Embed Size (px)
DESCRIPTION
Glycolisis, gluconeogenesis, regulation of glucose synthesis
Citation preview

THEME
Metabolism of carbohydrates

DIGESTION OF CARBOHYDRATESDIGESTION OF CARBOHYDRATES
Glycogen, starch and disaccharides (sucrose, lactose and maltose) are hydrolyzed to monosaccharide units in the gastrointestinal tract.The process of digestion starts in the mouth by the salivary enzyme –amilase.
The time for digestion in mouth is limited.
Salivary -amilase is inhibited in stomach due to the action of hydrochloric acid.
Another -amilase is produced in pancreas and is available in the intestine.

-amilase hydrolyzes the -1-4-glycosidic bonds randomly to produce smaller subunits like maltose, dextrines and unbranched oligosaccharides.
-amilase

The intestinal juice contains enzymes hydrolyzing disaccharides into monosaccharides (they are produced in the intestinal wall)
Sucrase hydrolyses sucrose into glucose and fructose
Sucrose
sucrase
Fructose
Glucose

Lactose
lactase
Maltase hydrolyses maltose into two glucose molecules
Lactase hydrolyses lactose into glucose and galactose
Maltose
maltase
Galactose Glucose
GlucoseGlucose

ABSORPTION OF ABSORPTION OF CARBOHYDRATESCARBOHYDRATESOnly monosaccharides are absorbed
The rate of absorption: galactose > glucose > fructoseGlucose and galactose from the intestine into
endothelial cells are absorbed by secondary active transport
Na+ GlucoseProtein
Protein

Carrier protein is specific for D-glucose or D-galactose.
L-forms are not transported.
There are competition between glucose and galactose for the same carrier molecule; thus glucose can inhibit absorption of galactose.
Fructose is absorbed from intestine into intestinal cells by facilitated diffusion.
Absorption of glucose from intestinal cells into bloodstream is by facilitated diffusion.

Transport of glucose from blood into cells of different organs is mainly by facilitated diffusion.
The protein facilitating the glucose transport is called glucose transporter (GluT).
GluT are of 5 types.
GluT1 is seen in erythrocytes and endothelial cells;
GluT2 is located mainly in hepatocytes membranes (it transport glucose into cells when blood sugar is high);
GluT3 is located in neuronal cells (has higher affinity to glucose);
GluT4 - in muscles and fat cells.
GluT5 – in intestine and kidneys;

Glucose
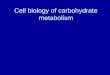
The fate of glucose molecule in the cell
Glucose-6-phosphate
Pyruvate
Glycogen
Ribose, NADPH
Pentose phosphate pathway supplies
the NADPH for lipid synthesis and
pentoses for nucleic acid synthesis
Glycogenesis (synthesis of glycogen) is
activated in well fed, resting state
Glycolysis is activated if
energy is required
Glycogenolysis (degradation of
glycogen)
Gluconeogenesis is activated if glucose is
required


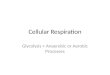
Regulation of Glycolysis
The rate glycolysis is regulated to meet two major cellular needs: (1) the production of ATP, and (2) the provision of building blocks for synthetic reactions.
There are three control sites in glycolysis - the reactions catalyzed byhexokinase, phosphofructokinase 1, and pyruvate kinase These reactions are irreversible.
Their activities are regulated by the reversible binding of allosteric effectorsby covalent modificationby the regulation of transcription (change of the enzymes amounts).
The time required for allosteric control, regulation by phosphorylation, and transcriptional control is typically in milliseconds, seconds, and hours, respectively.

Inhibition1) PFK-1 is inhibited by ATP and citrate2) Pyruvate kinase is inhibited by ATP and alanine 3) Hexokinase is inhibited by excess glucose 6-phosphate
Stimulation1) AMP and fructose 2,6-bisphosphate (F2,6BP) relieve the inhibition of PFK-1 by ATP 2) F1,6BP stimulate the activity of pyruvate kinase
Regulation of Glycolysis
Alanine

Gluconeogenesis - synthesis of "new" glucose from such precursors as pyruvate, lactate, certain amino acids, and intermediates of the tricarboxylic acid cycle.
Most of the reaction steps in the pathway from pyruvate to glucose 6-phosphate are catalyzed by enzymes of the glycolytic sequence and thus proceed by reversal of steps employed in glycolysis. However, there are two irreversible steps in the normal "downhill" glycolytic pathway which cannot be utilized in the "uphill" conversion of pyruvate to glucose 6-phosphate. In the biosynthetic direction these steps are bypassed by alternative reactions.



