Embed Size (px)
Citation preview

Facial NerveBy
Dr. Ibrahim HabibENT Consultant (MD)

ما) قليال واألفئدة واألبصار السمع لكم وجعلالسجدة ( ) : (9تشكرون
دونه) ( • من الذين خلق ماذا فأروني الله خلق هذا ( 10لقمان) :
ال) • يوم يأتي أن قبل من القيم للدين وجهك فأقمالروم ( ) : الله من له (43مرد

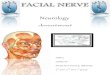
Facial Nerve Anatomy
Mixed nerve
• Sensory: from Nucleus Solitarius• Motor : Facial nucleus (at the level of Pons)• Parasympathetic: superior salivary
nucleus

Segments of Facial Nerve Length Course
From toSegment
23 -24 mm IAC Brain stem Meatal
3 -5 mm Geniculate ganglia
Metal foramen Larynthine
8 – 11 mm Pyramidal eminence
Geniculate ganglia
Tympanic70% dehiscent
10 – 14mm Stylomastoid foramen
Pyramidal eminence Mastoid
15 -20 mm Muscles supplied by it
Stylomastoid foramen
Extratemporal

Course of Facial Nerve




Branches of Facial Nerve

Facial N. BranchesStructure supplied Type of the
nerveBranches
Post. Belly of digastric muscle.Styloid m.
Motor Post. auricular
Muscles of facial expression
Motor Temporal
Muscles of facial expression
Motor Zygomatic
Muscles of facial expression
Motor Buccal
Muscles of facial expression
Motor Mandibular

Facial N. Branches( cont. )Structure supplied Type of the
nerveBranches
Muscles of facial expressionplatysma
Motor cervical
Stapedius Motor Nerve to Stapedius
Lacrimal gland ( via synapse in pterygo-palatine ganglion)
Parasympathetic secretomotor
Greater petrosal
Submandibular & sublingual gland ( via synapse in the submandibular ganglion
Parasympathetic secretomotorTaste ( join lingual n. to supply the tongue).
Chorda tympani
Area of skin around the external auditory meatus.
Somatic sensory Fibers to geniculate ganglion

Pathophysiology of nerve injury
• Neuropraxia : Blocks flow of axoplasm from stoma to distal axon.
• Axonotemesis : Wallerian degeneration with intact endoneural tubules.
• Neurotemesis : Wallerian degeneration with loss of endoneural tubules .
• Transection : Complete division of the nerve .

Facial nerve paralysis: Signs• Facial asymmetry • Eyebrow droop • Loss of forehead & nasolabial folds • Drooping of corner of mouth • Uncontrolled tearing • Inability to close eye • Lips cannot be held tightly together :
difficulty keeping food in mouth • Facial muscle atrophy ( late (

Facial nerve palsy

Clinical Testing of Facial Nerve Functions1. Observe patient Face during rest & movement for :
• Asymmetry• Hemi facial spasm• Facial tics• blinking

Clinical Testing of Facial Nerve Functions2. Blink test: Delay in blinking on one
side3. Testing facial movementi. Temporal branch: To wrinkle forehead,
To elevate eye browii. Zygomatic branch: to screw up the eyeiii. Buccal branch: to wrinkle the noseiv. Mandibular branch: to show the teeth, to
blow out the cheeksv. Crvical branch: by grimacing

House-Brackmann grading system of facial function
Degree of injury
Definition Grade
Normal Normal symmetrical function IMild dysfunction Slight weakness & asymmetry
Complete closure of the eye with minimal effort. Barely notice Synkinesis.
absent ( contructure or spasm )
II
Moderate dysfunction
Obvious weakness & asymmetryObvious Synkinesis, mass movement or spasmNo disfiguring
III

House-Brackmann grading system of facial function (cont.)
Degree of injury Definition Grade
Moderately severe dysfunction
Obvious disfiguring, weakness & asymmetrySever synkinesis, mass movement , spasm
IV
Severe dysfunction
Barely perceptible motionAbsent Synkinesis, contructure ,spasm
V
Total paralysis No movement , loss of tone no synkinesis, contructure or spasm
VI

Features associated with facial palsy
• Synkinesis: movement of group of muscles that don’t usually contract together.
• Hemifacial spasm: an intermittent spasm of some or all of the facial muscles
• Facial myokymia: multiple facial movement.
• Blepharospasm: involuntary spasmodic eye closure
• Crocodile tears: lacrimation with eating due to regenerating motor nerve fibers connect the greater petrosal nerve.

Topognostic testing
• Help to determine the site of facial n. injury

Supranuclear lesion:
Lower face palsy associated with neurological deficit
Nuclear lesion:Motor function affected only

C P A , labyrinthine segment , geniculate ganglion lesions:
Lacrimation , stapedeal reflex , taste , salivation impaired
Lesion between geniculate g. and n. to stapedius :
Stapedeal reflex , taste , salivation lost .

Lesion between stapedius and chorda tympani n.:
Taste impaired .
Lesion bellow chorda tympani n. :
Pure motor deficit .

