Embed Size (px)
Citation preview

DISEASES OF THE OVARIES
NAME: HERMAN NDJAMENGROUP: 305

PLAN
• Histological structure of normal ovary• Classification of Ovarian Diseases• Features of Each Diseases • Possible Complications

The ovary has three main histologic compartments: (1) the surface müllerian epithelium (2) the germ cells (3) the sex cord–stromal cells.

CLASSIFICATION OF OVARIAN DISEASES
OVARIAN DISEASES
PRIMARY INFLAMMATORY
DISORDER
TumorsFunctional cysts

I- PRIMARY INFLAMMATORY DISORDER (Autoimmune Oophoritis)Definition: Autoimmune oophoritis is an autoimmune inflammation of ovaries resulting in their destruction, atrophy, and fibrosis. It is a rare disease that causes premature ovarian failure (POF) in 10 percent of cases characterized by premature menopause before 40 years of age.
Pathogenesis: Autoimmune oophoritis is caused by presence of special autoantibodies (StCA) that react both against steroid-producing cells in adrenal glands and gonad as well.



OTHER FORMS AND COMPLICATIONS
OTHER FORMS:
• XANTHOGRANULOMATOUS OOPHORITIS• PARASITIC OOPHORITIS• BILATERAL CYTOMEGGALOVIRUS OOPHORITIS
COMPLICATIONS:
* PRIMARY AMENORRHEA (MENSTRUATION HAS NEVER OCCURRED), * SECONDARY AMENORRHEA (MENSTRUATION APPEARED AT PUBERTY BUT SUBSEQUENTLY STOPPED), * INFERTILITY * PRIMARY OVARIAN FAILURE

II- FUNCTIONAL CYSTSA- FOLLICULAR CYSTS Cystic follicles in the ovary are so common that they are considered virtually normal. They originate in unruptured graafian follicles or in follicles that have ruptured and immediately sealed.
Morphology: These cysts are usually multiple. They range in size up to 2 cm in diameter, are filled with a clear serous fluid, and are lined by a gray, glistening membrane.Granulosa lining cells can be identified histologically if the intraluminal pressure has not been too great. The outer theca cells may be conspicuous due to increased amounts of pale cytoplasm (luteinized). It may be associated with increased estrogen production and endometrial abnormalities.


B- LUTEAL CYSTS.These are cysts from which the granulosa cells have disappeared leaving a cyst surrounded by luteinized tissue.
MORPHOLOGY: The cysts are typically 2-3 cm in diameter lined by a rim of bright yellow tissue containing luteinized granulosa cells.There is continued production of progesterone that leads to menstrual impairment .
COMPLICATION: Rupture of the cyst may lead to peritoneal reaction

C- STROMAL HYPERTHECOSISAlso called cortical stromal hyperplasia, it is a disorder of ovarian stroma most commonly seen in postmenopausal women.MACROSCOPICALLY: The disorder is characterized by uniform enlargement of the ovary (up to 7 cm), which has a white to tan appearance on sectioning.
MICROSCOPICALLY: There is hypercellular stroma and luteinization of the stromal cells, which are visible as discrete nests of cells with vacuolated cytoplasm.

D- Polycystic ovarian disease (PCOD, SteinLeventhal syndrome)
Affecting 3% to 6% of reproductive-age women, the central pathologic abnormality is numerous cystic follicles, often associated with oligomenorrhea. Women with PCOD have persistent anovulation, obesity (40%), hirsutism (50%), and, rarely, virilism.
PATHOGENESIS: The initiating event in PCOD is not clear, but It is now believed that a variety of enzymes involved in androgen biosynthesis are poorly regulated in PCOD.
MORPHOLOGY: Macroscopically, the ovaries are usually twice normal size and have a smooth, gray-white outer cortex studded with subcortical cysts 0.5 to 1.5 cm in diameter. Microscopically, there is a thickened, fibrotic superficial cortex beneath which are innumerable follicle cysts associated with hyperplasia of the theca interna

