experiments and led to the concept that switching of fetal toadult hemoglobin involves 2 mechanisms: autonomous silencing of
Hematology 2013 357

the fetal globin genes and competitive access of the adult globingene to the upstream �-locus control region. However, it wasdifficult to reconcile these concepts of Hb switching with thecommon variable persistence of HbF in healthy adults and inpatients with SCD and �-thalassemia. In many cases, the inheri-tance patterns of the modestly elevated HbF levels are not clear andnot linked to the HBB cluster on chromosome 11. An early exampleis an extended family of Asian-Indian origin, in which segregationanalysis showed that the genetic determinant for HPFH wasinherited independently from the HBB cluster and eventuallymapped to chromosome 6q23.19 Observations of variable HbF withdifferent �S haplotypes first suggested that the HBB cluster is aprime location for a HbF determinant, represented by the C3TSNP (rs7482144) at position �158 of the G� promoter, known asthe Xmn1-HBG2 polymorphism.2 By early 2006, developments ingenetic tools and genotyping platforms expedited by the Interna-tional Human Genome HapMap Project enabled the development ofGWAS that led to the identification of BCL11A on chromosome2p16 as another locus modifying �-globin levels.10,12 The next cluein the hemoglobin-switching puzzle again came from humangenetics provided by a Maltese family in which 10 of 27 membershad HPFH that segregated independently from the HBB cluster.42
Genetic studies followed by expression profiling of erythroidprogenitors identified KLF1 as the �-globin modifier in this familyin which members with HPFH were heterozygous for the nonsensep.K288X mutation in KLF1. Soon, a steady stream of novelmutations in KLF1 associated with increases in HbF were reportedin different populations (for review, see Borg et al43). The increasesin HbF occurred as a primary phenotype or in association with RBCdisorders such as congenital dyserythropoietic anemia.
Functional studies in primary human erythroid progenitors andtransgenic mice demonstrated that BCL11A acts as a repressor of�-globin; the silencing effect involves reconfiguration of the HBBlocus through interaction with GATA-1 and SOX6 that binds theproximal �-globin promoters.44,45 Profiling of erythroid cells fromthe Maltese family showed that KLF1 p.K288X carriers had reducedBCL11A expression.42 KLF1 was also shown to be a direct activatorof BCL11A in human erythroid progenitor cells and in transgenicmice.42,46 Previous knockout studies in mice had shown that KLF1is essential for activation of �-globin expression, but the embryonicand fetal globin genes remain fully activated in the absence ofKLF1.47 Collectively, these results have led to the proposal thatKLF1 has dual functions in the �-globin to �-globin switch: KLF1activates HBB directly and also silences the �-globin gene indirectlyvia activation of BCL11A.47
High-resolution genetic mapping and resequencing refined the 6qQTL to variants in a 24-kb region between the HBS1L and MYBgene, referred to as HMIP block 2.19 Work in primary humanerythroid progenitor cells48 and transgenic mice showed that thisregion contains distal enhancers required for MYB activation.49,50
MYB, which encodes the c-MYB transcription factor, is a keyregulator of hematopoiesis and erythropoiesis. One suggestion ofhow MYB modulates HbF levels is via its effects on erythroidproliferation/differentiation balance. A low MYB environmentfavors accelerated erythropoietic differentiation, leading to therelease of early erythroid progenitors that are still synthesizingpredominantly HbF.51 Another suggestion is that MYB repressesfetal globin gene expression via KLF1 activation of BCL11A.52 Athird suggestion is that MYB works via its effects on the TR2/TR4pathway. MYB up-regulates the nuclear receptors TR2/TR4, whichare repressors of the �-globin gene. Therefore, down-regulation of
MYB leads to suppression of the TR2/TR4 pathway and up-regulation of fetal globin gene expression. The emerging network ofHbF regulation also includes SOX6; chromatin-modeling factorFOP; the NuRD complex; the orphan nuclear receptors TR2/TR4(part of direct repeat erythroid definitive [DRED]); the proteinarginine methyltransferase PRMT5, involving DNA methylation;and HDACs 1 and 2, which are epigenetic modifiers53 (Figure 1).Regulators of the key TFs, such as microRNA-15a and 16-1, incontrolling MYB54,55 could also have a potential role in regulatingHbF levels.
