Embed Size (px)
DESCRIPTION
Citation preview

Goodbye Suxamethonium!
C. Lee
Emeritus Professor, Department of Anesthesiology, Harbor-UCLA Medical Center, Torrance, CA, USA
SummaryNo drugs in anaesthesia are more problematic than suxamethonium. Yet, no drugs have survived assuxamethonium does in spite of crisis after crisis, and attempt after attempt at its replacement. Fordecades, suxamethonium has taught us neuromuscular pharmacology and provided us with anencyclopaedia of side effects, while benefiting millions and millions of our anaesthetised patients.With the arrival of sugammadex, it finally appears that suxamethonium can be retired. Suxamet-honium has done its job and seen its days! The present review is intended to offer a eulogy forsuxamethonium.
........................................................................................................
Correspondence to: Dr Chingmuh LeeE-mail: [email protected]
Accepted: 15 December 2008
After decades of effort by many investigators around theworld to replace suxamethonium, and years after theslogan ‘So Long, Sux!’ was first coined with the clinicalintroduction of atracurium, it now appears that suxame-thonium is finally on its way out. It has seen its days. As oneof many investigators who has spent years searching for anon-depolarising replacement for suxamethonium, thisauthor proposes for eulogy to suxamethonium. No drug inanaesthesia is more problematic than suxamethonium andyet no drug has survived crisis after crisis as suxametho-nium has. Suxamethonium is indeed an amazing drug.
Preclinical history of suxamethonium
Suxamethonium had a remarkable history from the verybeginning. Along with other choline-related compounds,it was first tested as a cardiovascular agent in 1906. Huntand Taveau [1] observed that suxamethonium slowed theheart and increased the blood pressure. As the experi-ments were done on animals already paralysed withcurare, the neuromuscular effects of suxamethoniumwere not noticed until 1949 by Bovet [2] almost half acentury later. In other words, suxamethonium began witha side effect.
Clinical introduction of suxamethonium
Suxamethonium was introduced into clinical anaesthesiain Europe in 1951 by Br}uke et al. and in the UnitedStates in 1952 by Foldes et al., then of Pittsburgh [3, 4].The Foldes report, a classic, reported 202 consecutive
patients undergoing intra-abdominal procedures. Sux-amethonium was given both by bolus and by infusion,with doses of 66–1830 mg given over 35–363 min.After premedication with pentobarbital, atropine orscopolamine and morphine, anaesthesia was provided bythiopental and nitrous oxide. Lung ventilation was mostlyspontaneous. Foldes et al. wrote: ‘Assisted respiration wasseldom necessary, and respiratory arrest never developed,except when produced deliberately’. Readers might findit interesting that in those days tracheal intubation wasrare, oxygen and carbon dioxide monitors were absent,and anaesthesia and surgery were very different fromtoday. The results with suxamethonium were considered‘close to ideal’, ‘without unwanted side effects’, ‘with lowpostoperative complication rate’, and ‘much superior’ tocurare preparations. Also in those days, postoperativepulmonary complications were common, but none wasattributed to the use of suxamethonium.Foldes et al. further stated that: ‘the advantages of
suxamethonium as a muscular relaxant in anesthesiologyfar outweighed its disadvantages’ [3, 4]. ‘On the basis ofour experience, suxamethonium is the muscle relaxant ofchoice, especially in debilitated, dehydrated and agedpatients, in whom prolonged postoperative respiratorydepression with other agents is most common’. ‘It ishoped that the clinical use of suxamethonium willstimulate the search for other agents – for example,barbiturates – with ultrashort activity’. Points well made!Suxamethonium’s flexibility of use was emphasised.Interestingly, an addendum to the paper on suxame-
thonium stated: ‘Since this paper was submitted for
Anaesthesia, 2009, 64 (Suppl. 1), pages 73–81.....................................................................................................................................................................................................................
! 2009 The AuthorJournal compilation ! 2009 The Association of Anaesthetists of Great Britain and Ireland 73

publication several cases of prolonged respiratory depres-sion after the use of suxamethonium have been reported.As pointed out elsewhere, unnecessarily high doses ofsuxamethonium were used in these cases. It has also beenshown that the depressant effect of a given dose ofsuxamethonium on respiration is inversely proportional tothe plasma cholinesterase activity of the patients. Accord-ing to our experience in over 500 cases… no prolongedrespiratory depression was observed’ [3, 4]. It appears thatanaesthetic masters of those days practised titrationaccording to a patient’s individual responses and theneeds of surgery. Without nerve stimulators, theywatched the patient’s chest and abdomen, as well as thebreathing bag and the surgical field.
