Embed Size (px)
Citation preview

FUNCTIONAL CAST BRACING & SPICA
DR.S.SENTHIL SAILESH
SENIOR ASSISTANT PROFESSOR
IOT MMC RGGGH

FUNCTIONAL CAST
• The concept of Functional cast bracing
was described in the early 18th century
• Sarmiento re-established the ideology
in late 60s
• It is a type of bracing where the limb is
allowed to do restricted function with
the brace in

PRINCIPLES
Continuing function while a fracture is uniting encourages
osteogenesis promotes the healing of tissues and prevents the
development of joint stiffness thus accelerating rehabilitation

PRINCIPLES
• Not merely a method of fracture reduction but an attitude
towards fracture healing.
• Requirements for fracture healing
• Stability
• Maintenance of reduction
• Blood supply

STABILITY
• Fluid is not
compressible
• Fascia cannot be
stretched beyond
the confines of the
cast
• “Hydraulic container
theory”; Sarmiento
et al 1974

LOADING
• Stability is maintained
by loading in a
functional cast
• Pressure & Load is
transmitted without
further deformation
• Rotation is restricted
by components of the
brace

MUSCLE CONTRACTION
Intermittent loading of the fracture area by muscle activity & weight bearing, promote local blood flow & development of electrical fields which are beneficial for healing
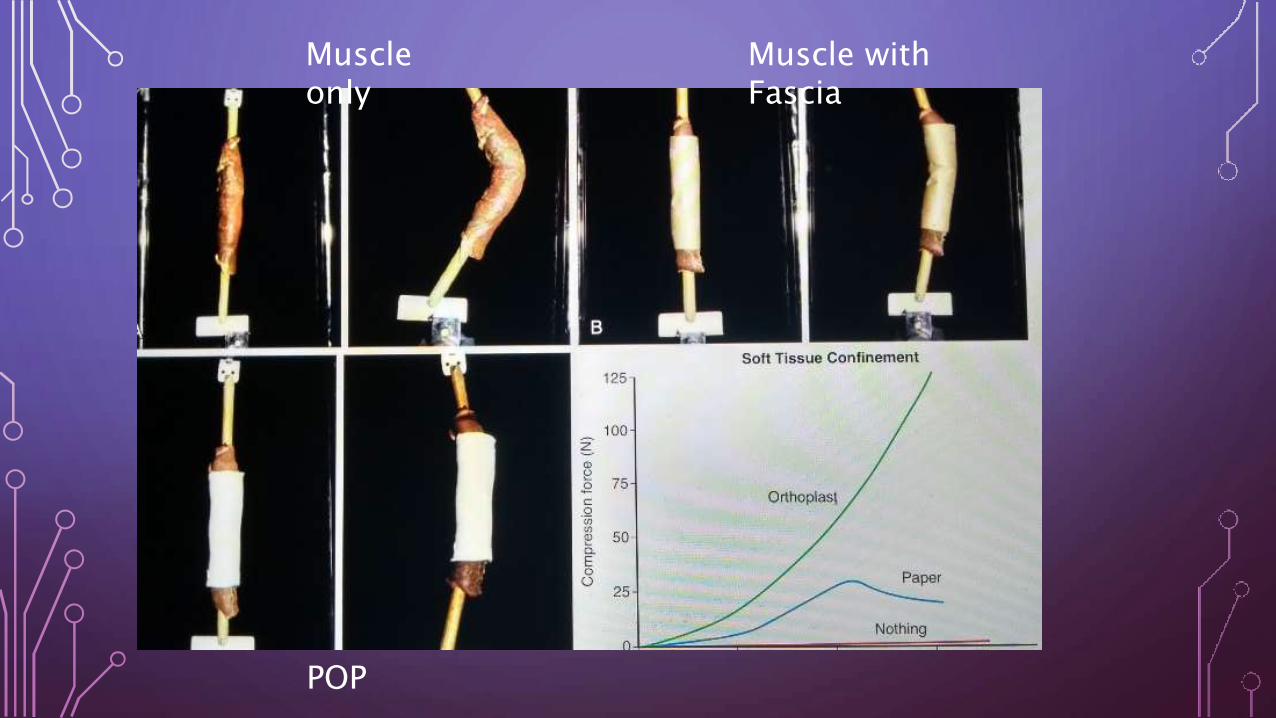
Muscle only
Muscle with Fascia
POP

BLOOD SUPPLY
Loading Contraction
of muscle
Micromotion
at # site
Increases
Blood supply
Bridging
callus

BRIDGING CALLUS & BLOOD SUPPLY

INDICATION
• All middle third shaft fractures and lower 3rd
junction fractures in long bones
in co-operative patients.

