Embed Size (px)
Citation preview
- Dr Sujay IyerGeneral Medicine
Postgraduate student
Introduction Mechanism Cough Reflex Classification Dry Cough Epidemiology Etiology Management Algorithm Treatment Complications
Cough is an explosive expiration that provides a normal protective mechanism for clearing the tracheobronchial tree of secretions and foreign material.
It is one of the most common symptoms for which patients seek medical attention

Coughing may be initiated either voluntarily or reflexively.
It is a protective reflex serving a normal physiologic function of clearing excessive secretions and debris from the pulmonary tract.
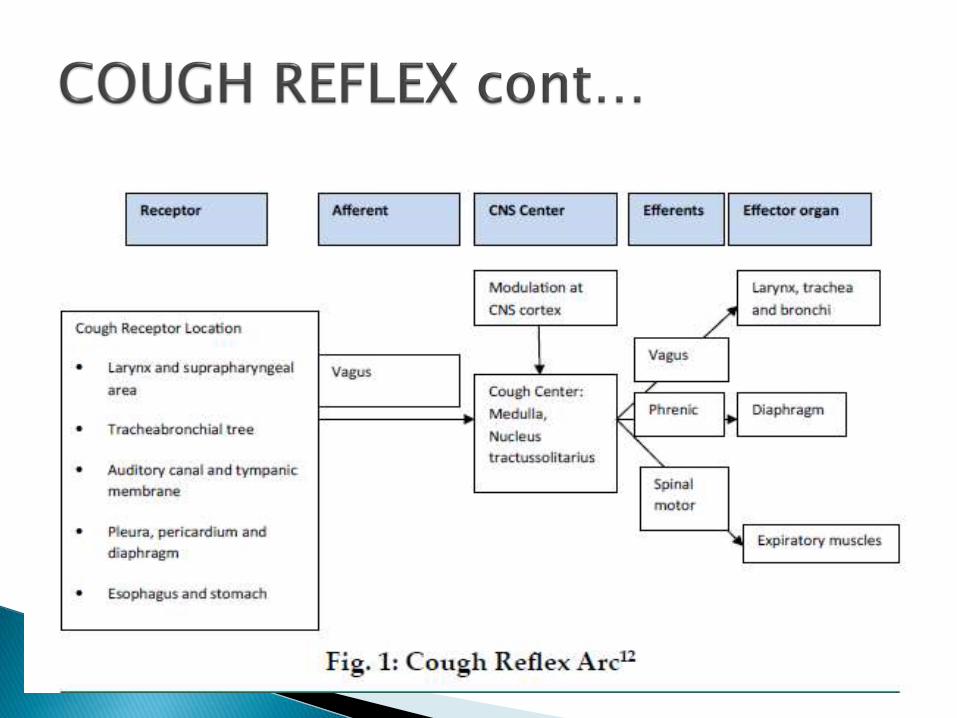
The Cough Reflex has three components:- Afferent Limb- Efferent Limb- Central Processing Center

Afferent Limb consists of the Vagus, Glossopharyngeal and Trigeminal nerves that supply pathways for cough receptors.
The Vagus Nerve, through its Pharyngeal, Superior Laryngeal and Pulmonary branches supply majority of the receptors.

Three types of Cough receptors are predominant:
- RARS (Rapidly Adapting Receptors)
- SARS (Slowly Adapting Stretch Receptors)
- C- Fibers Receptors are located throughout the airway
with greatest concentration in Larynx, Carina and bifurcation of larger bronchi.

The Afferent impulses are transmitted to the Cough Center located in the Nucleus TractusSolitarius in the Medulla Oblongata of the Brainstem which in itself is connected to the Central Respiratory Generator.

Efferents leave the Medulla and travel to the Larynx and the Tracheobronchial tree via the Vagus nerve while the Phrenic nerve and Spinal Motor nerves of C3 to S2 supply intercostal muscles, abdominal wall, diaphragm and pelvic floor.
Cough Reflex is considered neuroplastic.
Inspiratory Phase: Deep inspiration
Compression Phase: Closure of Glottis in combination with contraction of muscles of chest wall and diaphragm resulting in increased intrathoracic pressure.
Expiratory Phase: Opening of the Glottis resulting in high expiratory flow.
ACUTE (Less than 3 weeks)
SUBACUTE (3 to 8 weeks)
CHRONIC (More than 8 weeks)
Cough is also classified as - Productive cough- Non-productive (Dry Cough)
Our focus today is primarily going to be on Dry Cough.
Any cough that does not produce expectoration is termed as dry cough.
Usually, dry cough is chronic.
Up to 46% of patients with dry cough have unexplained etiology.
Patient presents with either cough as the only symptom or in collaboration with other symptoms.