Current uses of suxamethonium
After its introduction, suxamethonium gained greatpopularity. In the year 1980–1981, sales of suxametho-nium in the US peaked at 2233 kg [4]. With increaseduse, more side effects were observed. Many of these sideeffects were previously unheard of. Some were associatedwith significant mortality. Each issue, such as malignanthyperthermia, atypical plasma cholinesterases and Phase IIblock generated great controversy and stimulated impor-tant research. Amazingly, as pointed out by Lee [4, 5], adrug capable of generating so many controversies andsurviving so many crises just would not die. Lee [5] alsonoted in 1994 that anything that could go wrong hadgone wrong, yet suxamethonium still maintains importantuses in clinical anaesthesia, even today in its sixth decadeof use. It survives on a few advantages – rapid onset, rapidrecovery, non-toxic metabolites and economy of use. Inits niche, suxamethonium is still the gold standard againstwhich other neuromuscular block techniques are com-pared. For example, rocuronium is said to provide equallygood intubation conditions and TAAC3 claims fasteronset and shorter duration of action than suxamethonium[6, 7]. At the time of writing, suxamethonium againserves as the gold standard against which sugammadexreversal of rocuronium is compared for rapid recovery.The indications for suxamethonium appear to have
stabilised in the last decade or two [5]. Among the fewremaining indications for suxamethonium, the major oneis to facilitate rapid sequence tracheal intubation in theoperating room and in the emergency department, mainlyfor fear of pulmonary aspiration of stomach contentsduring intubation. The other indication is when difficultintubation is a concern (without full stomach) butcircumstances warrant an attempt at intubating thetrachea facilitated by anaesthesia and paralysis, as analternative to awake intubation. An equivocal indicationis to facilitate routine intubation in surgical patients. In
the first two indications, failure to intubate and failure toventilate the lungs could be disastrous, and a rapid returnof muscle power becomes crucial. In the last indication,an occasional encounter with an unsuspected difficultairway may make suxamethonium a hero if it allows thepatient to regain the capacity to breathe spontaneouslybefore hypoxaemia intervenes. Suxamethonium as asingle dose is also useful for fracture setting, cardioversion,electroconvulsive therapy and other procedures requiringparalysis of very short duration. In otorhinolaryngologicalprocedures, complete paralysis may be required forforeign body removal and other brief endoscopic proce-dures. Here, the need for profound paralysis may lastthrough the case, only to end abruptly, thereby makingreversal of a deep non-depolarising block difficult.Further, once suxamethonium is chosen, a brief infusionmay come in handy if one dose is not sufficient.
Mechanisms of actions of suxamethonium
Foldes et al. [3] recognised and attributed the transienttwitching upon injection of suxamethonium to the initialstimulating effect of depolarising drugs on skeletal muscle.No myalgia was mentioned. Neuromuscular block bydepolarisation of muscle cells is, in a sense, like generalanaesthesia by depolarisation of cerebral neurons. It isintuitively a bad idea. Electroconvulsive therapy for majordepression produces a transient unconsciousness and yetelectro-anaesthesia, which was tried in the former SovietUnion, has not gained popularity. Fortunately, the neuro-muscular endplates and muscle cells repolarise themselvesin seconds or minutes to maintain cellular homeostasis.Suxamethonium is structurally two acetylcholine mol-
ecules joined end-on-end on the acetyl side to make asuccinyl di-ester of choline, i.e. succinyldicholine, henceits name succinylcholine elsewhere in the world. Itstherapeutic actions and side effects are attributed to itsacetylcholine moieties. Its metabolites are succinylmo-nocholine and choline. Succinylmonocholine has aboutone-sixth to one-tenth the potency of suxamethonium.Choline exists in the body as a normal metabolite.Suxamethonium used to be considered a bis-quaternary
neuromuscular blocking agent, and historically it wasthought that two quaternary -onium heads are requiredfor any compound to be a potent neuromuscular blocker.Succinylmonocholine is thought to be weak because it ismonoquaternary. However, the notion that monoqua-ternary compounds will not make potent neuromuscularblockers was overturned by the realisation that vecuro-nium is monoquaternary [8].During the onset of neuromuscular block, suxametho-
nium produces fasciculation, which results from depolar-isation [3]. To be precise, fasciculation is due to an agonist
C. Lee Æ Goodbye suxamethonium! Anaesthesia, 2009, 64 (Suppl. 1), pages 73–81......................................................................................................................................................................................................................
! 2009 The Author74 Journal compilation ! 2009 The Association of Anaesthetists of Great Britain and Ireland

action on the motor nerve terminal, a prejunctional actionthat propagates retrogradely up the motor axon to triggerthe axon into firing the entire motor unit. Activation ofindividual muscle fibres will only cause fibrillation, notfasciculation. Activation of a motor neuron excites thewhole motor unit to cause fasciculation. A small dose ofcurare-like, non-depolarising neuromuscular blockingdrug (NMB) is often used to prevent or decrease thefasciculation, mainly to decrease the increase in gastricpressure during fasciculation. While acting as defasciculantprejunctionally, the defasciculating drug also decreases thepotency of suxamethonium postjunctionally. Prejunction-al and postjunctional nicotinic receptors are different intheir functions, and depolarising and non-depolarisingNMBs interact at both places with different pharmacody-namics [9].
