Embed Size (px)
Citation preview
Donor hepatectomy

Apollo Medicine 2012 MarchReview Article
Volume 9, Number 1; pp. 17–23
© 2012, Indraprastha Medical Corporation Ltd
Donor hepatectomy
Rajesh Nambiar*, Neerav Goyal**, Subash Gupta***Transplant Fellow, Center for Liver and Biliary Surgery, **Consultant, Department of Surgical Gastroenterology and Liver Transplantation, Indraprastha Apollo Hospitals, Sarita Vihar, New Delhi – 110076, India.
ABSTRACT
Background: Living donor liver transplantation (LDLT) is performed all over the world today. The shortage of cadav-eric grafts makes it the only option for many end stage cirrhotics in many countries. Donor hepatectomy is a compli-cated operations and this has raised concerns about the safety of this operation. However, today donor hepatectomy is a safe operation with a low incidence of complications.
History: From the first living donor transplant performed in Brazil it has grown into a highly successful operation performed in many centers. The amazing regenerative capacity of the liver allows us to perform this operation with a good degree of safety. While increasing the donor pool the quality of the graft is also better.
Donor Selection: Selecting a donor for LDLT is a complex process with the aim of providing a graft that will benefit the recipient and at the same time not put the donor at risk. To be eligible the donor has to satisfy the donor criteria. Following this a potential donor has to undergo biochemical and radiological investigations that will assess the func-tional capacity of the liver and ensure a suitable anatomy.
The Operation: Today donor hepatectomy is a standardized operation performed with finesse is LDLT units. The complication rates are low and the success rates are high. The operation starts with a suitable incision and good exposure. The first step is a good cholangiogram. The liver is mobilized and the outflow is looped. The inflow vessels and isolated followed by parechymal transection.
Complications: Though, there are reports of a high incidence of complications in the initial years of LDLT the incidence has decreased. The morbidity and mortality of this operations in high volume LDLT units is extremely low. The most common complication are bile leaks (−8%) with overall morbidity of 12–16%.
Ethical Dilemma: As this is complex operation performed on a normal healthy adult there will always be questions about the ethics of this operation. However, the benefits to an end stage cirrhotic who has no chance of getting a cadaveric graft is unquestionable. The surgeon however has the responsibility to inform all donors and recipients of the potential risks of this operation.
Conclusion: Donor hepatectomy is a safe operations in high volume centers. It is a good option for end stage cirrhotics who find it difficult to get a cadaveric graft.
Keywords: Donor hepatectomy, living donor liver transplantation
Correspondence: Dr. Neerav Goyal, E-mail: [email protected]: 10.1016/S0976-0016(12)60115-X
In the early part of this century, man has attempted complex operations on the liver, but these attempts were hindered by its extensive vascularity. With advances in surgical and anesthetic techniques, progressively more complex opera-tions on the liver have been performed. Although kidney donation has become quite common, living donor liver transplantation (LDLT) is still restricted to some specialized centers due to the complexity of this operation. Donor safety
being paramount, selection of the donor needs experience as the anatomy of the liver is highly variable. Moreover, all the mysteries of the liver have not been revealed to us. There is still a large gap in our understanding of the meta-bolic functions of the liver. Due to the shortage of deceased donor livers and the absence of an organized organ sharing network in India and in most Asian countries, LDLT has emerged as the prime choice for most end-stage cirrhotics.
04-AMJ-RA-RN.indd 17 3/9/2012 6:19:02 PM

18 Apollo Medicine 2012 March; Vol. 9, No. 1 Nambiar et al
© 2012, Indraprastha Medical Corporation Ltd
Even in the United States and Europe where there are estab-lished transplant programs, the gap between the demand and the availability of deceased donor grafts continues to grow.
Hepatitis B affects about 2–7% of the Indian popula-tion. An estimated 40 million Indians are HBsAg carriers and of the 25 million infants born every year, over 1 million run a lifetime risk of getting infected. In addition, there are an estimated 12 million hepatitis C virus (HCV) carriers in India. Alcohol is a major cause of chronic liver disease in India. There are 14 million alcohol-dependent adults in India of who a large number go on to develop cirrhosis (Source: www.whoindia.org). An increasing number of patients with chronic liver disease put a heavy burden on the society and the only hope is to increase the donor pool by perform-ing living donor transplantation.