Prospective targets for therapeutic induction of HbFIdentification of these genetic loci regulating HbF levels hasrevealed cellular pathways providing insights for new therapeutictargets for increasing HbF (Figure 1). The ideal target would be onethat mimics and enhances the effect of the genetic variants that havebeen identified in modulating HbF levels, but does not affect otherbiological pathways. Targets identified in the emerging network ofHbF regulation include MYB, KLF1, and BCL11A. ManipulatingMYB to achieve an adequate therapeutic window could be problem-atic due to its pleiotropic role in hematopoiesis. KLF1 appears to bekey in the �-globin to �-globin switch; although KLF1 expression isalmost exclusively restricted to erythroid cells, there would bedifficulty in achieving specificity due to its broad array of erythroidactivity.47 Reducing BCL11A activity is an attractive approach;proof-of-principle in HbF reactivation has already been demon-strated in a variety of systems, including cell lines, primary humanerythroid cells, transgenics, and a mouse model of SCD withreversal of characteristic organ damage.56 However, BCL11A hasessential roles in neuronal and B-lymphocyte development. Otherpromising targets include the DNA-methylating and histone-modifying enzymes. Proof-of-principle has already been providedby the effective in vivo HbF induction properties of 5-azacytidineand decitabine, both of which target the DNA methyltransferaseDNMT1.2 Another attractive target is modulating expression of theorphan nuclear receptors TR2/TR4; one approach is inhibition oflysine-specific demethylase 1 (LSD1) via tranylcypromine (TCP),an antidepressive agent.57
From genetics to more precise risk prediction?Although environmental factors are important in determining theclinical outcome of both SCD and �-thalassemia, it is evident thatthe genetic background of the affected individual imparts a substan-tial contribution to the clinical severity and response to ironchelators and hydroxyurea. Over the past 20 years, numerousassociation studies have been published and roles for many modify-ing factors and genes proposed, but the results are questionablebecause of the lack of replication. Furthermore, the genetic evidencegenerated about the phenotype has not been supported by functionalassays or relevant models. Even if the variants are verified, they arelikely to explain only a small fraction of the phenotype variationand, therefore, have limited predictive value and clinical utility.
One exception is HbF genetics. HbF levels in adults are highlyheritable and controlled by 3 main loci, BCL11A, HBS1L-MYBintergenic polymorphisms, and Xmn1-HBG2. In healthy Europeans,the 3 loci explained more than 44% of the total variance in HbFlevels (BCL11A 15.1%, HMIP 19.4%, and Xmn1-HBG2 10.2%),10
whereas in African patients with SCA, the 3 loci contribute from16% (Tanzanians)24 to 20% (African Americans)23 of the HbFvariance, with a corresponding reduction in frequency of acutepainful crises. The impact of the HbF QTLs on HbF response and
358 American Society of Hematology
reduction in blood transfusion requirements has also been demon-strated in patients with �-thalassemia and HbE/�-thalassemia.12,38
The relatively large fraction (20%-50%) of phenotypic variation inHbF explained through a limited number of genetic loci is uniquefor a disease-relevant trait in humans compared with other traits andcomplex disorders, For example, in Crohn disease, 20% to 23% ofdisease risk can be explained by 71 QTLs.13 HbF could be the firsthuman quantitative trait to be effectively predicted through geneticassay systems and its value tested to inform clinical or pharmacoge-netic management (eg, response to HbF-activating agents).
Based on the current state of knowledge, the 3 HbF QTLs should beable to predict an individual’s ability to produce HbF within aclinically meaningful confidence limit. Studies in Sardinia andFrance showed that a combination of the Xmn1-HBG2 site, SNPs inBCL11A and HMIP, together with �-globin genotypes can predict75% to 80% of disease severity in �-thalassemia.37,39 In a cohort of316 �0 thalassemia patients, delayed or absent transfusion needswere correlated with status of the 3 HbF QTLs and the �-globingenotype.58 In a recent study of patients with SCA, a panel of 14SNPs comprising 6 from BCL11A and the rest from chromosome11p15 encompassing the HBB gene complex and olfactory receptorgene region explained 23.4% of HbF variability.59 The value of HbFpredictive genetics lies in the newborn and early childhood stage,when it may be possible to combine this knowledge with otherlaboratory and clinical parameters (eg, dactylitis in infants, leuko-cyte count, hemoglobin level, and TCD velocity) to predict severedisease outcomes such as stroke, frequent pain crises, and acutechest syndrome in SCA,25 thus facilitating early implementation ofpreventive therapy. In �-thalassemia, HbF predictive diagnostics
could be integrated with information on �-globin and �-globingenotypes to better inform genetic counseling.
