Embed Size (px)
Citation preview
DUTY REPORTEMERGENCY ROOM29TH MAY 2015ACUTE ABDOMEN WITH OBSTRUCTIVE JAUNDICE CAUSED BY SUSPECTED CHOLEDOCHOLITHIASISUNCONTROLLED GRADE II ESSENTIAL HYPERTENSION
GP on duty: dr. Karen Pandhika & dr. Husnah
Co-ass on duty: Raymond Pranata & Grace Fonda
Supervisor : dr Soroy Lardo SpPD FINASIM
PPDS FKUI
Department Of Internal Medicine
Indonesia Army Central Hospital Gatot Soebroto

RECAPITULATION
1. Mr. Y GERD
2. Mrs. S Abdominal pain in jaundice e.c. cholecystitis
3. Mr. Y dyspnea e.c. suspect COPD
4. Mr. B polycythemia vera
5. Mrs. S dyspepsia + herpes zoster infection
6. Mr. S dyspnea e.c. acute asthma exacerbation
7. Mr. G dyspnea e.c. acute asthma exacerbation +
neurodermatitis + Hepatitis C
8. Mrs. M acute psychosis
9. Ms. G acute gastroenteritis e.c. viral infection
10. Ms. S acute gastroenteritis e.c. suspect food intoxication

PATIENT’S IDENTITY
Name : Mrs. S Age : 61 y.o Occupation : housewife Medical record No : 09-51-xx Address :

ANAMNESIS
Alloanamnesis with patient’s daughter
Chief complaint:
Abdominal pain since 1 week before admission
Additional complaint:
Jaundice
Pale color stool
Dark color urine

1 week before admission
• Sudden onset abd. pain, radiating to epigastrium, back and shoulder
• Dark urine color + acholic stool
• Not relieved with antacid
3 days before admission
• Abd. pain persists
• Sclera looked icteric on both eyes
• 2d before admission whole body jaundice
Days of admission
• Abd. pain persists
• Blood test 1d before admission increase liver function test and bilirubin

HISTORY OF PRESENT ILLNESS
Abdominal pain since 1 week before admission
Site: Right upper quadrant
Onset: sudden at midnight (1 week before admission)
Characteristic: sharp, stabbing
Radiation: to epigastrium, back, and shoulder
Not improve with antacid or food, not relieved by defecation
Continuous throughout the day and interfere with daily
activities
Getting worse with activity and deep inspiration
Weight loss (-)

Associated symptoms:
Jaundice
Sclera 3 days
before admission
Whole body 2 days before admission
Pruritus (-)
Dark urine color (‘tea’ color)
Onset: 1 week
before admission
Frequency: no
changes
No blood, painless
Pale color
stool
Onset: 1 week
before admission
Consistency: no
changes
Blood (-), mucus
(-), steatorrhea (-)
Tenesmus (-), foul
smell (-)

History of other systemic illnesses:
Uncontrolled hypercholesterolemia
Uncontrolled hypertension with BetaBlock™
High uric acid controlled without drug
Habits:
Frequent consumption of fried and oily food
Alcohol bingeing (-)
Smoking (-)
NSAID use (-)
History of past illnesses (including surgery)
Appendectomy at year 2009
Cataract surgeries on both eyes
Patient had once been admitted to hospital because of
abnormally high blood cholesterol and cardiomegaly
History of family illnesses
DM (-)
Hypertension (+) in both parents
Cardiovascular disease (+) in father at age 50
Cerebrovascular disease (-)
Kidney disease (-)
Hypercholesterolemia (-)
Allergy (-), Asthma (-)
PHYSICAL EXAMINATION
General Examination
General condition: moderately ill
State of consciousness: compos mentis
Vital signs:
Blood Pressure : 150/80 mmHg
Heart rate : 98 bpm
Respiratory : 22x/minute
Temperature : 36,7oC
Body weight : 82 kg
Body height : 165 cm
Body mass index :
Head : normocephal
Eye : sclera icteric +/+, pale conjunctiva -/-
ENT : nasal flare (-), discharge (-), blood (-),
hyperemic pharynx (-)
Mouth : moist lip, papillary atrophy (-)
Neck : JVP 5+1cmH2O
Skin : generalized jaundice

