Embed Size (px)
Citation preview

Presented by: Anvita
M. Pharm (IP)
What is drug targeting
The therapeutic response of a drug depends upon the interaction of drugmolecules with cell on cell membrane related biological events at receptorsites in concentration dependent manner.
Selective and effective localization of the pharmacologically-activemoiety at preidentified target(s) in therapeutic concentration, whilerestricting its access to non-target(s) normal cellular linings, thusminimizing toxic effects and maximizing the therapeutic index.
Target cell
Normal Cell
Normal Cell
Reasons for Drug Targeting
Drug instability
Low absorption
Short half-life
Large volume of distribution
Low specificity
Low therapeutic index

Common Approaches of Targeted Drug
Delivery
Controlling the distribution of drug by incorporating it in a carrier system
Altering the structure of the drug at molecular level
Controlling the input of the drug into bioenvironment to ensure a programmed and desirable biodistribution

Properties of Ideal Targeted Drug Delivery
Nontoxic, biocompatible and physicochemical stable in vivo and invitro.
Restrict drug distribution to target cells or tissue or organ or should have
uniform capillary distribution.
Controllable and predictable rate of drug release.
Minimal drug leakage during transit.
Carrier used must be biodegradable or readily eliminated from the body
without any problem.
Its preparation should be easy or reasonably simple, reproductive and
cost effective.

Important Properties Influencing
Drug Targeting
Drug Concentration, Particulate location and DistributionMolecular Weight, Physiochemical propertiesDrug Carrier Interaction
Carrier Type, Amount of Excipients, Surface Characteristics, size, Density
In Vivo Environment
PH, Polarity, Ionic Strength, Surface Tension, Viscosity, Temperature, Enzyme, Electric Field

Drug Targeting strategies
Passive Targeting
Inverse Targeting
ActiveTargeting
Ligand-mediatedTargetingPhysical
Targeting
DualTargeting
DoubleTargeting
CombinationTargeting

Passive Targeting
It utilizes the natural course of biodistribution of the carrier.
The colloids which are taken up by the reticulo-endothelial system(RES) can be ideal vectors for passive targeting of drugs to RESpredominant compartments.
Passive capture of colloidal carriers by macrophages offerstherapeutic opportunities for the delivery of anti-infective agents.
Inverse Targeting
It is a result of the avoidance of passive uptake of colloidal carriersby the RES.
It can be achieved by suppressing the function of RES by pre-junction of a large amount of blank colloidal carriers ormacromolecules like dextran sulphate.
Other strategies include modification and defined manipulation ofthe size, surface charge, composition, surface rigidity &hydrophilicity characteristics of carriers for desirable biofate.

Active Targeting
It involves the modification or functionalization of the drug carriers so that the contents are delivered exclusively to the site corresponding to which the carrier is architected.
Active targeting can be affected at different levels –1. First order targeting (organ compartmentalization)
2. Second order targeting (cellular targeting)
3. Third order targeting (intercellular organelles targeting)

Active Targeting
First Order Targeting
Second Order
Targeting
Third Order Targeting
Restricted distribution of the drug
carrier system to the capillary bed
of a pre-determined target site,
organ or tissue.
The selective drug delivery to a
specific cell type such as tumor
cells (& not to the normal cells)
Drug delivery specifically to the
intracellular organelles of the target
cells

Strategies for Drug Targeting
Ligand-mediated Targeting
Ligands are carrier surface group(s), which can selectively direct thecarrier to the pre-specified site(s) housing the appropriate receptorunits to serve as ‘homimg device’ to the carrier/drug.
Most of the carrier systems are colloidal in nature & can be specificallyfunctionalized using various biologically-relevant molecular ligandsincluding antibodies, polypeptides, oligosaccharides, viral proteins &fusogenic residues.
The ligands confer recognition & specificity upon drug carrier & endowthem with an ability to approach the respective target selectivity &deliver the drug

Examples of Ligands
Ligands Target Tumor targetFolate Folate receptor Overexpression of folate
receptorTransferrin Transferrin receptor Overexpression of transferrin
receptorGalactosamine Galactosamine receptors
on hepatocytesHepatoma
Physical Targeting
Characteristics of environment changes like pH, temperature, light intensity, electric field, and ionic strength.
This approach was found exceptional for tumor targeting as well as cytosolic delivery of entrapped drug or genetic material.