HISTORY
The first LDLT was performed in Brazil by Raia in 1987.1 Although the recipient did not survive, this paved the road for modern LDLT. The first successful LDLT was reported from Australia the same year by Strong2 and the technique was further refined by Broelsch at the Chicago Medical center.3 His first recipient Alyssa Smith transplanted in 1989 recently graduated from college in 2010. The credit for pioneering the first adult-to-adult liver transplants goes to the Japanese. The first successful adult-to-adult LDLT was done by the Shinshu group in 1993. A 53-year-old woman with primary biliary cirrhosis (PBC) received a left lobe graft from her son. Thus, began a new era in LDLT giving new hope to all those cirrhotics with no hope of get-ting a deceased donor graft.
While increasing the donor pool, the other advantages of living donor transplantation were that these grafts were healthier and the cold ischemia time was much less as com-pared with deceased donor grafts. The disadvantages being that this procedure required a perfectly normal individual to undergo a complex operation with its inherent risks. Today, the complications of the procedure have reduced but not eliminated.
The liver has amazing regenerating capacity allowing us to take up to 70% of the liver volume during a donor hepatectomy. This regenerative capacity of the liver has been described in Greek mythology 2500 years ago. Promethius was cursed by the gods to endure eternal pain for revealing the secret of fire to man. He was chained to Mount Caucasus and his liver eaten daily by the eagle of Zeus. He would not die as his liver regenerated only to be eaten again the next day (Figure 1).
DONOR SELECTION
Donor selection is a complex process involving a full hema-tological, radiological, and cardiopulmonary workup. There are two aspects to evaluation of a donor that proceed side by side. One focuses on making sure that taking the graft will not harm the donor and that it will be suitable for the recipi-ent. And the second is to ensure that the donor has no under-lying medical condition that will cause problems in the peri-operative period.
Candidates for donation:1. Age group 18–55 years.2. Healthy fit individual with no comorbidities.3. Compatible blood group.4. No active substance abuse.5. Predicted graft volume should be adequate.6. Favorable vascular and biliary anatomy.7. Approved by the ethics committee of the hospital.
RADIOLOGICAL INVESTIGATIONS
Plain Computed Tomography of
Abdomen
Measurement of the liver-attenuation index is the first step. This must be between +5 and +15. Donors outside this range are biopsied. This is arrived at by subtracting the liver density from the splenic density on a noncontrast scan. Less than +5 increases the chance of steatosis and more than +15 increases the chance of fibrosis.
Figure 1 Prometheus, chained to the rocky Mount Caucasus, has his liver eaten by the eagle of Zeus.
04-AMJ-RA-RN.indd 18 3/9/2012 6:19:02 PM

Donor hepatectomy Review Article 19
© 2012, Indraprastha Medical Corporation Ltd
Table 1 Donor evaluation protocol.
History(i) Age, (ii) blood group, and (iii) relationshipComorbidities/previous illnessSubstance abusePrevious surgery and allergies
Hematological workupComplete hemogram—Hemoglobin, platelet count, white blood cell countsLiver function test—Total/direct bilirubin, SGOT/SGPT, ALP/GGT, total protein and albumin, prothrombin time, and INRRenal function—Blood urea, serum creatinine, and electrolytesFasting lipid profile—Total cholesterol, triglycerides LDL/VLDLThyroid function tests—T3, T4, TSHFBS and HBA1c
Serology—HBsAg, anti-HCV, HIV I & II
Cardiopulmonary evaluationPulmonary—Chest radiograph, pulmonary function testCardiac—ECG, two-dimensional echo with pulmonary pressures, stress echo (if ≥40 yr)
Radiological investigationsUSG abdomen/pelvis with Doppler—Routine screenPlain CT abdomen—Liver-attenuation indexCT liver angiogram—Liver volumes, arterial, portal, and hepatic venous anatomyMRCP—Biliary anatomy
ALP: alkaline phosphatase; CT: computed tomography; ECG: electrocardiogram; FBS: fasting blood sugar; GGT: gamma-glutamyltranspeptidase; HBA1c: hemoglobin A1c; HBsAg: hepatitis B surface antigen; HCV: hepatitis C virus; HIV: human immunodeficiency virus; INR: international normalized ratio; LDL: low-density lipoprotein; MRCP: magnetic resonance cholangiopancreatography; SGOT: serum glutamic-oxaloacetic transaminase; SGPT: serum glutamic-pyruvic transaminase; T3: triiodothyronine; T4: thyroxine TSH: thyroid stimulating hormone; USG: ultrasonography; VLDL: very-low-density lipoprotein.