ConclusionThe generation of a personalized genetic risk score to informprognosis and guide therapeutics has been a major driver underlyinggenetic association studies in numerous diseases and traits, includ-ing the �-hemoglobinopathies.60 A challenge that faces all GWAS isthe translation of genetic risk variants into clinical utility. In thisregard, predictive HbF genetics has 2 advantages: (1) the clinicalimpact of HbF is well documented and (2) a limited number ofQTLs account for a substantial proportion of the trait variance.Already, identification of the loci regulating HBG production hasprovided new insights and leads for therapeutic HbF reactivation. ADNA assay-based diagnostic for the testing of one’s ability toproduce HbF could provide predictive information for those at riskof early complications. The success of predictive testing will dependon continued accurate identification of genetic and environmentalfactors and its ultimate clinical utility.
AcknowledgmentsThe author thanks Claire Steward for help in preparation of themanuscript and apologizes to the many investigators whose workcould not be cited due to space limitations.
DisclosuresConflict of interest disclosure: The author declares no competingfinancial interests. Off-label drug use: None disclosed.
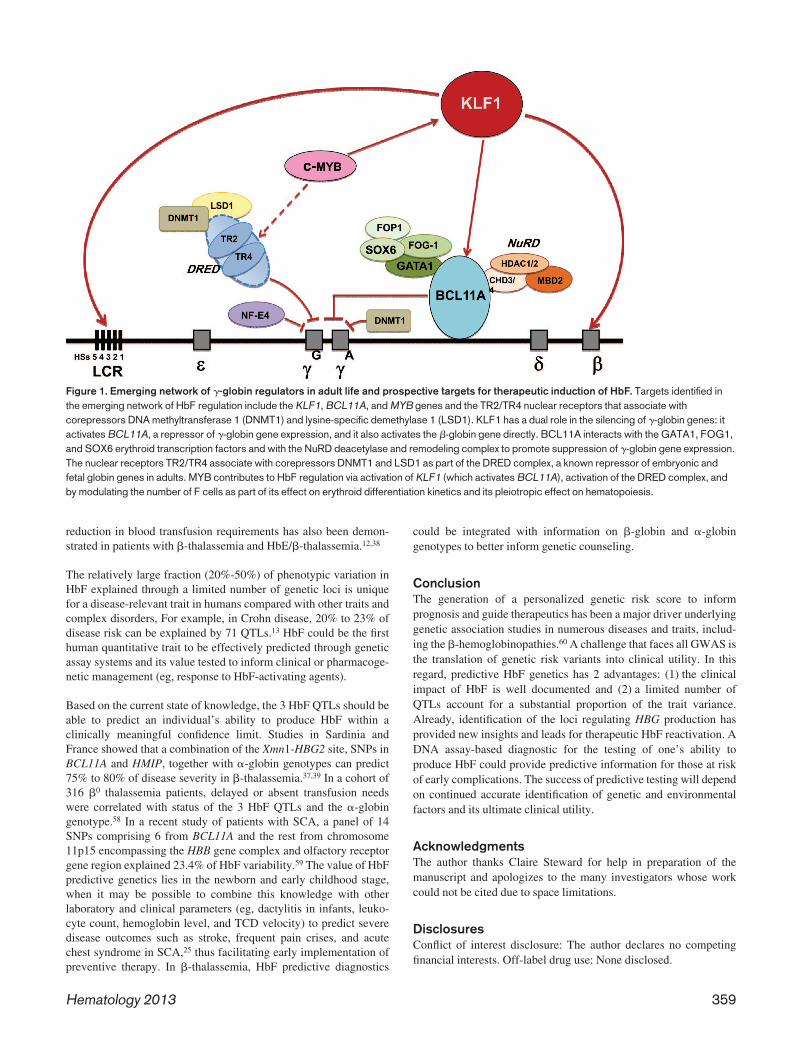
Figure 1. Emerging network of �-globin regulators in adult life and prospective targets for therapeutic induction of HbF. Targets identified inthe emerging network of HbF regulation include the KLF1, BCL11A, and MYB genes and the TR2/TR4 nuclear receptors that associate withcorepressors DNA methyltransferase 1 (DNMT1) and lysine-specific demethylase 1 (LSD1). KLF1 has a dual role in the silencing of �-globin genes: itactivates BCL11A, a repressor of �-globin gene expression, and it also activates the �-globin gene directly. BCL11A interacts with the GATA1, FOG1,and SOX6 erythroid transcription factors and with the NuRD deacetylase and remodeling complex to promote suppression of �-globin gene expression.The nuclear receptors TR2/TR4 associate with corepressors DNMT1 and LSD1 as part of the DRED complex, a known repressor of embryonic andfetal globin genes in adults. MYB contributes to HbF regulation via activation of KLF1 (which activates BCL11A), activation of the DRED complex, andby modulating the number of F cells as part of its effect on erythroid differentiation kinetics and its pleiotropic effect on hematopoiesis.
