Embed Size (px)
DESCRIPTION
ESC and ACC/AHA dyslipidemia guidelines
Citation preview

Dyslipidemia guidelines update
ByAshraf Reda, MD, FESC
Prof and head of Cardiology Dep. Menofiya University

LDL-C Goals for High Risk Patients
*And other forms of atherosclerotic disease.2
† Factors that place a patient at very high risk: established cardiovascular disease plus: multiple major risk factors (especially diabetes); severe and poorly controlled risk factors (e.g., cigarette smoking); metabolic syndrome (triglycerides ≥200 mg/dL + non–HDL-C ≥130 mg/dL with HDL-C <40 mg/dL); and acute coronary syndromes.1
1. Grundy SM et al. Circulation 2004;110:227–239.2. Smith SC Jr et al. Circulation 2006; 113:2363–2372.
<100 mg/dL
<70 mg/dL
Recommended LDL-C treatment goals
2006Update
• If it is not possible to attain LDL-C <70 mg/dL because of a high baseline LDL-C, it generally is possible to achieve LDL-C reductions of >50% with more intensive LDL-C–lowering therapy, including drug combinations.
ATP IIIUpdate 20041
<100 mg/dL:Patients with CHD or CHD risk equivalents(10 year risk >20%)1
<70 mg/dL:Therapeutic option for very high risk patients1
AHA/ACC guidelinesfor patients with CHD*,2
<100 mg/dL:Goal for all patients with CHD†,2
<70 mg/dL:A reasonable goal for all patients with CHD2

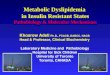
Goals
LDL-C Non–HDL-C Apo B
Highest-Risk Patients <70 mg/dL <100 mg/dL <80 mg/dL
• Known cardiovascular disease (CVD)
• Diabetes plus ≥1 additional major CVD risk factor
High-Risk Patients <100 mg/dL <130 mg/dL <90 mg/dL
• No diabetes or known CVD but ≥2 major CVD risk factors
• Diabetes but no other major CVD risk factors
“In individuals on statin therapy who continue to have low HDL-C or elevated non–HDL-
C, especially if Apo B levels remain elevated, combination therapy is recommended. The preferred agent to use in combination with a statin is nicotinic acid…”
Reprinted from Brunzell JD, et al. J Am Coll Cardiol.2008;51:1512–1524 ,with permission from Elsevier.
ADA/ACC 2008 Consensus Statement:Treatment Goals for Patients With
Cardiometabolic Risk and Lipoprotein Abnormalities

ESC/EAS 2011
• Life style intervention should be tried first• If not effective statin is the first choice• Addition of Ch. Absorption inhibitors, bile acid
Seq. or niacin if not at goal

Calculating the risk: SCORE
• Very high, high, moderate or low risk• Total and HDL-c are incorporated• Relative risk charts for young apparently low
risk individuals• Charts for low and charts for high risk region• Charts for different HDL levels

LDL levels are the main target of lipid management
• Less than 115 mg/dl in moderate risk• Less than 100 mg/dl in high risk• Less than 70 mg/dl in very high risk
• If target can’t be achieved………50% reduction• Non-HDL-c and Apo-B potential targets in
DM2, Met.S and combined dyslipidemia

Non-HDL Includes All Atherogenic Lipoprotein Classes
Very low-density lipoprotein– Made in the liver– TG >> CE– Carries lipids from the liver to peripheral tissues
HDL
LDL
IDL
VLDL
Atherogenic
Lip
op
rote
ins
No
n-H
DL
; A
po
B1
00-
con
tain
ing
Intermediate-density lipoprotein– Formed from VLDL due to loss of TG– Also known as a VLDL remnant
Low-density lipoprotein – Formed from IDL due to loss of TG– CE>>TG
High-density lipoprotein– Removes cholesterol from peripheral tissues
Lp(a)Lipoprotein (a)
– Formed from LDL w/ addition of apo (a)?– Very atherogenic