Thorax
Pulmonary examination
Inspection: normochest, symmetrical lung movement, scar (-)
Palpation: symmetrical chest expansion and vocal fremitus,
mass (-), tenderness (-)
Percussion: sonor at both lung field
Auscultation: VBS +/+, no additional breath sound
Cardiac examination
Inspection: ictus cordis not visible
Palpation: ictus cordis not palpable
Percussion: right cardiac border at ICS IV right parasternal line,
left cardiac border at ICS V left mid-clavicular line, upper border
at ICS III left parasternal line
Auscultation: normal S1/S2 regular, no murmur, no gallop
Abdomen
Inspection: flat, jaundice, no venous engorgement
Auscultation: bowel sound (+) 8 times per minute
Percussion: tympanic on four abdominal quadrant,
shifting dullness (-)
Palpation: supple, tenderness (+) on epigastrium and
RUQ, (+) rebound tenderness in RUQ, Murphy sign (+),
splenomegaly (-), liver palpation was not done due to
tenderness, fluid wave (-)
Extremities: CRT <2 seconds, warm distal extremities, no
edema, no deformities, jaundice
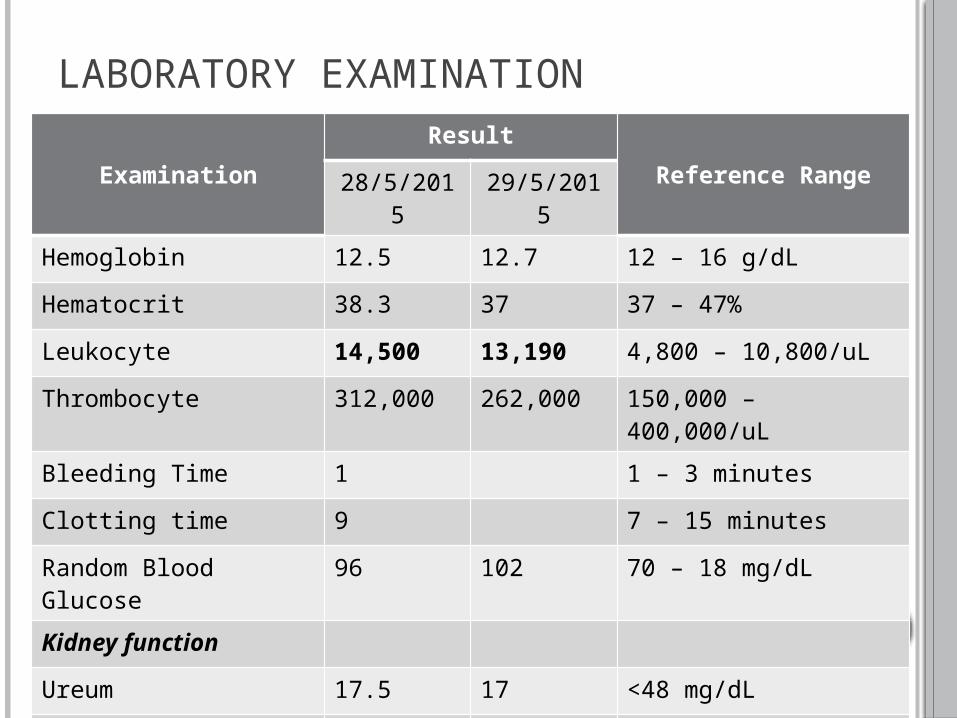
LABORATORY EXAMINATION
ExaminationResult
Reference Range28/5/2015 29/5/2015
Hemoglobin 12.5 12.7 12 – 16 g/dL
Hematocrit 38.3 37 37 – 47%
Leukocyte 14,500 13,190 4,800 – 10,800/uL
Thrombocyte 312,000 262,000 150,000 – 400,000/uL
Bleeding Time 1 1 – 3 minutes
Clotting time 9 7 – 15 minutes
Random Blood Glucose
96 102 70 – 18 mg/dL
Kidney function
Ureum 17.5 17 <48 mg/dL
Creatinine 0.8 0.5 0.45 – 0.75 mg/dL
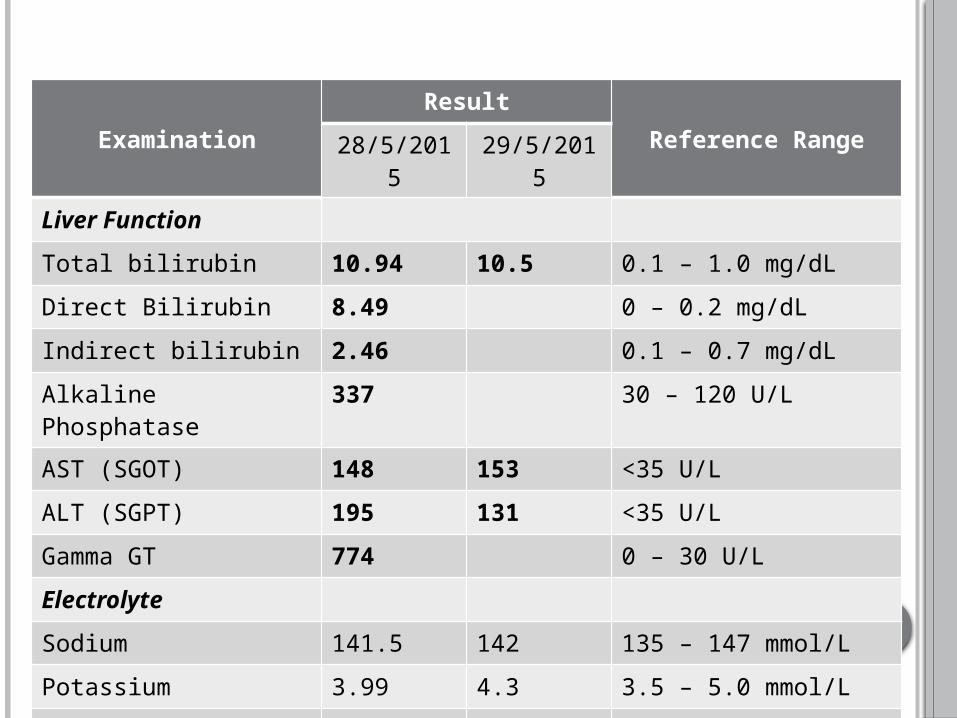
ExaminationResult
Reference Range28/5/2015 29/5/2015
Liver Function
Total bilirubin 10.94 10.5 0.1 – 1.0 mg/dL
Direct Bilirubin 8.49 0 – 0.2 mg/dL
Indirect bilirubin 2.46 0.1 – 0.7 mg/dL
Alkaline Phosphatase 337 30 – 120 U/L
AST (SGOT) 148 153 <35 U/L
ALT (SGPT) 195 131 <35 U/L
Gamma GT 774 0 – 30 U/L
Electrolyte
Sodium 141.5 142 135 – 147 mmol/L
Potassium 3.99 4.3 3.5 – 5.0 mmol/L
Chloride 101.5 107 95 – 105 mmol/L