Physical Targeting
Physical Targeting Formulation System Mechanism for DrugDelivery
Heat Liposome Change in Permeability
MagneticModulation
Magnetically Responsive Microspheres Containing Iron oxide
Magnetic Field can retard fluid Flow of particles.
Ultrasound Polymers Change in Permeability
Electrical Pulse Gels Change in Permeability
Light Photo responsive Hydro gels Containing Azo-Derivatives
Change in Diffusion Channels, Activated by Specific Wavelength
Dual Targeting
In this targeting approach, carrier molecule,itself have their own therapeutic activity andthus increase the therapeutic effect of drug.
A carrier molecule having its own antiviral
activity can be loaded with antiviral drug
and for the synergistic effect of drug
conjugate.

Double Targeting
Spatial Control
Temporal
Control
Double Targeting
Targeting drugs to specific organs, tissues, cells or even sub cellular compartment
Controlling the rate of drug delivery to target site
Combination Targeting
These targeting systems are equipped with carriers, polymers and homing devices of molecular specificity that could provide a direct approach to target site.

Components for Drug
Targeting
Target
• Specific organ or a cell or group of cells, which in chronic or acute condition need treatment.
Carrier
• Special molecules or system essentially required for effective transportation of loaded drug up to the pre selected sites

Carriers
Liposomes
Microspheres
NanoparticlesQuantum Dots
Dendrimers
Nanoerythrocytes
Resealed Erythrocytes

Targeted NanoparticlesPlatform Targeting ligand Drug Stage
PEGylated liposome F(ab ¢ ) 2 fragment of humanantibody GAH
Doxorubicin Phase I
NGPE liposome Transferrin Oxaliplatin Phase I/II
Liposome Single-chain antibody fragment p53 gene Phase I
PEGylated PLGA NP Peptide Docetaxel Phase I
Applications of Resealed Erythrocytes
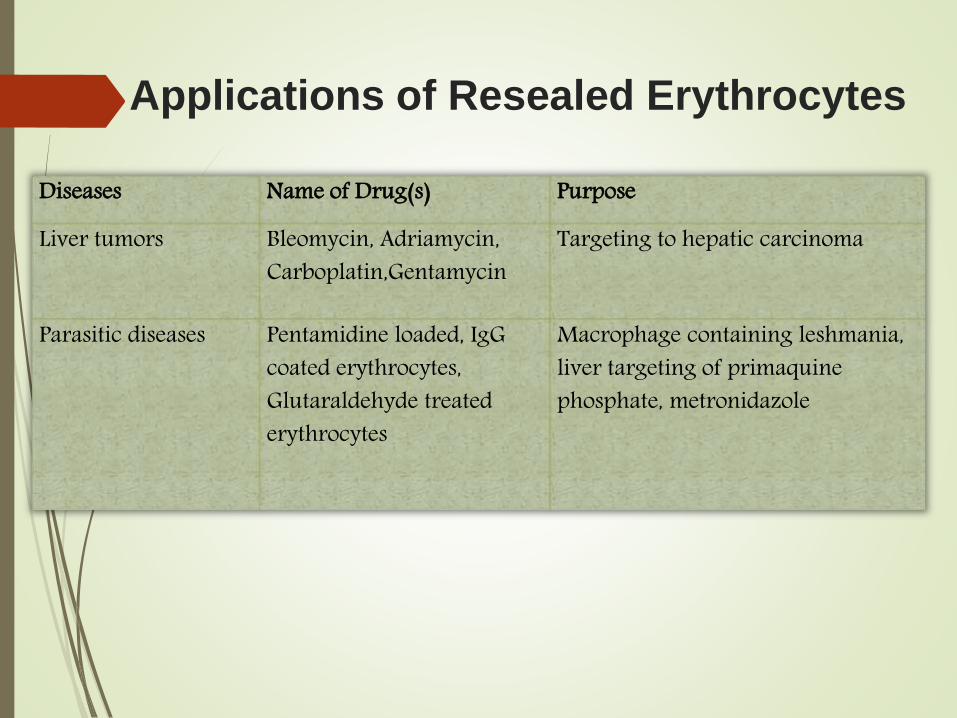
Diseases Name of Drug(s) Purpose
Liver tumors Bleomycin, Adriamycin, Carboplatin,Gentamycin
Targeting to hepatic carcinoma
Parasitic diseases Pentamidine loaded, IgGcoated erythrocytes, Glutaraldehyde treated erythrocytes
Macrophage containing leshmania, liver targeting of primaquinephosphate, metronidazole