The conformational mechanism of action ofsuxamethonium
Marshall et al. [10] reported in 1990 that it takes twomolecules of suxamethonium, as it takes two molecules ofacetylcholine, to open one nicotinic channel. In otherwords, each half-molecule of suxamethonium acts likeone acetylcholine, and each molecule of suxamethoniumuses only one of its two half-molecules at a time [10, 11].This contradicts the traditional belief that suxamethoniumworks like decamethonium, with a bisquaternary mech-anism of action.The monoquaternary mechanism of action of suxame-
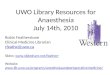
thonium is interesting from the viewpoint of modernreceptor theory and molecular conformation–actionrelationship [11]. First, vecuronium proves that mono-quaternary muscle relaxants could be better than theirbisquaternary analogues [8]. Then, basic thermodynamiccalculations show that suxamethonium cannot exist as astraight molecule [11]. The negatively charged oxygenatoms are strongly attracted to the positively chargedammonium heads, and the energy penalty in existing as astraight molecule is too high. In other words, suxame-thonium is too short to reach both receptive sitessimultaneously [11] (Fig. 1). In contrast, decamethoniumis a straight molecule, and it reaches both receptive siteswith its twin methonium heads.Several questions followed. Firstly, if only one acetyl-
choline moiety is binding the receptor site, what does theother moiety contribute to the action of suxamethonium?Secondly, why is suxamethonium not totally like acetyl-choline in pharmacology? Thirdly, if succinylmonocholinehas the same acetylcholinemoiety in themolecule, why is itnot as potent a neuromuscular blocker as suxamethonium?Lee [11] recently proposed a general mechanism of
action of the NMBs based on their molecular conforma-
tion. As a molecule constantly vibrates around eachrotatable bond to seek the lowest possible total energy, itpreferentially populates the lowest energy conformations.According to organic chemistry, molecular shape deter-mines molecular action. Rigid molecules change shapewith difficulty and tend to concentrate on a few lowest-energy conformations. A rigid compound therefore tendsto either work very well or not at all, depending onwhether its most populated conformer fits the targetreceptive site. If it works, it has high potency and few sideeffects. A flexible compound by contrast tends to assumenumerous conformations liberally, allowing it to fitseveral receptors, including receptors mediating sideeffects. Lacking conformational concentration, it tendsto have low potency. For example, vecuronium is a rigidmolecule, and its D-ring acetylcholine moiety fits thereceptive site of the endplate receptor with greatprecision, giving it potency and specificity. By contrast,suxamethonium has a flexible molecule, allowing it towork on several cholinergic receptors with numerous sideeffects. Nevertheless, suxamethonium has sufficient con-formational preference for the skeletal muscle endplate
Figure 1 Molecular conformation and mechanism of action ofsuxamethonium (SDC) and succinylmonocholine. Suxametho-nium exists in bent form, too short to bind both receptive sites ofthe nicotinic receptor simultaneously. Whereas each ACh-moiety of suxamethonium has its functional groups (N, O)configured to conform to a receptive site of the nicotinicreceptor, no such conformation is possible for the solo ACh-moiety of succinylmonocholine. In suxamethonium, the ACh-moieties are balanced by the mutually repelling force of themethonium heads, which permits each ACh-moiety to maintaina nicotinic configuration. In succinylmonocholine, all O atomsare attracted towards the lone -onium head, preventing the ACh-moiety from assuming a nicotinic configuration. Arrows indicatethe distance from the center of the N atoms to the van der Waalsextensions (dotted red spheres) of the respective O atoms, whichdetermine whether an ACh-moiety will have nicotinic activity[11, 12]. Atoms are colour-coded: O, red; N, blue; C, white;H, green. (Reproduced from reference [11], with permission).
Anaesthesia, 2009, 64 (Suppl. 1), pages 73–81 C. Lee Æ Goodbye suxamethonium!......................................................................................................................................................................................................................
! 2009 The AuthorJournal compilation ! 2009 The Association of Anaesthetists of Great Britain and Ireland 75

receptor to be a useful neuromuscular rather thancardiovascular or other cholinergic drug. Because of theinteraction among its functional groups – the methoniumgroups, the carbonyl oxygen atoms and the ester oxygenatoms – the molecule assumes a peculiar bent conforma-tion and the acetylcholine moieties assume a conforma-tion suitable for nicotinic action but not muscarinic action[11, 12]. The above explains not only why it takes twomolecules of suxamethonium to open one receptorchannel but also why suxamethonium is more nicotinicthan muscarinic. The question then becomes: why doessuccinylmonocholine not work equally well as a NMB?The answer is that without balance from the secondmethonium head, the lone acetylcholine moiety ofsuccinylmonocholine conforms poorly to the receptivesite, nicotinic or muscarinic [11, 12]. In summary, theinteraction between the two acetylcholine moietiesrender suxamethonium a monoquaternary neuromuscularblocking agent, although it is a bisquaternary chemicalcompound.
Breakdown of suxamethonium
Suxamethonium is hydrolysed by plasma cholinesterase.Patients with hepatic dysfunction have deficient plasmacholinesterase, while patients taking the eye drop echo-thiophate may have inactivated plasma cholinesterase.They exhibit prolonged neuromuscular block fromsuxamethonium. Echothiophate inhibition of plasmacholinesterase is irreversible, and recovery of the enzy-matic action depends on generation of new enzymes.Plasma cholinesterase has several variants [13]. The
atypical enzymes can be identified by their resistance tofluoride, dibucaine and other laboratory agents [13].While the normal enzyme hydrolyses suxamethoniumeffectively, its ability to hydrolyse butyrylcholine ismarkedly inhibited by dibucaine – by up to 80%, inwhich case the dibucaine number is said to be 80. Bycontrast, a homozygous atypical enzyme does nothydrolyse suxamethonium effectively, but its ability tohydrolyse butyrylcholine may be resistant to dibucaine. Ifit is inhibited by only 20%, the dibucaine number is saidto be 20. A heterozygote will have a dibucaine number of40–60. Besides dibucaine or fluoride-resistant atypicalplasma cholinesterases, there are silent genes and othervariants. Interestingly, hyperactive – as opposed tohypoactive – plasma cholinesterase also exists, althoughit is rare [5].Following a typical intubation dose of suxamethonium
(1 mg.kg)1), a patient with normal plasma cholinesterasewill be paralysed for 5–11 min, of which 3–7 min may becomplete block. A heterozygous enzyme could result in aneuromuscular block with a duration of 10–30 min. An
atypical homozygote will be paralysed for 40–200 min, ofwhich 30–90 min could be complete block, and theblock will manifest Phase II block characteristics [14].Blood transfusion or administration of plasma cholin-
esterase concentrates will terminate suxamethonium-induced prolonged paralysis in patients unable tohydrolyse suxamethonium. In fact, most of the injectedsuxamethonium (80%) is normally hydrolysed in plasmabefore reaching the neuromuscular junction. It has alsobeen shown that 10% the normal dose of suxamethoniumwill produce a paralysis of nearly normal duration inpatients with homozygous atypical plasma cholinesterase.