Abdominal ultrasonography (23/05/2015 at
Ananda Hospital, Bekasi)
Thickening of gallbladder wall (thickness: 6,5mm)
Sludge (+)
Suggestive of cholecystitis

RESUME
Patient, 61 y.o female came with chief complaint of RUQ
abdominal pain radiating to epigastrium, back, and shoulder
since 1 week before admission. No fever. Nausea (+), vomit (-).
Dark color urine (+), acholic stool (+). Jaundice (+) since 3 days
before admission. History of hypercholesterolemia, uncontrolled
hypertension, high uric acid.
PE: high BP, generalized jaundice (+), (+) tenderness on
abdominal palpation, rebound tenderness on RUQ, Murphy
sign (+), ascites (-)
Lab: leukocytosis, direct hyperbilirubinemia, increased
ALT/AST/ALP/GGT
Abd. Ultrasound suggestive of cholecystitis
LIST OF PROBLEMS
Acute abdomen
Jaundice with direct hyperbilirubinemia and
elevated liver function test
Uncontrolled grade II hypertension
Suspected hypercholesterolemia (?)
Suspected hyperuricemia (?)

WORKING DIAGNOSIS
1. Acute abdomen with obstructive jaundice caused
by suspected choledocholithiasis
2. Uncontrolled grade II essential hypertension
Differential diagnosis:
3. Acute abdomen with obstructive jaundice caused