Figure 2 Plain computed tomography—measurement of leaf area index (LAI). Figure 3 Hepatic venous anatomy—the middle hepatic vein
and its tributaries. Note the drainage of the segment 4 veins.
Chest Tomography Liver Angiogram
This will delineate the hepatic arterial, portal, and venous anatomy of the liver. Of these, the hepatic arterial anatomy
is most variable. In case of a right lobe graft, the major area of interest is the drainage of segment 4 into the middle hepatic vein (MHV). This determines whether the MHV can be taken with the graft.
04-AMJ-RA-RN.indd 19 3/9/2012 6:19:04 PM

20 Apollo Medicine 2012 March; Vol. 9, No. 1 Nambiar et al
© 2012, Indraprastha Medical Corporation Ltd
Liver Volumetry
The approximate volume of the proposed liver graft and the volume of residual liver is measured on the computed tomog-raphy liver angio gram. The remnant liver should at least 30% of the total liver volume.
Once the volume of the proposed graft is measured, the graft recipient weight ratio (GRWR) is calculated. This should preferably be above 0.8 in living donor trans-plantation.
GRWR = Graft weight (g)
× 100Patient weight (g)
Figure 4 Portal venous anatomy.
Figure 5 Hepatic arterial anatomy. CHA: common hepatic artery; GDA: gastroduodenal artery; HAP: hepatic artery pseudoaneurysm; LHA: left hepatic artery; LT: liver transplantation; RHA: right hepatic artery.
Figure 6 Computed tomography volumetry.
Figure 7 Magnetic resonance cholangiopancreatography show-ing a type III biliary anatomy.
Table 2 Types of liver grafts.
Graft type Segments Hepatic vein taken
Right lobe graft Extended right 4–8 RHV/full MHV taken
lobe graft with graft Modified right 4–8 RHV/partial MHV
lobe graft with reconstruction Standard right 4–8 RHV/MHV not taken
lobe graft or reconstructed
Left lobe graft 2–4 LHV/MHV
Left lobe with caudate 1–4 LHV/MHV
Left lateral segment 2, 3 LHV
Monosegmental graft 2 or 3 LHV
LHV: left hepatic vein; MHV: middle hepatic vein; RHV: right hepatic vein.
04-AMJ-RA-RN.indd 20 3/9/2012 6:19:05 PM
Donor hepatectomy Review Article 21
© 2012, Indraprastha Medical Corporation Ltd
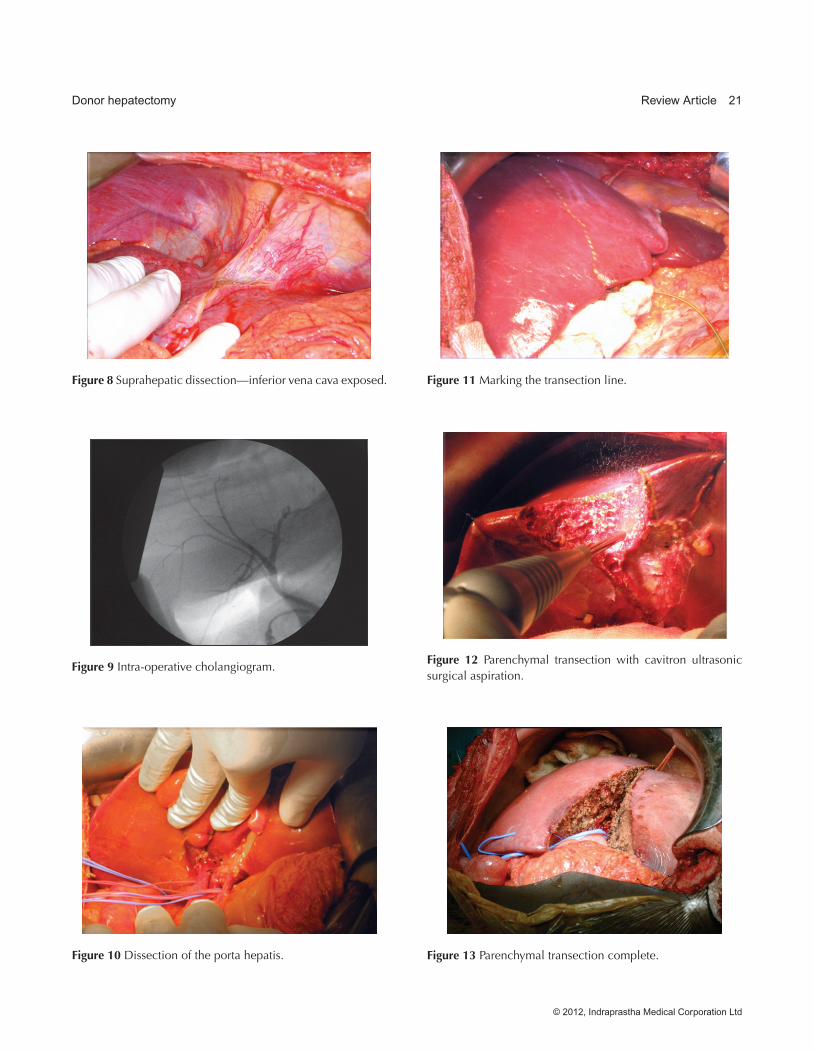
Figure 8 Suprahepatic dissection—inferior vena cava exposed.
Figure 9 Intra-operative cholangiogram.
Figure 11 Marking the transection line.
Figure 12 Parenchymal transection with cavitron ultrasonic surgical aspiration.
