Embed Size (px)
Citation preview

LOWER GI HEMORRHAGE
FISSURE-IN-ANO
Dr.B.SELVARAJ MS;Mch;FICS:
PROFESSOR OF SURGERY
MELAKA MANIPAL MEDICAL COLLEGE
MELAKA 75150 MALAYSIA

FISSURE-IN-ANO
Causes of Lower GI Hemorrhage
Etiopathogenesis
Types of Fissre-In-Ano
Clinical features
Treatment
Mindmap
Diagnostic algorithm
Management Algorithm

Causes for Lower GI Hemorrhage
Diverticular disease
Angiodysplasia- AV Malformation
Colorectal carcinoma
Hemorrhoids
Fissure-in-ano
Ischemic colitis
Inflammatory bowel disease
Meckel’s diverticulum
Upper GI hemorrhage

CLASSICAL CLINICAL VIGNETTE
A 23 year old lady describes excruciating pain with defecation and blood streaks on the outside of the hard stools.
Because of the pain she avoids having bowel movements and when she finally does, the stools are hard and even more painful.
Physical examination can not be done, as she refuses to allow anyone to even “spread her perianal area” to look at the anus for fear of precipitating the pain.
Diagnosis: Fissure-in-ano
EUA should be done to R/O other pathologies like Anal Carcinoma, Crohn’s disease, Tuberculosis, HIV and Leukemia

ETIOPATHOGENESIS
An anal fissure is an ulcer in the lower portion of the anal canal
Most tears of the anal canal are due to the passage of large, hard stool or explosive diarrhea, trauma to the anus, or a tear during vaginal delivery.
Patients have increased resting anal pressure caused by the increased tone of the internal sphincter muscle. This results in ischemia and ulceration to the overlying anal skin.
In men, almost all fissures are located in the posterior midline, whereas in women, 10% are in the anterior midline.

Types of Fissure-in-Ano
Acute Fissure-in-Ano: Symptoms
within one month
Chronic Fissure-in-Ano:
Symptoms 2 to 3 months duration
The primary fissure occurs
without association with other
local or systemic diseases
The secondary fissure occurs in
association with Crohn’s disease,
leukemia or aplastic anemia.

Clinical Features
Bleeding per rectum: Bleeding is painful associated with defecation.
It is bright red blood and blood usally streaks on the hard fecal
matter
Painful defecation: Anal pain during and after defecation is the most
prominent symptom.The pain is described as burning, throbbing, or
dull aching.
Physical examination confirms the diagnosis. Chronic fissures have
a triad of a fissure, sentinel skin tag, and hypertrophied anal papilla
In acute Fissure-in-Ano you shouldn’t do DRE or Proctoscopy for
fear of aggravating the pain.

TREATMENT
Nonoperative for all Acute and some chronic Fissure-in-Ano
a. Sitz bath—The patient is asked to sit in warm water with the anal
region and buttocks dipped in water for about 20 minutes,2 to 3 times
a day. This reduces pain, edema and promotes healing.
b. Antibiotics, laxatives (stool softener) and antiinflammatory drugs
are beneficial.
c. Regulation of bowel habit with a high fiber diet.
d. Local application of nitroglycerin or calcium channel blockers like
diltiazam lowers the resting anal sphincter tone.
e. Injection of Botulinium toxin lowers the resting internal sphincter
tone.

TREATMENT
Operative Treatment:
Anal fissures usually heals in six weeks. Surgery is not usually
required unless the conservative therapy fails.
Lateral internal Sphincterotomy is the surgical procedure of choice if
the anal sphincter tone is normal. This can be done as open or blind
subcutaneous lateral internal Sphincterotomy.
If anal sphincter tone is low- do endoanal v-y skin flap
Fissures or ulcers in Crohn’s disease are larger and deeper than
primary anal fissures. The surrounding skin is macerated and
edematous. Treatment consists of proper anal hygiene and treatment
of the underlying inflammatory disease.

TREATMENT
Notaras Closed blind subcutaneous lateral internal sphincterotomy
Open subcutaneous lateral internal sphincterotomy

MINDMAP
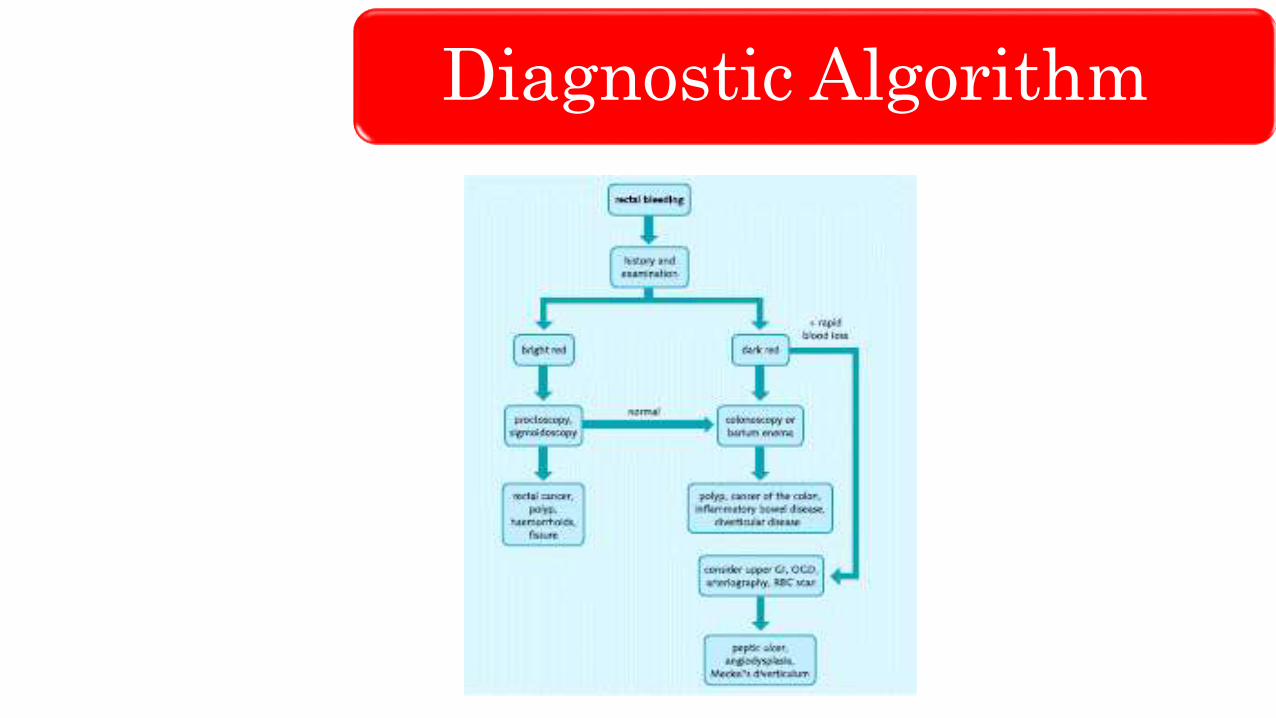
Diagnostic Algorithm

Treatment Algorithm

THANK YOU
LIKE
SHARE
SUBSCRIBE





