Hematology 2013 359

CorrespondenceSwee Lay Thein, King’s College London School of Medicine,Molecular Haematology, The James Black Centre, 125 ColdharbourLane, London SE5 9NU, United Kingdom; Phone: 44-20-7848-5443/5447; Fax: 44-20-7848-5444; e-mail: [email protected].
References1. Weatherall DJ. The inherited diseases of hemoglobin are an
emerging global health burden. Blood. 2010;115(22):4331-4336.
2. Steinberg MH, Forget BG, Higgs DR, Weatherall DJ, eds.Disorders of hemoglobin: genetics, pathophysiology, and clini-cal management. 2nd Ed. Cambridge, UK: Cambridge Univer-sity Press; 2009.
3. Galanello R, Origa R. Beta-thalassemia. Orphanet J Rare Dis.2010;5:11.
4. Weatherall MW, Higgs DR, Weiss H, Weatherall DJ, SerjeantGR. Phenotype/genotype relationships in sickle cell disease: apilot twin study. Clin Lab Haematol. 2005;27(6):384-390.
5. Rakyan VK, Down TA, Balding DJ, Beck S. Epigenome-wideassociation studies for common human diseases. Nat RevGenet. 2011;12(8):529-541.
6. Heeney MM, Howard TA, Zimmerman SA, Ware RE. UGT1Apromoter polymorphisms influence bilirubin response to hy-droxyurea therapy in sickle cell anemia. J Lab Clin Med.2003;141(4):279-282.
7. Vasavda N, Menzel S, Kondaveeti S, et al. The linear effects ofalpha-thalassaemia, the UGT1A1 and HMOX1 polymorphismson cholelithiasis in sickle cell disease. Br J Haematol. 2007;138(2):263-270.
8. Ashley-Koch AE, Okocha EC, Garrett ME, et al. MYH9 andAPOL1 are both associated with sickle cell disease nephropa-thy. Br J Haematol. 2011;155(3):386-394.
9. Genovese G, Friedman DJ, Ross MD, et al. Association oftrypanolytic ApoL1 variants with kidney disease in AfricanAmericans. Science. 2010;329(5993):841-845.
10. Menzel S, Garner C, Gut I, et al. A QTL influencing F cellproduction maps to a gene encoding a zinc-finger protein onchromosome 2p15. Nat Genet. 2007;39(10):1197-1199.
11. Milton JN, Sebastiani P, Solovieff N, et al. A genome-wideassociation study of total bilirubin and cholelithiasis risk insickle cell anemia. PLoS One. 2012;7(4):e34741.
12. Uda M, Galanello R, Sanna S, et al. Genome-wide associationstudy shows BCL11A associated with persistent fetal hemoglo-bin and amelioration of the phenotype of beta-thalassemia.Proc Natl Acad Sci U S A. 2008;105(5):1620-1625.
13. Lander ES. Initial impact of the sequencing of the humangenome. Nature. 2011;470(7333):187-197.
14. Flanagan JM, Sheehan V, Linder H, et al. Genetic mapping andexome sequencing identify 2 mutations associated with strokeprotection in pediatric patients with sickle cell anemia. Blood.2013;121(16):3237-3245.
15. Steinberg MH, Sebastiani P. Genetic modifiers of sickle celldisease. Am J Hematol. 2012;87(8):795-803.
16. Serjeant GR, Higgs DR, Hambleton IR. Elderly survivors withhomozygous sickle cell disease. N Engl J Med. 2007;356(6):642-643.
17. Vasavda N, Badiger S, Rees D, Height S, Howard J, Thein SL.The presence of alpha-thalassaemia trait blunts the response tohydroxycarbamide in patients with sickle cell disease. Br JHaematol. 2008;143(4):589-592.
18. Wang WC, Pavlakis SG, Helton KJ, et al. MRI abnormalities of
the brain in one-year-old children with sickle cell anemia.Pediatr Blood Cancer. 2008;51(5):643-646.