Side effects of suxamethonium
Twinning of two acetylcholine molecules to makesuxamethonium thinly veils the true nature of suxame-thonium.What is surprising is not that suxamethonium hasso many acetylcholine-related side effects, but thatsuxamethonium is still selective enough to be a NMB.This can be explained by its molecular conformation, asdescribed above [11]. Still, suxamethonium has so manyside effects that even their classification can prove contro-versial. Lee [4, 5] classified these side effects according tomechanism of action as: depolarisation of the endplate andmuscle; agonistic actions at other nicotinic sites; musca-rinic effects; abnormal breakdown; idiosyncratic actions;drug interactions; changing nature of block after prolongeduse. Some of these are highlighted below.Myalgia after suxamethonium is a common occur-
rence. However, the precise incidence, severity andmechanism of pain are very variable. Lying on theoperating table alone is often enough to cause aches andpains. Typical suxamethonium myalgia is deep aching inall muscles. The large number of proposed remediesmeans that none works well. These include non-steroidalanti-inflammatory drugs, vitamins, physiotherapy,stretching exercises, defasciculation, phenytoin, self-tam-ing (pre-treatment with a small dose of suxamethoniumitself) and others [5]. The most susceptible patient is theyoung adult female.Fasciculation, if vigorous, may look cruel to observers.
One cannot but link vigorous fasciculation to myalgia,but an exact causal and quantitative relationship is simplynot there. Anaesthetists do not even agree on thenecessity or benefit of defasciculation. Some use fascic-ulation to tell that the neuromuscular block has started towork. For patients with full stomach, fasciculation mayincrease gastric pressure and result in regurgitation. Forrapid sequence intubation, many anaesthetists woulddefasciculate with a small dose of non-depolarisingNMB. In frail, older patients, some fear that a forcefulfasciculation might fracture a bone. Foldes et al. [3]
C. Lee Æ Goodbye suxamethonium! Anaesthesia, 2009, 64 (Suppl. 1), pages 73–81......................................................................................................................................................................................................................
! 2009 The Author76 Journal compilation ! 2009 The Association of Anaesthetists of Great Britain and Ireland

observed that a slower injection of suxamethonium elicitsless fasciculation. However, slow injection is not suitablefor rapid sequence intubation.Avian and lower animals respond to suxamethonium
and other depolarising neuromuscular blockers with aspastic paralysis [15]. A bird paralysed by suxamethoniumor decamethonium is a stiff bird. Mammalian extra-ocularmuscles respond similarly [16]. Whereas a tetanic con-traction is a fusion of twitches with transmitted electro-myographic pulses, suxamethonium-induced contractureis a form of paralysis, with no electrophysiologicalevidence of neuromuscular transmission.Contracture of the extra-ocular muscles is another
controversial issue. The controversy is not about itsoccurrence, but in its consequence in patients with anopen globe injury. Normally, the contracture increasesintraocular pressure. However, the greatest increase inintraocular pressure appears to result from light anaesthe-sia, with its associated relative hypertension in response totracheal intubation, not from extra-ocular muscle con-traction. A far greater increase in intra-ocular pressurewould be created by a vigorous cough and straining on thetracheal tube. If the globe is open, the contraction mayexpel some eye content. For rapid sequence intubation inthe presence of open globe injury, both rocuronium andsuxamethonium are acceptable drugs but if suxamethoni-um is selected, it might be advisable to defasciculate. Witheither drug, it is wise to induce sufficiently deep anaes-thesia and paralysis before tracheal intubation. Theavailability of sugammadex for the rapid reversal ofrocuronium may tip the choice of NMB further awayfrom suxamethonium and towards rocuronium [17].Some patients have spasm of the jaw in response to
suxamethonium. Masseter spasm can be an early sign or amild form of malignant hyperthermia. It can become anobstacle to tracheal intubation. Studies have shown that toa variable degree – usually minor – all humans respond tosuxamethonium with increased jaw tension. While someinvestigators have recommended muscle biopsy for allpatients who exhibit marked masseter spasm, mostanaesthetists exercise discretion, depending on theirclinical assessment. The mortality and morbidity ofmalignant hyperthermia have been decreased by advancesin recognition and treatment, while a diagnostic musclebiopsy in itself is quite invasive and the biopsy result doesnot always offer clear-cut benefit. Avoidance of suxame-thonium would be the safest alternative.When first recognised, a fulminant case of malignant
hyperthermia carried a mortality of about 80%. Treatedwith dantrolene, the mortality today should be < 10%.The onset of malignant hyperthermia varies. Aftersuxamethonium, it may ensue immediately. After theuse of inhalational agents, it can manifest in a few
minutes, or even as late as in the recovery room or on thefirst postoperative day. A fulminant malignant hyperther-mia attack often manifests as generalised rigidity, difficultlung ventilation, hypermetabolism and high fever of rapidonset. In patients with malignant hyperthermia trait ormuscle diseases such as Duchene muscular dystrophy,suxamethonium may cause cardiac arrhythmia and cardiacarrest by direct agonistic action on the heart.A small increase in plasma potassium, in the order of
0.1–0.5 mmol.l)1, usually follows suxamethoniumadministration. Most anaesthetists avoid suxamethoniumin patients with borderline or marked hyperkalaemia,such as in those with renal failure. In patients with a majorburn injury, severe trauma, major nerve injury, paraple-gia, severe metabolic acidosis and other critical condi-tions, plasma potassium may increase markedly aftersuxamethonium. Fatal cardiac arrest may ensue even if theplasma potassium concentration before the administrationof suxamethonium is normal. The danger starts at about12–24 h after a major burn. In burns and in paraplegia,the danger of hyperkalaemia will last as long as inflam-mation and the degeneration and regeneration processesof the dystrophic muscle cells persist. Defasciculation doesnot protect patients from hyperkalaemia.Suxamethonium is an agonist at the heart and the
ganglia, including the adrenal glands. By direct or reflexvagal action, suxamethonium not uncommonly causesbradycardia or transient (10–30 s) cardiac arrest, especiallyin children and especially upon the administration of asecond dose of suxamethonium [18]. Anaesthetists ofteninject atropine before the second dose of suxamethoniumto prevent bradycardia. Children are often given atropineprophylaxis with or before the first dose of suxametho-nium. However, more often than not, suxamethonium(especially in a large dose) causes tachycardia andhypertension, which may follow an initial bradycardia.