Other Approaches of Drug
Targeting
1. Magnetically modulated drug targeting
2. Monoclonal antibody based targeted drug delivery
3. Prodrug

Magnetically modulated drug targeting
An interesting approach of targeting carrier system has been tomagnetize the carrier so that these particles can be retained at orguided to the target site by the application of an external magneticfield of appropriate strength.
Retention of magnetic carrier at the target site will delayreticuloendothelial clearance, facilitate extravasation & thus prolongthe systemic action of drug.

Magnetic Drug /Carrier Circulation
Major Pathway
Minor Pathway
RES Organs( liver/spleen/ bone
marrow)
N
S
Target Tissues
Principle of Magnetic Drug Targering

ADVANTAGES
Therapeutic responses in target organs at only 1/10th of the free drug dose.
Controlled drug release within target tissues for intervals of 30 min to 30 h, as desired.
Avoidance of acute drug toxicity directed against endothelium & normal parenchymal cells.
Adaptable to any part of the body.
DISADVANTAGES
It is expensive
It needs miniaturized specialized magnet for targeting, advanced techniques for monitoring, & trained personnel to perform procedures.
Magnet must have relatively constant gradients, in order to avoid focal overdosing with toxic drugs.
A large fraction (40 – 60 %) of the magnetite, which is entrapped in the carriers, may be deposited permanently in target tissues.
Magnetic Drug Targeting

Magnetic microspheres
Magnetic nanoparticles
Magnetic liposomes
Magnetic emulsion
Magnetic resealed erythrocytes
Magnetic delivery systems

Monoclonal antibody based targeted
drug delivery
The recognition site for the monoclonal antibody should be located on thesurface of the cell.
The antibodies should have sufficient tumor tissue specificity.
The extent of localization of the antibody at the target site. Biodistribution ofthe drug–antibody conjugate in the body relative to that of the parentantibody.
Stability of the drug–antibody conjugates in blood.
The host toxicity of the conjugate. The conjugate must be biodegradable andnon-immunogenic. Drugs should be released upon interaction between thecarrier molecule and the cell.

Approved Monoclonal Antibodies
Antibody Target Indication
Trastuzumab HER2 Breast Cancer
Bevacizumab VEGF Lung Cancer
Cetuximab EGFR Colorectal carcinoma
Panitumumab EGFR Colorectal carcinoma
Immunoconjugates
The possibility of raising monoclonal antibodies against cell surface markers allowtumor site targeting discretely.
Many cytotoxic drugs have been conjugated with monoclonal antibodies. Theseconjugates have been used to study drug localization in tumors and modulation ofdrug toxicity. They have been found to be useful in the management of varioustypes of carcinomas.
The conjugation of antibodies developed against a specific tumor determinant withanother recognition component provides them dual specificity to target the drug ortoxin intracellularly.

