Embed Size (px)
Citation preview
The Elective Care Approach at the Royal Free London NHS Foundation Trust
David Sloman Chief executive
Kate Slemeck Chief operating officer
Background and context to the Royal Free London NHS Foundation Trust

Modern history
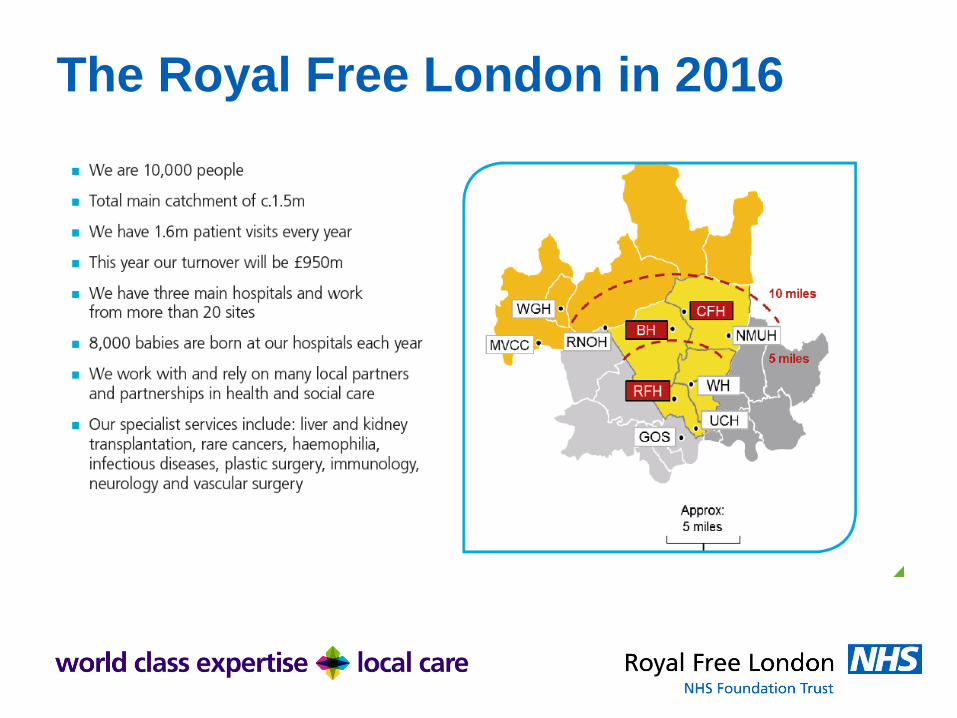
The Royal Free London in 2016
Inherited problems
• Legacy BCF had stopped nationally reporting in September 2013
• 1.8m pathways on the waiting list
• 75,000 pathways requiring individual validation to ensure accurate reporting
• No rigorous PTL monitoring
• Lack of operational grip on capacity planning
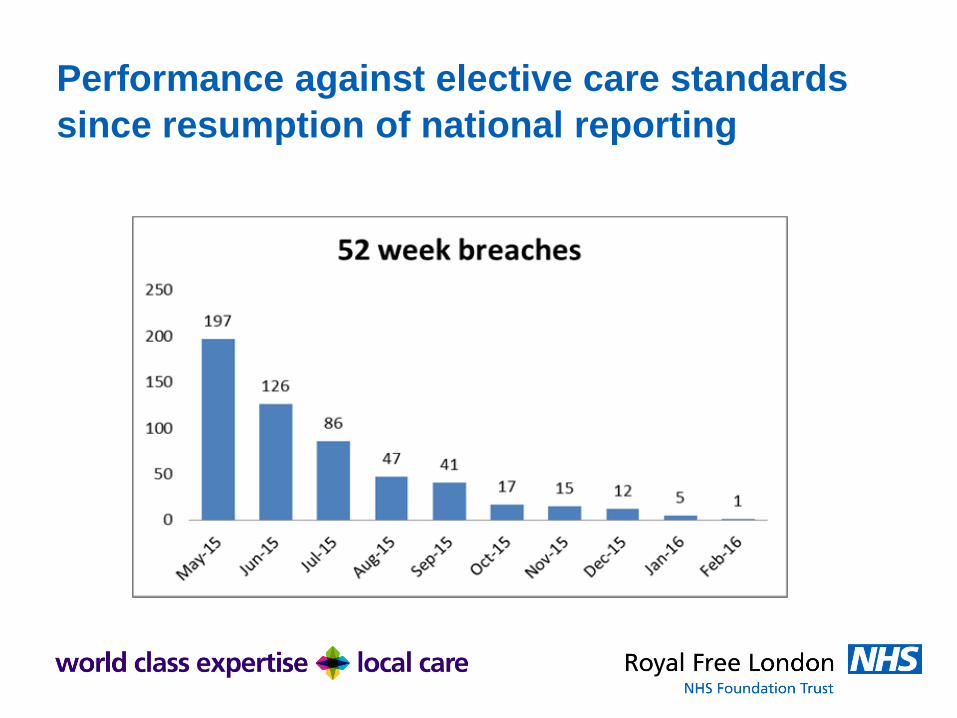
Performance against elective care standards
since resumption of national reporting
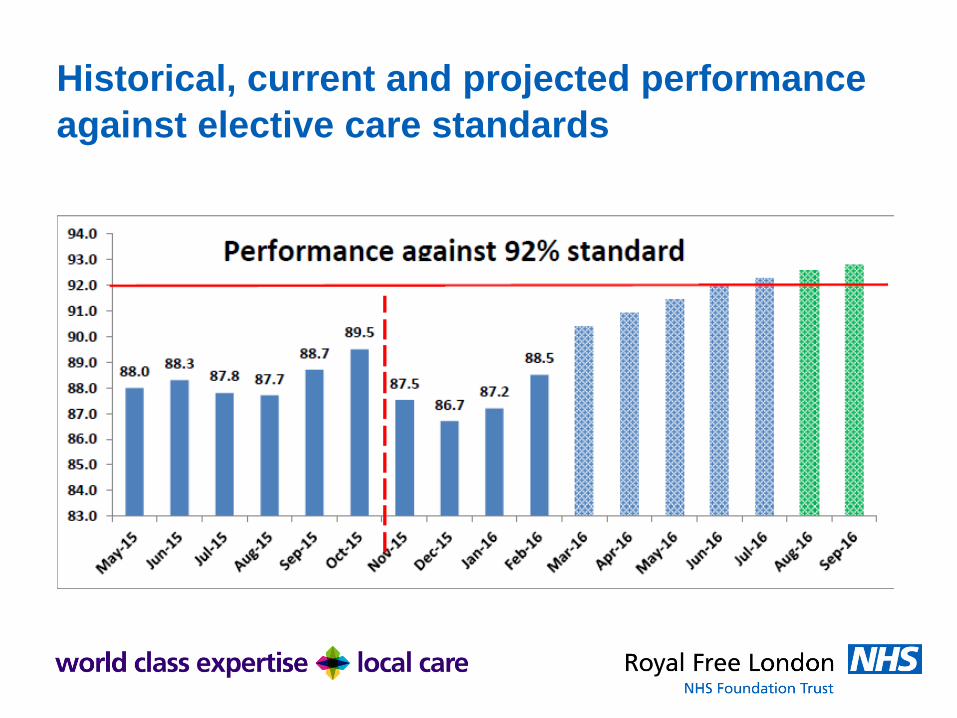
Historical, current and projected performance
against elective care standards
Challenges – 1/4 Data validation and data quality:
• Thousands of pathways requiring individual validation to
ensure accurate reporting
• 2 PAS systems with limited RTT management
• 2 legacy PTL’s
• Sporadic use and implementation of outcome forms
Training:
• Limited trust-wide understanding of RTT
• 2 legacy elective access policies harmonised into one
large version
• No trust-wide aligned training package
Challenges – 2/4
PTL Monitoring:
• 2 legacy PTL monitoring meetings with very different cultures and outputs
• Lack of accountability for the PTL from clinicians and operational managers
• Lack of rigorous and active waiting list management