19. Thein SL, Menzel S, Peng X, et al. Intergenic variants ofHBS1L-MYB are responsible for a major quantitative traitlocus on chromosome 6q23 influencing fetal hemoglobin levelsin adults. Proc Natl Acad Sci U S A. 2007;104(27):11346-11351.
20. Sedgewick AE, Timofeev N, Sebastiani P, et al. BCL11A is amajor HbF quantitative trait locus in three different populationswith beta-hemoglobinopathies. Blood Cells Mol Dis. 2008;41(3):255-258.
21. Bhatnagar P, Purvis S, Barron-Casella E, et al. Genome-wideassociation study identifies genetic variants influencing F-celllevels in sickle-cell patients. J Hum Genet. 2011;56(4):316-323.
22. Bae HT, Baldwin CT, Sebastiani P, et al. Meta-analysis of 2040sickle cell anemia patients: BCL11A and HBS1L-MYB are themajor modifiers of HbF in African Americans. Blood. 2012;120(9):1961-1962.
23. Lettre G, Sankaran VG, Bezerra MA, et al. DNA polymor-phisms at the BCL11A, HBS1L-MYB, and beta-globin lociassociate with fetal hemoglobin levels and pain crises in sicklecell disease. Proc Natl Acad Sci U S A. 2008;105(33):11869-11874.
24. Makani J, Menzel S, Nkya S, et al. Genetics of fetal hemoglobinin Tanzanian and British patients with sickle cell anemia.Blood. 2011;117(4):1390-1392.
25. Sheehan VA, Luo Z, Flanagan JM, et al. Genetic modifiers ofsickle cell anemia in the BABY HUG cohort: influence onlaboratory and clinical phenotypes. Am J Hematol. 2013;88(7):539-632
26. Fertrin KY, Costa FF. Genomic polymorphisms in sickle celldisease: implications for clinical diversity and treatment. ExpertRev Hematol. 2010;3(4):443-458.
27. Thein SL. Genetic modifiers of sickle cell disease. Hemoglobin.2011;35(5-6):589-606.
28. Debaun MR, Armstrong FD, McKinstry RC, Ware RE, Vichin-sky E, Kirkham FJ. Silent cerebral infarcts: a review on aprevalent and progressive cause of neurologic injury in sicklecell anemia. Blood. 2012;119(20):4587-4596.
29. Thangarajh M, Yang G, Fuchs D, et al. Magnetic resonanceangiography-defined intracranial vasculopathy is associatedwith silent cerebral infarcts and glucose-6-phosphate dehydro-genase mutation in children with sickle cell anaemia. Br JHaematol. 2012;159(3):352-359.
30. Flanagan JM, Frohlich DM, Howard TA, et al. Geneticpredictors for stroke in children with sickle cell anemia. Blood.2011;117(24):6681-6684.
31. Sebastiani P, Solovieff N, Hartley SW, et al. Genetic modifiersof the severity of sickle cell anemia identified through agenome-wide association study. Am J Hematol. 2010;85(1):29-35.
32. Milton JN, Rooks H, Drasar E, et al. Genetic determinants ofhaemolysis in sickle cell anaemia. Br J Haematol. 2013;161(2):270-278.
33. van der Harst P, Zhang W, Mateo Leach I, et al. Seventy-fivegenetic loci influencing the human red blood cell. Nature.2012;492(7429):369-375.
34. Thein SL. The molecular basis of beta-thalassemia. ColdSpring Harb Perspect Med. 2013;3(5):a011700.
35. Musallam KM, Sankaran VG, Cappellini MD, Duca L, NathanDG, Taher AT. Fetal hemoglobin levels and morbidity in
360 American Society of Hematology

untransfused patients with beta-thalassemia intermedia. Blood.2012;119(2):364-367.
36. So CC, Song YQ, Tsang ST, et al. The HBS1L-MYB intergenicregion on chromosome 6q23 is a quantitative trait locuscontrolling fetal haemoglobin level in carriers of beta-thalassaemia. J Med Genet. 2008;45(11):745-751.
37. Galanello R, Sanna S, Perseu L, et al. Amelioration ofSardinian beta-zero thalassemia by genetic modifiers. Blood.2009;114(18):3935-3937.
38. Nuinoon M, Makarasara W, Mushiroda T, et al. A genome-wide association identified the common genetic variants influ-ence disease severity in �0-thalassemia/hemoglobin E. HumGenet. 2010;127(3):303-314.