According to one study (ERJ; WJ Song), dry cough affects 9.6% of the world population.
Another study tells us that dry cough affects 11 to 20% of the population (NEJM; RS Irwin).
The symptomatic burden of cough has been found to be reduced in India, 5%; although this needs to be further evaluated with greater in-depth study.
Supposed to affect Females more than Males.
RESPIRATORY NON-RESPIRATORY
Upper Airway Cough Syndrome Gastroesophageal Reflux Disease
Cough Variant Asthma ACE Inhibitor induced
Nonasthmatic Eosinophilic Bronchitis Psychogenic
Mediastinal Tumors Idiopathic
Pleural Disease Smoking
Early Interstital Fibrosis
Postinfectious induced
UACS, Asthma and GERD account for majority of the causes.
Recent research has brought up the term of Cough Hypersensitivity Syndrome.
Myriad of rhinosinus conditions that include:- Postnasal Drip Syndrome- Acute Bacterial Sinusitis- Allergic Fungal Sinusitis- Allergic Rhinitis- Nonallergic Rhinitis
Considered most common cause (87%) Mechanical stimulation of cough receptors in
the hypopharynx and larynx either directly or indirectly through inflammatory mediators is the mechanism.
Hallmarks of Asthma are variable airflow obstruction and airway hyperresponsiveness, which manifest as wheezing, dyspena and cough.
Cough occurs in al Asthmatics, and in a subset of patients with Cough-variant Asthma (CVA), it is the only presenting symptom.
Cough may be the sole clinical manifestation of GERD.
Two mechanisms have been postulated for GERD-associated cough:- Distal esophageal acid exposure that
stimulates cough reflex via Vagus nerve.- Microaspiration of esophageal contents.
Laryngopharyngeal Reflux or ExtraesophagealGERD does not manifest as traditional heartburn and tends to occur when patient is upright.
It is characterized by eosinophilic inflitrationof the bronchial tree as well as the absence of variable airflow obstruction and airway hyperresponsiveness.
Differs from Asthma in the localization of mast cells within the airway wall. Airway smooth muscle infiltration occurs in Asthma and epithelial infiltration in NAEB.
ACE Inhibitors
Smoking
Respiratory Causes: Usually present with complaints including dyspnea, wheezing and have significant radiographic findings.
Use of antitussives such as Codeine (opioid), Dextromethorphan (non-opioid), Levodropropizine (peripheral) is debatable as they have been shown to have limited or no efficacy in treatment of dry cough.
Use of Benzonatate may be helpful. Treatment with newer experimental options
such as Gabapentin and Amitriptyline is still under debate.
Cessation of smoking and use of ACE Inhibitors in patients.
Avoiding environmental irritants and offending antigens, treating sinusitis with antibiotics, and weaning patients off nasal decongestants for rhinitis. Allergy testing for allergic rhinitis.
Empiric therapy should be instituted with a combination of antihistamine and decongestants.
First generation antihistamines are more effective than newer less-sedating ones.
After undergoing spirometry and bronchoprovocation challenge, patients should be started on Beta-2 Agonists and Inhaled Corticosteroids.
Leukotriene Inhibitors and Oral Corticosteroids may also be instituted.
Inhaled Corticosteroids
Oral Corticosteroids for refractory cases.
Lifestyle modifications including limiting fat intake, avoiding caffeine, chocolate, mints, citrus products, alcohol and smoking.
Acid suppressive medications like Histamine 2 Blockers and Proton Pump Inhibitors.

Harrison’s Principles of Internal Medicine
Crofton and Douglas’s Respiratory Diseases
Physical Diagnosis - Vakil and Golwalla
Manual of Practical Medicine – R Alagappan
Supplement to Journal of the Association of Physicians of India
www.medscape.com
www.ncbi.nlm.nih.gov

Thank You!