Phase II block
Shortly after Ali introduced the train-of-four (TOF),Savarese et al. [14] and Lee independently observedmarked TOF fade in patients with atypical plasmacholinesterase who were given suxamethonium. Lee[4, 5] subsequently applied TOF stimulation to normalsubjects receiving suxamethonium and developed criteriathat set Phase II block in quantifiable terms (Fig. 2).The recognition of Phase II block predated the TOF by
some time [19–21]. Using isolated rabbit lumbricalmuscle under constant exposure to decamethonium invitro, Jenden et al. [20] described an initial profoundblock, a transitional partial spontaneous recovery (tachy-phylaxis), and a second profound block of the twitchresponse. In surgical patients treated with a continuous
Anaesthesia, 2009, 64 (Suppl. 1), pages 73–81 C. Lee Æ Goodbye suxamethonium!......................................................................................................................................................................................................................
! 2009 The AuthorJournal compilation ! 2009 The Association of Anaesthetists of Great Britain and Ireland 77

infusion of suxamethonium – a practice once popular –clinical anaetshetists long observed an initial phase ofblock characterised by fasciculation, non-fading tetanus,blurred post-tetanic facilitation and potentiation of theblock by cholinesterase inhibitors [4, 5, 19]. A transitionalphase is characterised by tachyphylaxis, necessitating agreater and greater infusion rate to maintain the samerelaxation. By the time the patient becomes well paralysedagain, the block has become slow to recover, and ischaracterised instead by tetanic fade, marked post-tetanicfacilitation, variable reversibility by cholinesterase inhib-itors, and without fasciculation upon injection of addi-tional bolus dose of suxamethonium. The patientbecomes extremely sensitive to even small doses ofcurariform drugs. Most troublesome is the slow sponta-neous recovery that cannot be satisfactorily accelerated byreversal. Attempts at reversal of the block often result injust enough muscle power to make lung ventilationdifficult but not enough to sustain a patent airway andadequate spontaneous breathing. Using TOF stimulation,Lee [4, 5] described two periods of profound neuromus-cular block interposed by tachyphylaxis in humans beinggiven a continuous infusion of suxamethonium, echoingthe very original observation of Phase II block by Jendenet al. [20].As is usual with suxamethonium, even the start of Phase
II block is controversial and confusing, because even in
Phase I minor TOF fade exists. This minor fade, typicallylabelled as ‘minimal fade’, lacks clinical significance [4, 5,22–24]. During the short time course of a single dose ofsuxamethonium 1 mg.kg)1, from which the twitchquickly recovers, the TOF ratio will initially read zero,but soon becomes 0.8, and then 1.0. Obviously, anyminor fade will make the TOF ratio initially zero. This isnot a mild Phase II block. By definition, linear changes donot make phases. Phase II block is differentiated fromPhase I by tachyphylaxis, receptor changes and contrast-ing clinical pictures [4, 5, 18–20].To make the TOF clinically relevant, the TOF ratio
should be measured at a point when the first twitch hasrecovered to 30–50% of control, ideally to 50% [4, 5, 24].Simply put, the first twitch is a major independentdeterminant of the TOF ratio with suxamethonium as it iswith a non-depolarising block. If measured in thestandardised manner, the TOF ratio clearly shows twophases: a Phase I of slight fade and a Phase II of markedfade, separated by a transitional phase in which tachy-phylaxis can be observed [4, 5]. When the standardisedTOF ratio is very low, such as 0.2–0.3, the block alwaysmanifests marked tetanic fade, facilitated post-tetanictwitch and slowed recovery. A standardised TOF ratioalso predicts reversibility with edrophonium. While aTOF ratio > 0.6 predicts block enhancement, a TOFratio < 0.4 predicts reversal – the greater the fade, thegreater the reversibility [25]. The reversal is seldomcomplete because inhibition of tissue cholinesterase doesnot normalise the desensitised receptors.The mechanism of Phase II block is not completely
understood. Desensitisation of the endplate receptors toacetylcholine, a postjunctional phenomenon, accounts forthe protracted residual paralysis. This also accounts for theexquisite sensitivity of patients to curariform drugs, asthere exists a diminished number of normal receptorsremaining to block. However, as in a curariform block,the fade (TOF and tetanic) is most likely a prejunctionalphenomenon [9]. Blockage of the prejunctional feedbackreceptors impairs the mobilisation of the transmitter tothe immediately releasable site. During neuromuscularblock, a 50% block of the twitch means most musclefibres are at threshold, 50% responding fully and 50% notat all. A minor decrease in transmitter output in responseto successive nerve impulses will make a significantdifference in the number of muscle cells responding,thereby causing fade. It is likely that tetanic fade and post-tetanic facilitation in Phase II are also prejunctional, asthey are in curariform block.Phase II block has been called different names. As few
users of suxamethonium would doubt the existence oftwo different blocks, this author prefers to just call itPhase II block to echo the original observation made by
Figure 2 Diagram of changing characteristics of neuromuscularblock in humans observed during continuous infusion of sux-amethonium. In Phase I, the train-of-four fades minimally, andedrophonium will deepen the block. During transition, tachy-phylaxis occurs and the twitches show partial recovery despiteconstant infusion of the relaxant. The train-of-four ratio andeffect of edrophonium also exhibit transition. In Phase II, thetrain-of-four fades markedly, the block becomes increasinglyreversible by edrophonium although the reversal is rarelycomplete, and the block deepens and becomes slow to recover.The curve depicting the twitch height is reminiscent of theoriginal observation in vitro [20], with similar time course andmagnitude. (Reproduced from reference [5] with permission).