Figure 13 Parenchymal transection complete.Figure 10 Dissection of the porta hepatis.
04-AMJ-RA-RN.indd 21 3/9/2012 6:19:08 PM

22 Apollo Medicine 2012 March; Vol. 9, No. 1 Nambiar et al
© 2012, Indraprastha Medical Corporation Ltd
Magnetic Resonance Cholangiopancreatogram
This modality outlines the biliary anatomy. Several classifi-cations have been proposed of which the Huang classifica-tion is the most commonly used.
THE OPERATION
A self-retaining retracting system such as the Thompson retractor or the omnitract retractor should be available. Apart from the routine surgical instruments, a good vascular set with venous clamps and arterial bulldog clamps should be available. The anesthetic team proceeds with induction of the patient. An arterial line and a peripherally inserted central line are usually placed after induction. Deep vein thrombo-sis (DVT) prophylaxis is given with graduated compression pumps and stockings. Pressure point protection is essential and a body warmer is used to prevent hypothermia.
The incision used in our unit is a hockey stick incision (reverse L) which is basically a right subcostal incision with an upper midline extension. Once the retractor is applied, the part of the liver to be taken as the graft is mobilized.
The next step is cholecystectomy and intra-operative cholangiogram. The hilar plate is lowered and a clip is placed over the right hepatic duct just beyond the confluence. The intra-operative cholangiogram is probably the most impor-tant step of the operation and no effort should be spared in getting a good cholangiogram. This gives us the intrahepatic biliary anatomy and the anatomy at the confluence. The clip tells us where we should transect the bile duct. Abnormal biliary anatomy should be noted. Rarely, a biliary anomaly may force you to cancel the operation.
Next, the lobe to be taken as the graft is dissected off the inferior vena cava (IVC) and all caudate veins ligated. The end point of this part of the dissection is the looping of the hepatic vein of that side. If an inferior hepatic vein >5 mm is seen, it is preserved for reconstruction. Once the lobe is mobilized, the porta hepatis is dissected. The branch of the hepatic artery and portal vein to that lobe is mobi-lized and looped. No attempt is made to loop the bile duct at this stage. Bulldog clamps are applied to the artery and portal vein; then, the transection plane appears which is marked.