TIMING
• For # tibia following low energy injury, bracing can be done with in first 2 wks.
• High energy injuries with more pain & swelling needs an additional period of 1 or 2 more wks.
• For humerus fractures , most conditions bracing can be done by 7-10 days time.
• Median time of brace removal
• Tibia - 18.7 wks,
• Humerus - 10 wks.

TIME TO APPLY
• Fracture ends sticky
• Assess the # , when pain and swelling subsided
1. Minor movts at # site should be pain free
2. Any deformity should disappear once D.F removed
3. Reasonable resistance to telescoping.
4. Shortening should not exceed 6.0 mm for tibia, 1.25 cm for femur

CONTRAINDICATION
• Intraarticular fractures.
• Compound fractures
• Lack of co-operation by the pt.
• Patient with spastic disorders
• Bed-ridden & mentally incompetent pts.
• Deficient sensibility of the limb [D.M with P.N]
• Fractures of both bones forearm when reduction is difficult.

NOT USED IN
• Galeazzi fractures
• Monteggia fractures
• Proximal half of shaft of femur [tends to angulate in to varus
only used by expert]
• Isolated # of tibia, fibula
• Tends to cause varus angulation and to delay in consolidation
of #.

ACCEPTABLE REDUCTION
• 50% cortical contact
• <5-10* of varus / valgus angulation
• <10-15* of anterior / posterior bowing
• <5-7* of internal / external rotation
• Not more than 10-15mm of shortening

SARMIENTO CAST / PTB CAST - PRINCIPLE
• Described by Sarmiento
• Below knee cast extending to the upper pole of
the patella and with a firm moulding over the
medial flare of the tibia, the patellar tendon and
the popliteal space and shaped in a triangular
manner at the upper end of the tibia
• Knee free to move allowed early ambulation as
weight bearing forces should be transmitted
from the ground to the proximal end of tibia
bypassing fracture site

SARMIENTO CAST
Ending point
Starting point
Moulding area
Proximal patellar tendon
Tibial flares Patellar tendon Poplitela space
Metatarsal head

PTB



HUMERAL FCB

SPICA - DEFINITION
• A bandage folded into a spiral
arrangement resembling an ear
of wheat or barley.
• It is applied where
immobilisation is required at
areas where there is difference in
size

HIP SPICA
• Hip spicas are most commonly used to
• correct developmental hip dysplasia (DDH)
• children with hip, femur and pelvic fractures
• Other orthopaedic conditions which require
stabilization of the hip and leg.
Eg: Abduction Cast in Post THR dislocation
• Hips spicas are generally used for children
from 6 months to 6 years of age

Abdomial padding and space for breathing
Diaper Care

TYPES

POSITIONING
Proximal 1/3 frx:
- hip flexion 45 deg
- hip abduction 30 deg
- ext rotation 20 deg
Mid shaft fractures:- hip flexion 30
deg
- hip abduction 20
deg
- ext rotation 15
deg
Distal 1/3 frx:- hip
flexion 20 deg- hip
abduction 20 deg- ext
rotation 15 deg

COMPLICATIONS
COMPARTMENT SYNDROME
•decreased with
•applying smooth contours around popliteal fossa
•limiting knee flexion to < 90°
•avoiding excessive traction
•monitored for by observing the child's neurovascular exam
and level of comfort

MINERVA CAST

t
Diaphyseal
fractures
Initial POP for
2-4 weeks
Functional
casting done
Maintenance of
reduction
External
bridging callus
Loading &
Muscle
contration
Restoration of
vascularityFracture union

THANK YOU