C. Lee Æ Goodbye suxamethonium! Anaesthesia, 2009, 64 (Suppl. 1), pages 73–81......................................................................................................................................................................................................................
! 2009 The Author78 Journal compilation ! 2009 The Association of Anaesthetists of Great Britain and Ireland

Jenden et al. [20] in 1954. Other terms include desen-sitisation block, dual block, and non-depolarising block.The term ‘desensitisation block’ is vague, because inPhase II the endplate is desensitised to acetylcholine, thetwitch is resistant to suxamethonium but sensitive to itsresidual effect, while the patient is very sensitive tocurariform drugs.Self-antagonism is an interesting phenomenon in Phase
II block. It is intrinsic to the agonistic, anti-curare natureof suxamethonium, and it explains tachyphylaxis [26]. Towhit, a fresh bolus of a small quantity of suxamethonium(0.05–0.1 mg.kg)1) will antagonise its own Phase IIblock, as it does curariform block. The twitch and theTOF ratio will both increase. A larger dose of suxame-thonium (0.2–0.5 mg.kg)1) will first briefly antagonisethe block before adding to the block. The resultant blockthen becomes protracted and typical of Phase II (Fig. 3).The phenomenon explains the clinical observation in the1960s that upon continuous infusion suxamethoniumbecomes ineffective, but upon further use the patientbecomes weak for a long time afterwards.The few remaining indications for suxamethonium
include brief infusion for short procedures. As a generalguide, up to 2–4 mg.kg)1 of suxamethonium adminis-tered over 30–40 min does not result in much prolongedresidual block in patients with normal plasma cholines-terase [4, 5, 27].
Efforts to replace suxamethonium
Among the proposed criteria for an ideal NMB are:efficacy, safety and economy of use. Efficacy implies fastonset, high potency and controllable level of block. Safetyimplies a lack of undesirable actions by the drug or itsmetabolites, and ease of termination of the block.Economy of use depends on dose requirement, cost ofsynthesis, supply, storage, shelf life and resupply. Whileseveral NMBs fulfil most of the criteria, none so far – noteven suxamethonium – is fast and short-acting enough tobe ideal, especially considering the risk of hypoxia in thecase of difficult lung ventilation and tracheal intubation[28]. The ideal NMB was once dubbed ‘non-depolarisingsuxamethonium’ because, so far, it is easier to use a5-min drug for 1-h surgery than to reverse a 1-h drug in5 min.The ‘non-depolarising suxamethonium’ has been
elusive. Nevertheless, searches have resulted in theintroduction of several good NMBs over the decades.Among these, doxacurium, pipecuronium, metocurineand pancuronium are long-acting; vecuronium, atracu-rium, and cisatracurium are intermediate ⁄ long-acting;rocuronium is intermediate-acting; mivacurium andrapacuronium are short-acting. Under the principle ofsurvival of the fittest, rocuronium, vecuronium andcisatracurium remain popular today. Because suxame-
Figure 3 Self-antagonism and prolonged residual block (dual action) in a typical case of well-established Phase II block after infusionof 7.3 mg.kg)1 of suxamethonium. Marked train-of-four fade was evident. Starting with an existing slow-recovering residual block,an additional bolus dose of suxamethonium 0.05 mg.kg)1, (a) only antagonised its own residual block. A dose of 0.1 mg.kg)1, (b)showed greater self-antagonism. A dose of 0.15 mg.kg)1, (c) first antagonised and then deepened the block. A dose of 0.2 mg.kg)1,(d) nearly increased the train-of-four ratio to 0.8, before it markedly depressed the ratio and the twitch. These doses of suxame-thonium are known to also antagonise a curariform non-depolarising block, to a similar extent. Instead of bolus, infusion ofsuxamethonium would blur the initial antagonism-potentiation sequence, and initially manifest only as inability to deepen the block,namely tachyphylaxis. The subsequent deepening of the slow-recovering residual block depicts a classic ‘desensitisation block’implying that the receptors are insensitive to the neurotransmitter acetylcholine [19, 27]. (Reproduced from reference [26], withpermission).
Anaesthesia, 2009, 64 (Suppl. 1), pages 73–81 C. Lee Æ Goodbye suxamethonium!......................................................................................................................................................................................................................