by suspected cholecystitis dd/ ascending
cholangitis
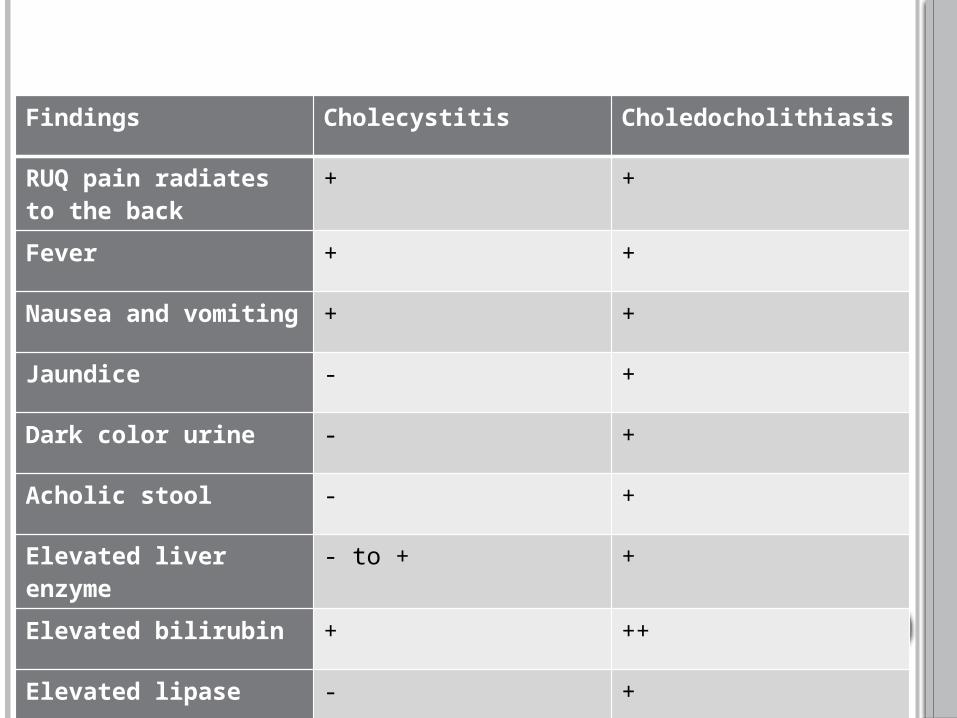
Findings Cholecystitis Choledocholithiasis
RUQ pain radiates to the back
+ +
Fever + +
Nausea and vomiting
+ +
Jaundice - +
Dark color urine - +
Acholic stool - +
Elevated liver enzyme
- to + +
Elevated bilirubin + ++
Elevated lipase - +

RECOMMENDATION
Further examination:
ERCP + US of biliary tree to see the presence of
common bile duct stone
Serum lipase
Funduscopy: to exclude hypertensive retinopathy
Chest x-ray
ECG LVH (?), arryhthmia (?)
Urinalysis bilirubin, protein (nephropathy?)
Lipid profile dyslipidemia (?)
Serum uric acid hyperuricemia(?)
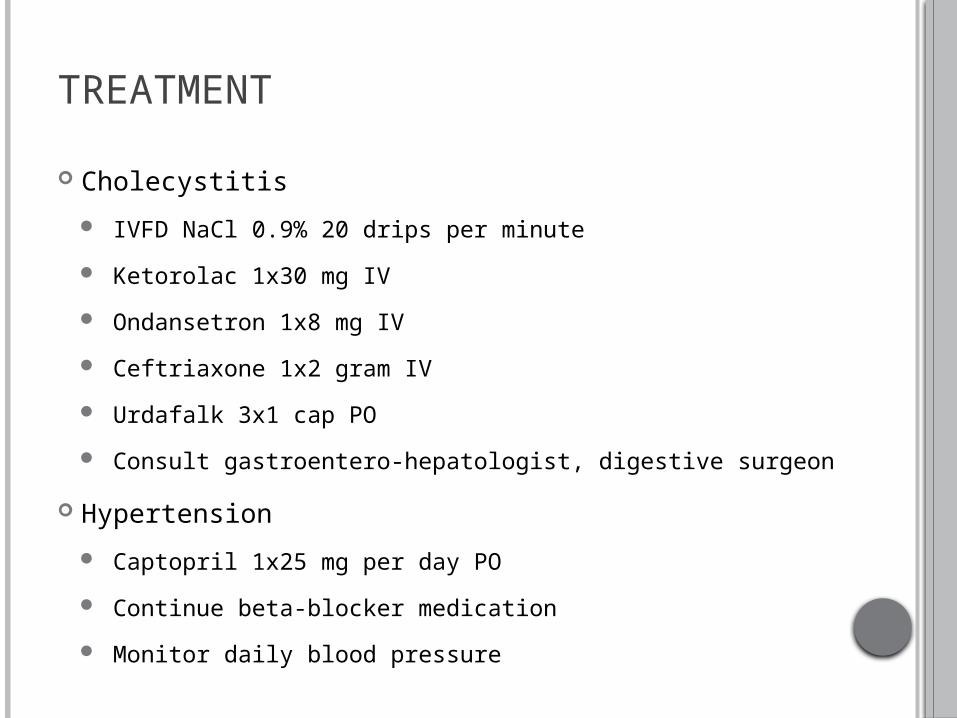
TREATMENT
Cholecystitis
IVFD NaCl 0.9% 20 drips per minute
Ketorolac 1x30 mg IV
Ondansetron 1x8 mg IV
Ceftriaxone 1x2 gram IV
Urdafalk 3x1 cap PO
Consult gastroentero-hepatologist, digestive surgeon
Hypertension
Captopril 1x25 mg per day PO
Continue beta-blocker medication
Monitor daily blood pressure
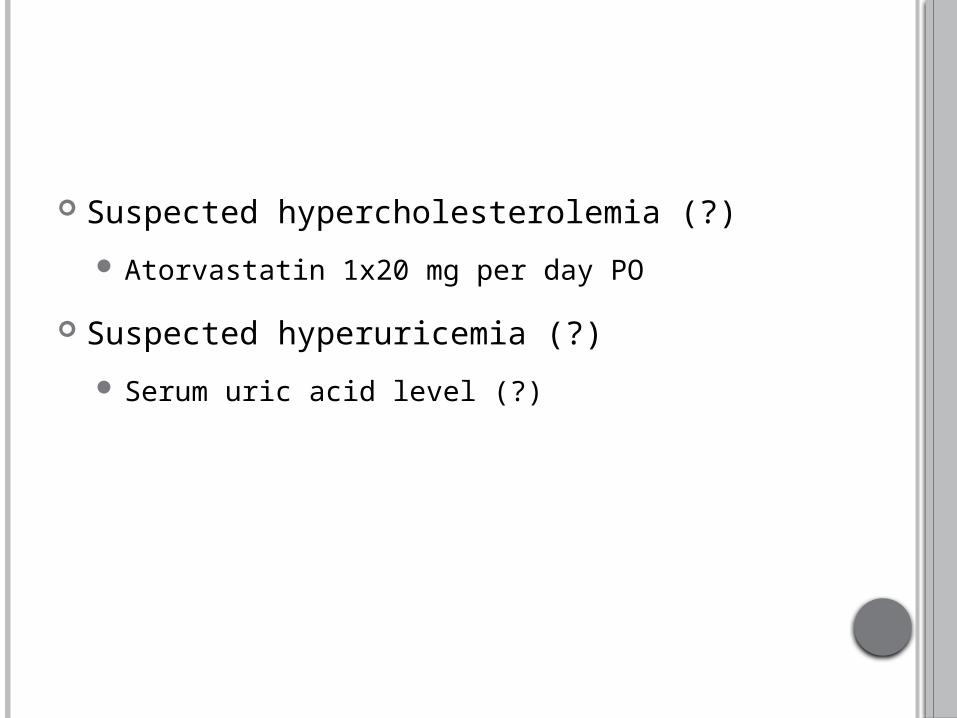
Suspected hypercholesterolemia (?)
Atorvastatin 1x20 mg per day PO
Suspected hyperuricemia (?)
Serum uric acid level (?)