LIPID PROFILEEGYPTIAN RF AND LIPID PROJECT

Non-HDL-c and Apo-B targets
• The goal for non HDL-c is 30 mg above LDL goal
• Apo-B goal less than 80 mg/dl in very high and less than 100 mg/dl in high risk
• Especially considered as 2ry target in atherogenic dyslipidemia with average LDL

American Diabetes Association (2009)Treatment recommendations and goals
• Statin therapy should be added to lifestyle therapy, regardless of baseline lipid levels, for diabetic patients:– with overt CVD – without CVD who are over the age of 40 and
have one or more other CVD risk factors.
Level of Evidence
A
A
DIABETES CARE, VOLUME 32, SUPPLEMENT 1, JANUARY 2009

American Diabetes Association (2009)Treatment recommendations and goals
• In individuals without overt CVD, the primary goal is an LDL cholesterol 100 mg/dl.
• In individuals with overt CVD, a lower LDL cholesterol goal of 70 mg/dl, using a high dose of a statin, is an option.
• If drug-treated patients do not reach the above targets on maximal tolerated statin therapy, a reduction in LDL cholesterol of 30–40% from baseline is an alternative therapeutic goal.
Level of Evidence
A
B
A
DIABETES CARE, VOLUME 32, SUPPLEMENT 1, JANUARY 2009

Although there are no specific goals , however Trigs., and HDL are important risk determinant

If TG are 200–499 mg/dL, non-HDL-C should be <130 mg/dL
Lipid Management in high TG: Recommendation
l lla llb lll
B
l lla llb lll
BFurther reduction of non-HDL-C to <100 mg/dL is reasonable
Therapeutic options to reduce non-HDL-C:More intense LDL-C–lowering therapy I (B) orNiacin (after LDL-C–lowering therapy) IIa (B) orFibrate (after LDL-C–lowering therapy) IIa (B)
l lla llb lll
CIf TG are >500 mg/dL, therapeutic options to prevent pancreatitis are fibrate or niacin before LDL lowering therapy; and treat LDL-C to goal after TG-lowering therapy, Achieve non-HDL-C <130 mg/dL, if possible
TG=Triglycerides; HDL-C=high-density lipoprotein cholesterolSmith SC Jr et al. Circulation 2006;113:2363–2372 .

Elevated Triglycerides
Non-HDL Cholesterol: Secondary Target
• Primary target of therapy: LDL cholesterol• Achieve LDL goal before treating non-HDL
cholesterol• Therapeutic approaches to elevated non-HDL
cholesterol– Intensify therapeutic lifestyle changes– Intensify LDL-lowering drug therapy– Nicotinic acid or fibrate therapy to lower VLDL

Genetic dyslypidemia
• Familial combined hperlipidemia is not rare: 1% of population
• Often unrecognized and untreated• Early detection and management

The issue of non-adherence
• Important barrier to dyslipidemia management
• Responsibility of Pt. Dr., and health care system

Implication of the new American guidelines: which one should we follow?
• ATP III 2002 JAMA (NHLBI)• The new one (ACC/AHA/ NHLBI)• The hottest in AHA 2013
• Key feature: from specific lipid goal to % reduction

The new American guidelines: Key features: Statin leeagable sub groups
• Clinical Atherosclerotic CVD• LDL> 190 mg/dl• Type 1 or 2 DM & LDL> 70 mg/dl• 10 year risk > 7.5% & LDL >70 mg/dl (New risk
calculator)

The new American guidelines: Sub groups with doughtful benefits from statin
• > 75 yrs without clinical Atherosc. CVD
• A need for hemodialysis
• Heart filure

The American guidelines: key features
• High or moderate intensity statin therapy when lipid lowering is indicated
• Diminished role of non statin lipid lowering agents alone or in combination
• Avoid LL drugs in certain group• No routine LDL assessment• New risk calculator and extended use in
primary prevention

Guidelines are important but they are just guidelines

Conclusions
• More aggressive approach• Early screening and management• Incorporation of Tgs. And HDL in risk evaluation• LDL is still the primary target• Non HDL-c is a secondary target in DM2, Met.S
and combined dyslipidemia• Is it the end of non statin LL agents and
combination?