! 2009 The AuthorJournal compilation ! 2009 The Association of Anaesthetists of Great Britain and Ireland 79

thonium survives into its sixth decade by being thefastest in onset and shortest in duration of action, andbecause rocuronium has matched suxamethonium inproviding good tracheal intubation conditions within1 min [6], all it still takes to retire suxamethonium israpid reversal.The drug TAAC3 is a bis-tropinyl long-chain di-ester
neuromuscular blocking compound that successfullyunderwent thorough pre-human tests in various animalspecies and preparations. Pure stereo-isomers were syn-thesised. It is the only NMB shorter-acting and with afaster onset than suxamethonium, with a benign sideeffect profile, and it is non-cumulative [7]. Unfortunately,renal toxicity derailed the pursuit of perfection (personalinformation).Of the asymmetric fumarate tetrahydroisoquinolinium
derivatives, GW280430A [29] and its reformulatedproduct, and the new halogenated and un-halogenatedproducts AV002 and congeners, are promising and stillbeing pursued. Some are short-acting; some are interme-diate. Some of these compounds have good pharmaco-logical profiles and are broken down rapidly by cysteineabduction. Some new AV compounds are immediatelyreversible by intravenous administration of cysteine orglutathione in animals in a manner comparable to thereversal of rocuronium by sugammadex. Their reversal‘drugs’ are normal amino acids in the body, and thereforesafe.
A new challenge to suxamethonium
In a direct challenge to suxamethonium, Lee et al. [17]recently compared sugammadex reversal of profoundrocuronium-induced neuromuscular block with sponta-neous recovery from suxamethonium. In this randomised,multicentre study of 110 patients from 11 North Amer-ican medical centres, half the patients received 1 mg.kg)1
of suxamethonium followed by spontaneous recovery;the other half received rocuronium 1.2 mg.kg)1 followedby sugammadex 16 mg.kg)1 3 min later. Both groupsunderwent intravenous anaesthesia, and their tracheaswere intubated 1 min after the start of administration ofthe NMBs.Results showed effective and safe reversal of rocuro-
nium. Intubating conditions were excellent in bothgroups. Mean times to recovery of the first twitch ofthe TOF (T1) to 10% and to 90% were significantlyshorter in the rocuronium–sugammadex group (4.4 minand 6.2 min respectively) compared with the suxame-thonium group (7.1 min and 10.9 min respectively, allp < 0.001). If timed from sugammadex administration,the mean times to recovery were: T1 to 10% = 1.2 min;T1 to 90% = 2.9 min; TOF ratio to 0.9 = 2.2 min.
Recurrence of block did not occur, and both treatmentswere well tolerated.The 1.2 mg.kg)1 dose is the largest approved dose of
rocuronium, and is rarely needed clinically. In practice,0.6 mg.kg)1 is more commonly used. Likewise,16 mg.kg)1 of sugammadex is the largest dose so fartested in human patients. Many other clinical studies haveshown that sugammadex can safely and effectively reverseall degrees of neuromuscular block produced by rocuro-nium and vecuronium in a number of patient popula-tions. In this study, sugammadex was injected 3 min afterrocuronium to mimic a clinical scenario of failed trachealintubation after two attempts. Theoretically, sugammadexcan be administered at any time as clinically indicated,with similar efficacy. In the scenario, the speed andefficacy of reversal is critical because in apnoea susceptiblepatients may begin to desaturate within 3 min even if pre-oxygenated, and then may worsen rapidly by the second[28]. Without pre-oxygenation, the margin of safety isnarrower.
So long, sux! and thanks!
It now appears that suxamethonium can be replaced evenfor its final remaining indications. Thinking inside thebox, i.e. the neuromuscular junction with its anatomy,physiology, enzymology and pharmacology, decades ofresearch have failed to create a single drug to replacesuxamethonium. Thinking outside the box, sugammadex,which is entirely non-neuromuscular, promises not onlyto revolutionise the reversal of neuromuscular block butalso to retire the cholinesterase inhibitors as well assuxamethonium.Suxamethonium has created great controversies and
survived countless attacks while benefiting millions andmillions of patients for decades. It has amply taught usneuromuscular pharmacology, given us an encyclopaediaof side effects, and forced us to learn organic andcomputer chemistry, amongst other things. Suxametho-nium has done its job!
Conflicts of interest
The author has in the past received supports for hisneuromuscular pharmacology research from varioussponsors including Organon, USA, Inc., now a part ofSchering-Plough Corporation, owner of sugammadex.He is coprincipal investigator and co-inventor of theTAAC3 series of compounds (now de-activated) cited inthe text [7], which was in the past sponsored in part byOrganon. At present, he is principal investigator of amulti-centre study on sugammadex [17], also sponsoredby Organon.
C. Lee Æ Goodbye suxamethonium! Anaesthesia, 2009, 64 (Suppl. 1), pages 73–81......................................................................................................................................................................................................................
! 2009 The Author80 Journal compilation ! 2009 The Association of Anaesthetists of Great Britain and Ireland

References
1 Hunt R, de M Taveau R. On the physiological action of
certain choline derivatives and new methods for detectingcholine. British Medical Journal 1906; 2: 1788–91.
2 Bovet D. Some aspects of the relationship between chemical
constitution and curare-like activity. Annals of the New YorkAcademy of Science 1951; 54: 407–37.
3 Foldes FF, McNall PG, Borrego-Hinojosa JM. Succinyl-choline: a new approach to muscular relaxation in anes-
thesiology. New England Journal of Medicine 1952; 247:596–600.