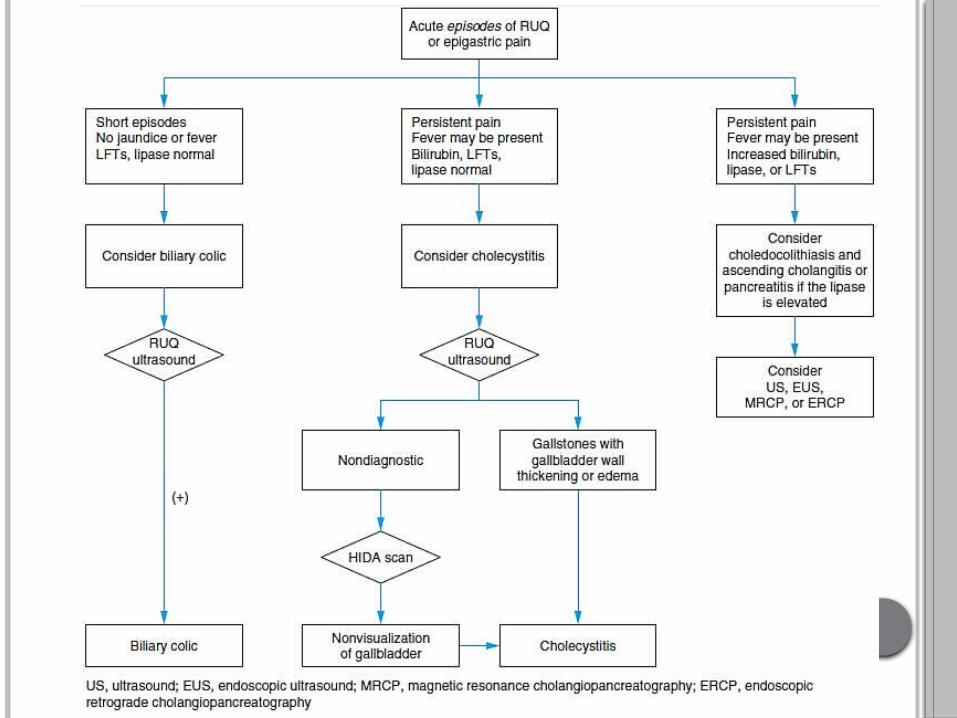
Source: Lange Symptoms to Diagnosis, 2nd ed. 2009
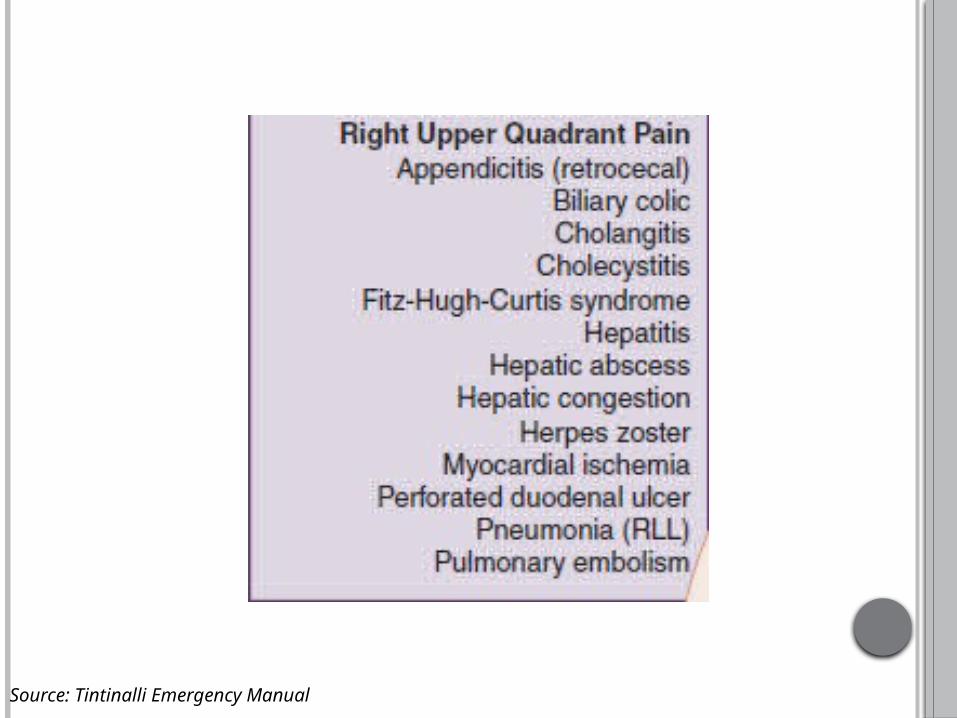
Source: Tintinalli Emergency Manual
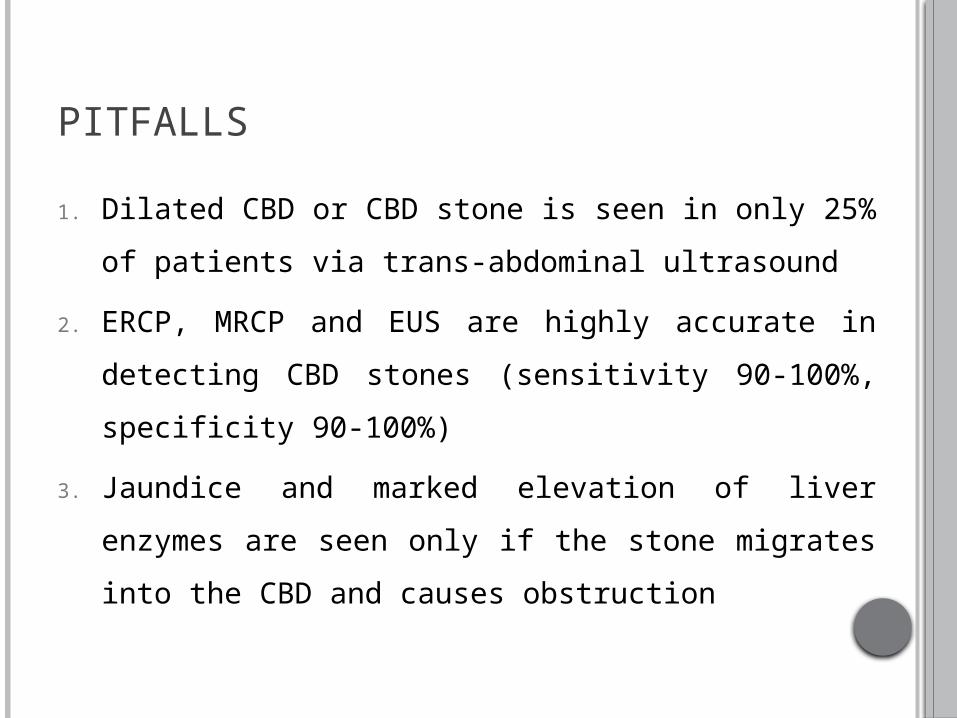
PITFALLS
1. Dilated CBD or CBD stone is seen in only 25%
of patients via trans-abdominal ultrasound
2. ERCP, MRCP and EUS are highly accurate in
detecting CBD stones (sensitivity 90-100%,
specificity 90-100%)
3. Jaundice and marked elevation of liver enzymes
are seen only if the stone migrates into the
CBD and causes obstruction