Bispecific antibodies
The approach has been mainly suggested for immunotherapy ofimmunological disorders especially those related to lack of MHC restrictedrecognition by immune effectors cells.
Bispecific antibodies against tumor endothelium & tissue factors (theinitiator of the intrinsic pathway of blood conjugation) have also beenproposed for synergistic effects.
Immunotoxins
These are conjugates of antibody (Mab & Fab) fragments & toxins, in which cell binding moieties of the toxins are replaced with specific binding chain of the antibodies.
Advantages The naturally occurring toxins used have very specific biological pathways in
producing their cytocidal effects.
The cytotoxic activity of the toxin that is conjugated to the antibody does not involve any other secondary agent(s).
Theoretically, immunotoxins should not bind to non-malignant cells, and even if they do bind, the internalization of the agent should not be sufficient to neutralize the therapeutic effect.
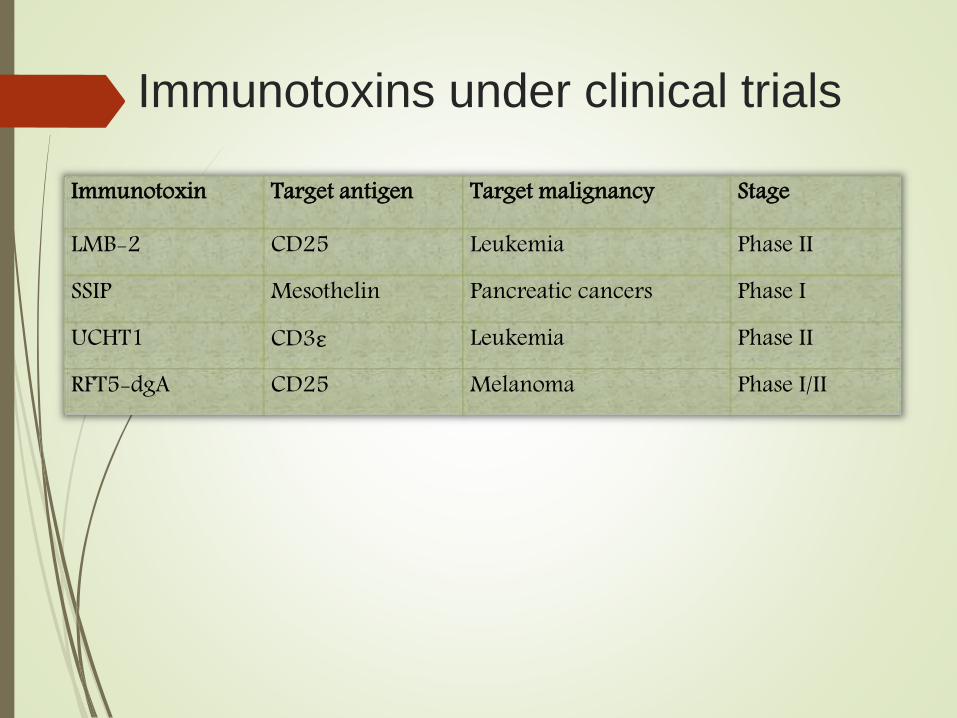
Immunotoxins under clinical trials
Immunotoxin Target antigen Target malignancy Stage
LMB-2 CD25 Leukemia Phase II
SSIP Mesothelin Pancreatic cancers Phase I
UCHT1 CD3ε Leukemia Phase II
RFT5-dgA CD25 Melanoma Phase I/II

Prodrugs
Prodrug is an inactive pharmacological moiety developed to optimizepharmacokinetics or site selectivity of a drug.
Since the prodrug has low cytotoxicity prior to its activation, it has very fewchances of its encounter with healthy cells.
In general, selective enzyme expression, hypoxia, & low extracellular pH at tumorsite is utilized for prodrug activation.
ADEPT has been investigated in the treatment of tumors, where an antibody-enzyme conjugate is administered systemically, where it clears from the circulation& localizes to its target by virtue of the antibody binding to its specific biomarkeron the tumor.