4 Lee C. Succinylcholine: its past, present, and future. In: Katz
RL, ed. Muscle Relaxants, Basic and Clinical Aspects. Orlando,San Diego, New York, London, Toronto, Montreal, Syd-ney, Tokyo: Grune & Stratton, 1984: 69–85.
5 Lee C. Suxamethonium in its fifth decade. Bailliere’s ClinicalAnaesthesiology 1994; 8: 417–40.
6 Cooper R, Mirakhur RK, Clarke RSJ, Boules Z. Com-parison of intubating conditions after administration of Org
9426 (rocuronium) and suxamethonium. British Journal ofAnaesthesia 1992; 69: 269–73.
7 Gyermek L, Lee C, Cho YM, Nguyen N, Tsai SK.
Neuromuscular pharmacology of TAAC3, a new non-depolarizing muscle relaxant with rapid onset and ultrashortduration of action. Anesthesia and Analgesia 2002; 94: 879–
85.8 Durant NN, Marshall IG, Savage DS, Nelson DJ, Sleigh T,
Carlyle IC. The neuromuscular and autonomic blocking
activities of pancuronium, Org NC 45, and other pancu-ronium analogues in the cat. Journal of Pharmacy and Phar-macology 1979; 31: 831–6.
9 Bowman WC. Prejunctional and postjunctional cholino-
ceptors at the neuromuscular junction. Anesthesia and Anal-gesia 1980; 59: 935–43.
10 Marshall CG, Ogden DC, Colquhoun D. The actions of
suxamethonium (succinyldicholine) as an agonist and chan-nel blocker at the nicotinic receptor of frog muscle. Journal ofPhysiology (London) 1990; 428: 155–74.
11 Lee C. Conformation, action, and mechanism of action ofneuromuscular blocking muscle relaxants. Pharmacology andTherapeutics 2003; 98: 143–69.
12 Beers WH, Reich E. Structure and activity of acetylcholine.
Nature 1970; 228: 917–22.13 Whittaker M. Genetic aspects of succinylcholine sensitivity.
Anesthesiology 1970; 32: 143–50.
14 Savarese JJ, Ali HH, Murphy JD, Padget C, Lee CM, PonitzJ. Train-of-four nerve stimulation in the management ofprolonged neuromuscular blockade following succinylcho-
line. Anesthesiology 1975; 42: 106–11.
15 Bowman WC, Rand MJ. Striated Muscle and NeuromuscularTransmission. Textbook of Pharmacology, Chapter 17, 2nd edn.London, Edinburgh, Boston, Melbourne, Paris, Berlin,
Vienna: Oxford, Blackwell Scientific Publications, 1980.16 Katz RL, Eakins KE. Pharmacological studies of extraocular
muscles. Investigative Ophthalmology and Visual Science 1967;6: 261–8.
17 Lee C, Jahr JS, Candiotti K, Warriner V, Zornow MH.Reversal of profound rocuronium NMB with sugammadexis faster than recovery from succinylcholine. Anesthesiology
2007; 107: A988.18 Lupprian KG, Churchill-Davidson HC. Effect of suxame-
thonium on cardiac rhythm. British Medical Journal 1960; 17:
1774–7.19 Churchill-Davidson HC, Christie TH, Wise RP. Dual
neuromuscular block in man. Anesthesiology 1960; 21: 144–9.20 Jenden DJ, Kamijo K, Taylor DB. The action of decame-
thonium on the isolated rabbit lumbrical muscle. Journal ofPharmacology and Experimental Therapeutics 1954; 11: 229–40.
21 Gissen AJ, Katz RL, Karis JH, Papper EM. Neuromuscular
block in man during prolonged arterial infusion with suc-cinylcholine. Anesthesiology 1966; 27: 242–9.
22 Ramsey FM, Lebowitz PW, Savarese JJ, Ali HH. Clinical
characteristics of long-term succinylcholine neuromuscularblockade during balanced anesthesia. Anesthesia and Analgesia1980; 59: 110–6.
23 Donati F, Bevan D. Long-term succinylcholine infusionduring isoflurane anesthesia. Anesthesiology 1982; 58: 6–10.
24 Hilgenberg JC, Stoelting RK. Characteristics of succinyl-choline-produced phase II neuromuscular block during
enflurane, halothane and fentanyl anesthesia. Anesthesia andAnalgesia 1981; 60: 192–6.
25 Lee C. Train-of-four fade and edrophonium antagonism of
neuromuscular block by succinylcholine in man. Anesthesiaand Analgesia 1976; 55: 663–7.
26 Lee C. Self-antagonism: a possible mechanism of tachy-
phylaxis in suxamethonium-induced neuromuscular blockin man. British Journal of Anaesthesia 1976; 48: 1097–102.
27 Katz RL, Wolf CE, Papper EM. The non-depolarizingneuromuscular blocking action of succinylcholine in man.
Anesthesiology 1963; 24: 784–9.28 Benumof JL, Dagg R, Benumof R. Critical hemoglobin
desaturation will occur before return to an unparalyzed state
following 1 mg ⁄ kg intravenous succinylcholine. Anesthesi-ology 1997; 87: 979–82.
29 Boros EE, Bigham EC, Boswell GE, et al. Bis- and mixed-
tetrahydroisoquinolinium chlorofumarates: new ultra-short-acting non-depolarizing neuromuscular blockers. Journal ofMedicinal Chemistry 1999; 42: 206–9.
Anaesthesia, 2009, 64 (Suppl. 1), pages 73–81 C. Lee Æ Goodbye suxamethonium!......................................................................................................................................................................................................................
! 2009 The AuthorJournal compilation ! 2009 The Association of Anaesthetists of Great Britain and Ireland 81