Source: Lange Symptoms to diagnosis, 2nd ed. 2009
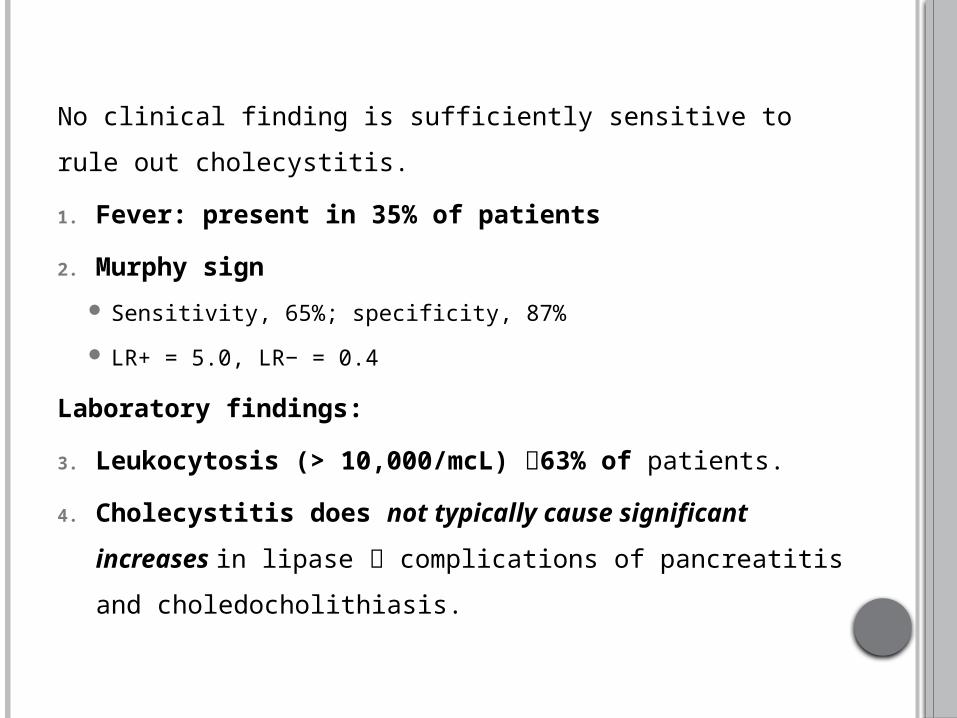
No clinical finding is sufficiently sensitive to rule out
cholecystitis.
1. Fever: present in 35% of patients
2. Murphy sign
Sensitivity, 65%; specificity, 87%
LR+ = 5.0, LR− = 0.4
Laboratory findings:
3. Leukocytosis (> 10,000/mcL) 63% of patients.
4. Cholecystitis does not typically cause significant
increases in lipase complications of pancreatitis and
choledocholithiasis.
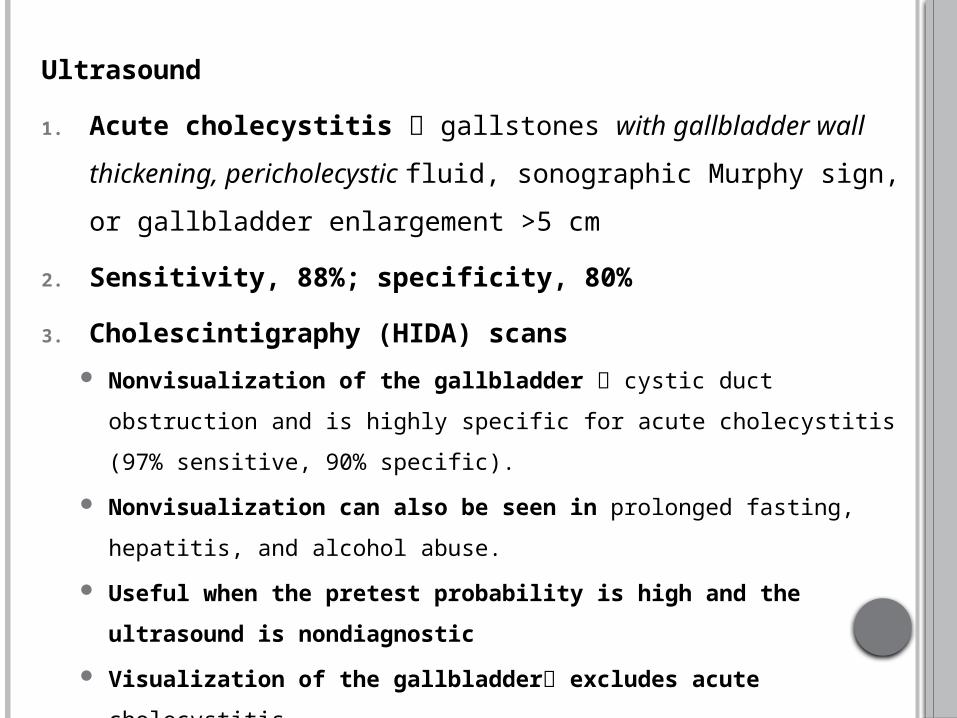
Ultrasound
1. Acute cholecystitis gallstones with gallbladder wall
thickening, pericholecystic fluid, sonographic Murphy sign,
or gallbladder enlargement >5 cm
2. Sensitivity, 88%; specificity, 80%
3. Cholescintigraphy (HIDA) scans
Nonvisualization of the gallbladder cystic duct obstruction and
is highly specific for acute cholecystitis (97% sensitive, 90% specific).
Nonvisualization can also be seen in prolonged fasting,
hepatitis, and alcohol abuse.
Useful when the pretest probability is high and the
ultrasound is nondiagnostic
Visualization of the gallbladder excludes acute cholecystitis.