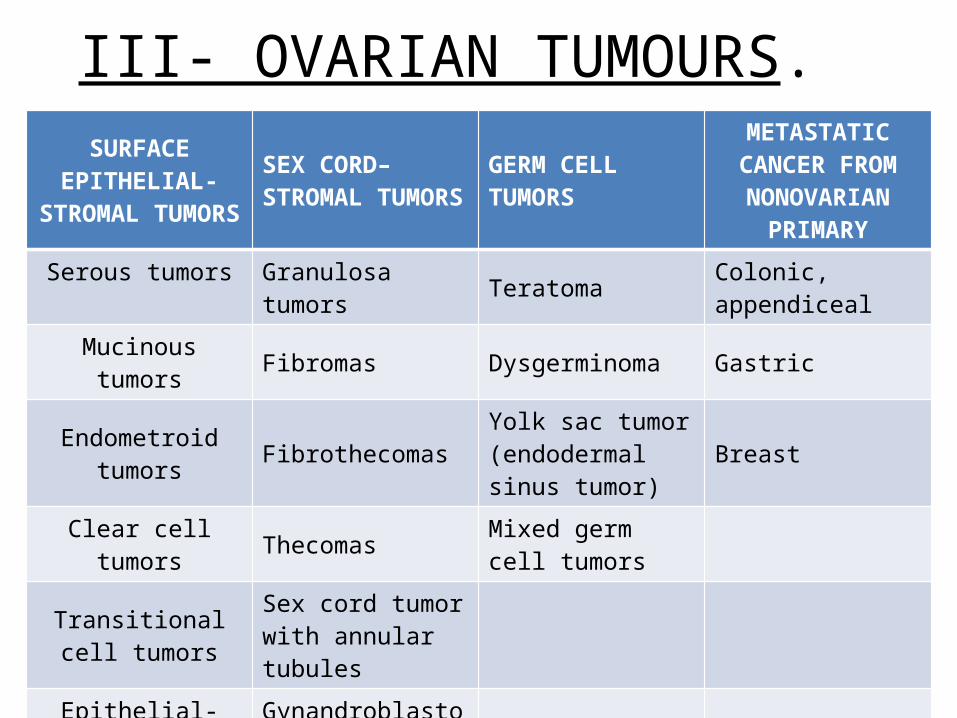
III- OVARIAN TUMOURS.SURFACE
EPITHELIAL-STROMAL TUMORS
SEX CORD–STROMAL TUMORS GERM CELL TUMORS
METASTATIC CANCER FROM NONOVARIAN
PRIMARYSerous tumors Granulosa tumors Teratoma Colonic, appendiceal
Mucinous tumors Fibromas Dysgerminoma Gastric
Endometroid tumors FibrothecomasYolk sac tumor (endodermal sinus tumor)
Breast
Clear cell tumors Thecomas Mixed germ cell tumors
Transitional cell tumors
Sex cord tumor with annular tubules
Epithelial-stromal Gynandroblastoma
Steroid (lipid) cell tumors

SEROUS TUMORS
These common cystic neoplasms are lined by tall, columnar, ciliated and nonciliated epithelial cells and are filled with clear serous fluid. They may be Benign, Borderline and malignant. Some examples of serous tumors are:
CYSTADENOMAS: Benign tumours which may include cystic areas
CYSTADENOFIBROMAS: containing cystic and fibrous areas
ADENOFIBROMAS: containing predominantly fibrous areas
CYSTADENOCARCINOMA: Malignant tumour containing cystic component
MUCINOUS TUMOURS
These types of tumours include:
- Benign and borderline Cystadenomas
- Primary mucinous Carcinomas

SEX CORD–STROMAL TUMORS
GRANULOSA–THECA CELL TUMORS:
Ovarian neoplasms composed of varying proportions of granulosa and theca cell differentiation.
FIBROMAS: Tumors arising in the ovarian stroma that are composed of fibroblasts
THECOMAS: Composed of plump spindle cells with lipid droplets.
FIBROTHECOMAS: Tumors containing a mixture of these cells

GERM CELL TUMORS
THANKS FOR YOUR ATTENTION





