Topognostic testing of Facial palsySignificance principle evaluate Test
↓of 75% or more of affected side
↓of 30% or more of total lacrimation on both sides
Tear production G.S.P.N Schirmer
If stapedial reflex absent in spite of normal hearing →the site of lesion proximal to branch to stapedius m.
Contraction of stapedius m.
N. To stapedius m.
Stapedeal reflex test
Metallic sensation.Normal threshold is 1mA.If ↑up to 4 mA. → chorda tympani is affected (rarely done)
Taste testing of ant. 2\3 of the tongue
Chorda tympani
Electrogastrometry

Topognostic testing of Facial palsy (cont.)
significance principle evaluate Test
↓salivation by 25% compared to normal side → chorda tympani is affected (but difficult & inaccurate)
Submandibular gland flow
Chorda tympani sialometry
Difference of 3.5mA. Or greater between 2 side→ degeneration →surgical decompression
Compare the minimal current necessary to elicit minimal muscle contraction when applied to branch of facial nerve on normal side to paralyzed side
Nerve degeneration
Minimal excitability test
No value for 1st 72 hEqual responseReduced responseAbsent responseFrequent testing shows progressive ↑ threshold →continuing degeneration
Compare the effect of nerve stimulator at highest level tolerated by the patient in normal side to paralyzed side
Nerve degeneration
Maximal stimulator test

Topognostic testing of Facial palsy (cont.)
significance principle evaluate Test
The degree of degeneration is directly proportion al to the amplitude loss of measured summation potential Not useful during 1st 72 h
90% or more degeneration indicate decompression within 3 weeks
Compare compound action potential of facial n. after supramaximal stimulation of both sides
Nerve degeneration
Electroneurography( ENG)
Fibrilation potential manifest 2 weeks after the onset of facial paralysis
(diagnostic)Polyphasic reinnervation potential 6- 12 weks prior to clinical return of facial function ( prognostic)
Activity of the muscle itself during rest & voluntary contraction
Activity of muscle itself (demonstrate survival of motor units)
Electromyography (EMG)

Causes of facial nerve palsy
1. Congenital Birth trauma. Inherited disorder .Mytonic dystrophyAlbers –Schoenberg disease Osteoporosis of bony canals for cranial n. III, VIII
& VII cranial n. affected.Developmental abnormalities .Moebius syndromeOcculo-auriculo-vertebral syndrome

Causes of facial nerve palsy(cont.)
2. Inflammatory : Bell’s palsy ( an acute peripheral self- limiting
(55% ) non progressive facial paralysis due to viral inflammatory process
Ramzy Hunt syndrome (7%) (herpes zoster virus causes facial palsy and vesicles often visible in ext. ear canal & on tympanic membrane.
Lyme disease ( tick - born spirochaete causes facial paralysis in children)

Causes of facial nerve palsy(cont.)
AIDS ( HIV causes facial paralysis as a result of :
-herpes zoster Atticus -progressive multifocal
leucoencephalopath - NeoplasmSuppurative otitis media( 4%) - facial paralysis may complicate acute or
chronic suppurative otitis media or malignant otitis externa.

Causes of facial nerve palsy(cont.)
- In ASOM.: infection spreads through congenital dehiscence.
- In chronic SOM: compression of facial n. by cholesteatoma or granulation tissue
- In malignant otitis externa Pseudomonas causes infection of ear canal in immunocompromised patient forming granulation tissue in ear canal , spread of infection causes facial paralysis and other cranial nerve affection .

Causes of facial nerve palsy(cont.)
3. Neoplasm ( 6% )• Benign facial n. tumours :
• Schwanoma• Meningioma , angiomas , haemangiomas .
• Malignant facial n, tumours :
• Acoustic neuromas .

Causes of facial nerve palsy(cont.)
4. Traumatic facial nerve paralysis ( 19 %)
• Iatrogenic injury :• Chronic ear surgery .• Parotid tumor resection .• Facial nerve tumor resection .• Resection of acoustic tumor .• Temporal bone fracture .• Facial wounds .

cholesteatoma

Acinic cell tumour

parotidecomy


C T temporal bone fracture

Temporal bone fracture

Acoustic neuroma

Causes of facial nerve palsy(cont.)
5. Other causes :
• Multiple sclerosis .
• Cerebrovascular accident .
• Myasthenia gravis .
• Sarcoidosis .

Treatment of facial palsy• Eye protection
• Specific treatment :• Bell’s palsy ; steroids and decompression .
• Ramsay Hunt syndrom ; acyclovir .
• Trauma ; exploration and repair .
• Tumour ; may need facial nerve sacrifice .
• Infection ; in chronic otitis media need mastiod exploration.•

ventilation tube insertion

mastoidectomy

Thank you
• Dr. Ibrahim Habib Barakat ENT consultant (MD)
•E-mail :[email protected]•www.facebook.com/Dr.Ibrahim.Barakat