Reactions Unique to Gluconeogenesis

The first of these bypass steps is the phosphorylation of pyruvate to phosphoenolpyruvate. The first step is catalyzed by pyruvate carboxylase of mitochondria:
pyruvate + CO2 + ATP oxaloacetate + ADP + P
The oxaloacetate formed in this mitochondrial reaction is then reduced to malate at the expense of NADH by the mitochondrial form of malate dehydrogenase:
oxaloacetate + NADH + H+ malate + NAD+
The malate so formed may then leave the mitochondria and in the cytosol the malate is then reoxidized by the cytoplasmic form of NAD-linked malate dehydrogenase to form extramitochondrial oxaloacetate:
malate + NAD+ oxaloacetate + NADH + H+

In the last step of the bypass, oxaloacetate is acted upon by phosphoenolpyruvate carboxykinase (GTP) to yield phosphoenolpyruvate and CO2, a reaction in which GTP serves as the phosphate donor:
oxaloacetate + GTP phosphoenolpyruvate + CO2 + GDP. The second crucial point in gluconeogenesis in which a reaction of the
downhill glycolytic sequence is bypassed is conversion of fructose 1,6-diphosphate into fructose 6-phosphate:
fructose 1,6-diphosphate + H2O fructose 6-phosphate + P.This reaction is catalized by the enzyme fructose diphosphatase.

In some animal tissues, particularly the liver, kidney, and intestinal epithelium, glucose 6-phosphate may be dephosphorylated to form free glucose; the liver is the major site of formation of blood glucose. The hydrolytic cleavage of glucose 6-phosphate does not occur by reversal of the hexokinase reaction but is brought about by glucose-6-phosphatase:
glucose 6-phosphate + H2O glucose + P
Glucose-6-phosphatase is not present in muscles or in the brain, which thus cannot donate free glucose to the blood.

THE PENTOSE PHOSPHATE PATHWAY



Diabetes mellitus
Diabetes mellitus is a disorder in which blood sugar (glucose) levels are abnormally high because the body does not produce enough insulin.Insulin a hormone released from the pancreas, controls the amount of sugar in the blood.The levels of sugar in the blood vary normally throughout the day. They rise after a meal and return to normal within about 2 hours after eating. Once the levels of sugar in the blood return to normal

Doctors often use the full name diabetes mellitus, rather than diabetes alone, to distinguish this disorder from diabetes insipidus, a relatively rare disease that does not affect blood sugar.

Types of Diabetes mellitus
Type 1: In type 1 diabetes ( insulin-dependent diabetes or juvenile-onset diabetes), more than 90% of the insulin-producing cells of the pancreas are permanently destroyed. The pancreas, therefore, produces little or no insulinOnly about 10% of all people with diabetes have type 1 disease. Most people who have type 1 diabetes develop the disease before age 30.

Type 2: In type 2 diabetes ( non-insulin-dependent diabetes or adult-onset diabetes), the pancreas continues to produce insulin, sometimes even at higher-than-normal levels. However, the body develops resistance to the effects of insulin, so there is not enough insulin to meet the body's needs.

Type 2 diabetes may occur in children and adolescents, but usually begins in people older than 30 and becomes progressively more common with age. About 15% of people older than 70 have type 2 diabetes. Obesity is the chief risk factor for developing type 2 diabetes, and 80 to 90% of people with this disease are obese. Because obesity causes insulin resistance, obese people need very large amounts of insulin to maintain normal blood sugar levels.

Symptoms The two types of diabetes have very similar symptoms. The first
symptoms are related to the direct effects of high blood sugar levels (hyperglycemia). When the blood sugar level rises above 160 to 180 mg/dL, sugar spills into the urine (glucoseuria). When the level of sugar in the urine rises even higher, the kidneys excrete additional water to dilute the large amount of sugar. Because the kidneys produce excessive urine, a person with diabetes urinates large volumes frequently (polyuria). The excessive urination creates abnormal thirst (polydipsia). Because excessive calories are lost in the urine, the person loses weight. To compensate, the person often feels excessively hungry. Other symptoms include blurred vision, drowsiness, nausea, and decreased endurance during exercise.