Source: UpToDate, Treatment of Acute Cholecystitis
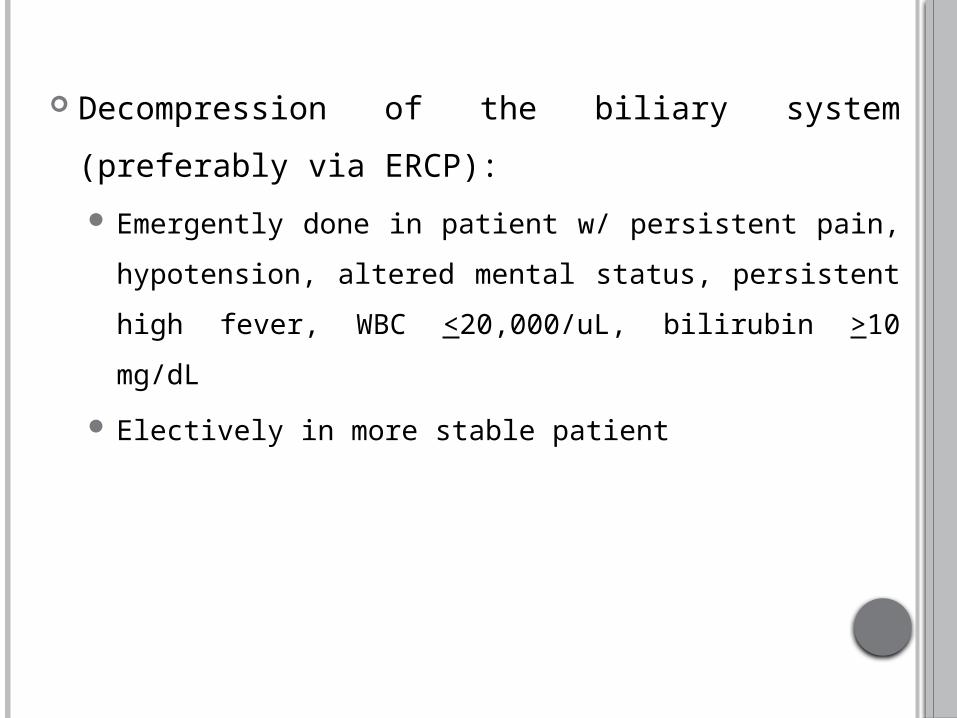
Decompression of the biliary system (preferably
via ERCP):
Emergently done in patient w/ persistent pain,
hypotension, altered mental status, persistent high
fever, WBC <20,000/uL, bilirubin >10 mg/dL
Electively in more stable patient

Source:Kaplan’s Clinical Hypertension (2010)

Source:
Kaplan’s Clinical Hypertension (2010)

PROGNOSIS
Quo ad vitam : dubia ad bonam
Quo ad sanationam : dubia ad bonam
Quo ad functionam : dubia ad bonam

THANK YOU