Challenges – 3/4
Capacity Planning
• No formal demand and capacity model for elective, emergency or diagnostic pathways
• WLI activity was unplanned and random and being used as business as usual activity
• Lack of consultant and management buy-in to outsourcing
• High cost of independent sector tariffs
Challenges – 4/4
Clinical harm
• Large number of patients waiting in excess of 52 weeks without having had a clinical review
System
• Working with commissioners and regulators who were highly anxious about the situation

Governance

Assurance
RTT Programme Board membership
• Chief Executive (Chair)
• Chief Operating Officer
• Medical Director
• Director of Nursing
• NHS Intensive Support Team
• Director of Planning
• Divisional Director of Surgery
• Director of Workforce and OD
• Director of Communications
• RTT Programme Director
• Chair, Barnet CCG (lead commissioner)
• Accountable Officer, Barnet CCG
• Accountable Officer Herts Valleys CCG
RTT Steering Group membership
• Chief Operating Officer (Chair)
• RTT Programme Director
• Clinical Directors of anaesthetics,
theatres, outpatients, T&O
• Divisional Directors for all divisions
• Divisional Directors of Nursing
• Head of Reporting and Analytics
• Head of Performance
• Clinical Harm Lead
• Head of external communications
• IST representative
• Finance representative
Learning Key ingredients for sustainability & success
• Mobilised in-house senior management to manage the recovery
• Methodical and systematic plan for recovery
• Best validation involves talking to the patient
• Centralised validation team
• Real time monitoring of backlog recovery
• Established outsourcing team with strong links with the independent sector
• Robust trust-wide training programme underpinned by elective access policy
Successes
• Carried out 10,793 clinical harm reviews to provide assurance that patient safety had not been affected
• Launched the Royal Free London validation wheel
• The RTT programme team created and developed 2 e-learning modules which has been incorporated into our mandatory training suite
• Outsourcing team – developed a team who seeks additional capacity, and manages patients safely through the pathways
Top Tips
• Executive engagement – Led from the top
• Recovery programme sits within operations – Programme Director reporting to Chief Operating Officer.
• Early engagement and ongoing involvement of IMAS
• Telephone agency utilised to call patients
• Seek buy-in from clinicians for outsourcing
• Ensure the timing of the switch from recovery to BAU is neither too soon or too late





