Enzymes & prodrugs used for ADEPT
Enzymes Prodrug ReactivityAlkaline Phosphatase Doxorubicin Hydrolysis of Phosphate Group
Etoposideβ lactamase Mitomycin Cleavage of Lactam Ring
Paclitaxel
Schematic representation of ADEPT

Conclusion
Targeted drug delivery essentially implies for selective and effective localization of the pharmacologically-active moiety at preidentified
target(s) in therapeutic concentration,
Various strategies such as active targeting, passive targeting etc. can be applied to achieve efficient drug targeting.
The targeted delivery is of great importance in cancer chemotherapy which always demands for reduction in adverse effect.
.

Reference:
Lachman/Lieberman’s The Theory and Practice of Industrial Pharmacy, Editors: Roop Khar, SP Vyas, Farhan Ahmad,Gaurav Jain, Chapter 25 Targeted Drug Delivery Systems, Pg. No. 907-943, 2014.
Lachman/Lieberman’s The Theory and Practice of Industrial Pharmacy, Editors: Roop Khar, SP Vyas, Farhan Ahmad,Gaurav Jain, Chapter 24 Novel Drug Delivery Systems, Pg. No. 872-906, 2014.
Mrs Jaya Agnihotri, Dr.Shubhini Saraf, Dr.Anubha Khale, Targeting : New Potential Carriers for Targeted DrugDelivery System, International Journal of Pharmaceutical Sciences Review and Research, Volume 8, Issue 2, Pg. No.117-123, May – June 2011.
Vidyavati S, Koppisetti and Sahiti. B, Magnetically Modulated Drug Delivery Systems, International Journal of Drug Development & Research, Vol. 3, Issue 1, Pg. No. 260 - 266, Jan-March 2011.
Priyanka Lokwani, Magnetic Particles for Drug Delivery: An Overview, International Journal of Research in Pharmaceutical and Biomedical Sciences, Vol. 2 (2), Pg. No. 465 – 473, Apr – Jun 2011.

R. Panchagnula and C. S. Dey, Monoclonal Antibodies in Drug Targeting, Journal of ClinicalPharmacy and Therapeutic, 22, Pg. No. 7 – 19, 1997.
Gupta Manish and Sharma Vimukta, Targeted drug delivery system: A Review, Research Journalof Chemical Sciences, Vol. 1 (2), Pg. No. 135 – 138, May 2011.
Archana Swami , Jinjun Shi , Suresh Gadde , Alexander R. Votruba , Nagesh Kolishetti , andOmid C. Farokhzad, Chapter 2 Nanoparticles for Targeted and Temporally Controlled DrugDelivery, Multifunctional Nanoparticles for Drug Delivery Applications: Imaging, Targeting,and Delivery, Nanostructure Science and Technology, Pg. No, 9 – 29, 2012.
Andrew M. Scott1, James P. Allison and Jedd D. Wolchok, Monoclonal Antibodies in CancerTherapy, Cancer Immunity, Vol. 12, Pg. No. 14 – 21, 2012.
Nurit Becker and Itai Benhar, Antibody-Based Immunotoxins for the Treatment of Cancer,Antibodies, 1, Pg, No. 39 – 69, 2012.
Tirupathi Rao K, Suria Prabha K and Muthu Prasanna, Resealed Erythrocytes: As a Specified toolin Novel Drug Delivery Carrier System, Research Journal of Pharmaceutical, Biological andChemical Sciences, Vol. 2, Issue 4, Pg. No. 496 – 512, October – December 2011.
Theresa M. Allen, Ligand-Targeted Therapeutics in Anticancer Therapy, Nature Review –Cancer, Vol. 2, Pg. No. 750 – 763, October 2002.






