The parenchyma is divided with a cavitron ultrasonic surgical aspiration (CUSA) device. The MHV is looped intrahepatically during the transection.
The graft is removed in the following sequence: divide the bile duct, then heparinize and ligate-divide the hepatic artery. Clamp and divide the portal vein branch on the side of the graft. All that remains are the hepatic veins. These are divided in sequence and the stumps oversewn. The graft is
removed and perfusion with cold preservative solution is started. The stump of the bile duct is oversewn, the hepatic artey stump transfixed, and the portal vein is oversewn.
Complications
Most donors have a smooth postoperative period and are ambulant by the fourth postoperative day. The overall mor-tality reported in literature for left lateral segment donors are 0.1–0.2%. For right lobe donors, the mortality is 0.2–0.5%.4 Under reporting of statistics is a major problem in LDLT.
While the overall morbidity rates are 12–16%, the real incidence of serious morbidity is low.5 Reported early com-plications are bleeding, bile leaks, intra-abdominal collection, wound sepsis, respiratory complications, and venous throm-bosis.6 Long-term morbidity is usually related to biliary complications.1 With proper preparation and care, the donor complications in major transplant centers are low. Only 0.5% of the donors require a blood transfusion. Biliary complica-tion rates are usually 4–8%. Long-term morbidity in the form of strictures occurs in 0.5–1% of donors.7 Pain and a feeling of tightness along the incision are common but temporary. Ninety-nine percent of donors are back to normal activity in 3 months.
Ethical Dilemmas
One of the issues with a donor hepatectomy is that a normal healthy individual is subjected to major operation. There is intense pressure on oneself when a loved one is unwell. Of concern is the fact that loved ones are willing to donate regard-less of the risk to themselves.8 In these situations, a simple informed consent is insufficient. Physicians have a duty to prevent individuals from taking this risk unless the chance of success is proportionately large. Of equal concern is the fact that family members may be under pressure to donate leading those who are reluctant to do so to feel coerced. Also, of concern is that this type of donation has the potential for making possible the buying and selling of organs, and hence the strict protocol of ethical committee clearance is followed.
CONCLUSION
Despite all concerns today, donor hepatectomy is a safe pro-cedure in expert hands. In India and most Asian countries, living donor transplantation remains the only hope for most patients with end-stage chronic liver disease. Although it is a major operation, our understanding of liver anatomy and the
04-AMJ-RA-RN.indd 22 3/9/2012 6:19:19 PM

Donor hepatectomy Review Article 23
© 2012, Indraprastha Medical Corporation Ltd
liver’s regenerative capacity has advanced to a point where major complications are unheard off.
REFERENCES
1. Raia S, Nery J, Mies S. Liver transplantation from live donors. Lancet 1989;2:497.
2. Strong RW, Lynch SV, Ong TH, Matsunami H, Koido Y, Balderson GA. Successful liver transplantation from a living donor to her son. N Eng J Med 1990;322:1505–15.
3. Broelsch CE, Emond JC, Thistlethwaite JR, Rouch DA, Whitington PF, Lichtor JL. Liver transplantation with reduced size donor organ. Transplantation 1988;45:519–24.
4. Florman S, Miller CM. Live donor liver transplantation. Liver Transplant 2006;12:499–510.
5. Lo CM. Complications and long-term outcome of living liver donors: a survey of 1,508 cases in five Asian centers. Transplantation 2003;75:s12–5.
6. Hashikura Y, Makuuchi M, Kawasaki S, et al. Successful living-related partial liver transplantation to an adult patient. Lancet 1994;343:1233–4.
7. Sugawara Y, Makuuchi M. Advances in adult living donor liver transplantation: a review based on reports from the 10th anniversary of the adult-to-adult living donor liver trans-plantation meeting in Tokyo. Liver Transplant 2004;10:715–20.
8. Robert D, Truog MD. The ethics of organ donation by living donors. N Eng J Med 2005;353:444–6.
04-AMJ-RA-RN.indd 23 3/9/2012 6:19:19 PM

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/