39. Badens C, Joly P, Agouti I, et al. Variants in genetic modifiersof beta-thalassemia can help to predict the major or intermediatype of the disease. Haematologica. 2011;96(11):1712-1714.
40. Weiss MJ, dos Santos CO. Chaperoning erythropoiesis. Blood.2009;113(10):2136-2144.
41. Bank A. Regulation of human fetal hemoglobin: new players,new complexities. Blood. 2006;107(2):435-443.
42. Borg J, Papadopoulos P, Georgitsi M, et al. Haploinsufficiencyfor the erythroid transcription factor KLF1 causes hereditarypersistence of fetal hemoglobin. Nat Genet. 2010;42(9):801-805.
43. Borg J, Patrinos GP, Felice AE, Philipsen S. Erythroid pheno-types associated with KLF1 mutations. Haematologica. 2011;96(5):635-638.
44. Sankaran VG, Menne TF, Xu J, et al. Human fetal hemoglobinexpression is regulated by the developmental stage-specificrepressor BCL11A. Science. 2008;322(5909):1839-1842.
45. Xu J, Sankaran VG, Ni M, et al. Transcriptional silencing of{gamma}-globin by BCL11A involves long-range interactionsand cooperation with SOX6. Genes Dev. 2010;24(8):783-798.
46. Zhou D, Liu K, Sun CW, Pawlik KM, Townes TM. KLF1regulates BCL11A expression and gamma- to beta-globin geneswitching. Nat Genet. 2010;42(9):742-744.
47. Siatecka M, Bieker JJ. The multifunctional role of EKLF/KLF1during erythropoiesis. Blood. 2011;118(8):2044-2054.
48. Wahlberg K, Jiang J, Rooks H, et al. The HBS1L-MYBintergenic interval associated with elevated HbF levels shows
characteristics of a distal regulatory region in erythroid cells.Blood. 2009;114(6):1254-1262.
49. Stadhouders R, Thongjuea S, Andrieu-Soler C, et al. Dynamiclong-range chromatin interactions control Myb proto-oncogenetranscription during erythroid development. EMBO J. 2012;31(4):986-999.
50. Suzuki M, Yamazaki H, Mukai HY, et al. Disruption of theHbs1l-Myb locus causes hereditary persistence of fetal hemo-globin in a mouse model. Mol Cell Biol. 2013;33(8):1687-1695.
51. Jiang J, Best S, Menzel S, et al. cMYB is involved in theregulation of fetal hemoglobin production in adults. Blood.2006;108(3):1077-1083.
52. Bianchi E, Zini R, Salati S, et al. c-Myb supports erythropoiesisthrough the transactivation of KLF1 and LMO2 expression.Blood. 2010;116(22):e99-110.
53. Bauer DE, Kamran SC, Orkin SH. Reawakening fetal hemoglo-bin: prospects for new therapies for the beta-globin disorders.Blood. 2012;120(15):2945-2953.
54. Zhao H, Kalota A, Jin S, Gewirtz AM. The c-myb proto-oncogene and microRNA-15a comprise an active autoregula-tory feedback loop in human hematopoietic cells. Blood.2009;113(3):505-516.
55. Sankaran VG, Menne TF, Scepanovic D, et al. MicroRNA-15aand -16-1 act via MYB to elevate fetal hemoglobin expressionin human trisomy 13. Proc Natl Acad Sci U S A. 2011;108(4):1519-1524.
56. Xu J, Peng C, Sankaran VG, et al. Correction of sickle celldisease in adult mice by interference with fetal hemoglobinsilencing. Science. 2011;334(6058):993-996.
57. Shi L, Cui S, Engel JD, Tanabe O. Lysine-specific demethylase1 is a therapeutic target for fetal hemoglobin induction. NatMed. 2013;19(3):291-294.
58. Danjou F, Anni F, Perseu L, et al. Genetic modifiers ofbeta-thalassemia and clinical severity as assessed by age at firsttransfusion. Haematologica. 2012;97(7):989-993.
59. Milton JN, Sebastiani P, Baldwin CT, et al. Prediction of fetalhemoglobin in sickle cell anemia using a genetic risk score[abstract]. Blood (ASH Annual Meeting Abstracts). 2012;120(21):3216.
60. Drmanac R. Medicine: the ultimate genetic test. Science.2012;336(6085):1110-1112.
Hematology 2013 361