Embed Size (px)
Citation preview

Furunculosis
A boil (furuncle) is an infection of a hair follicle]
A carbuncle occurs when a group of hair follicles next to each other become infected

• Furunculosis is a localized form of otitis externa resulting from infection of a single hair follicle
• Bacterial invasion of a single hair follicle
well-circumscribed deep skin infection
Pustule local abscess formation• Associated cellulitis and oedema• Bacteria attach initially to the cells of
the stratum corneum and proliferate around the ostium of the hair follicle.
• There is deeper invasion of the hair follicle between the inner and outer root sheath

DIAGNOSIS• Symptoms do not usually discriminate furunculosis from severe diffuse otitis externa
• The affected ear is extremely painful, feels blocked and exudes a scanty serosanguinous discharge
• The pinna and tragus are tender on palpation

AETIOLOGY AND EPIDEMIOLOGY
• Staphylococcus aureus (S. aureus) is the most common organism
• leukocidal toxins commonly isolated from pathogenic strains of S. aureus trigger lysis of phagocytic cells and may have an important role in cutaneous infection.
• Recurrent furunculosis---Several conditions appear to be associated with recurrent furunculosis including hypogammaglobulinaemia, diabetes mellitus and dysphagocytosis.

• Repeated infection can cause permanent scarring and fibrosis of the external canal with subsequent meatal stenosis.
• Ultimately, this may also predispose to chronic diffuse otitis externa.

Treatment choices include:• Antibiotics• Topical treatment (antibiotics, astringents, hygroscopic dehydrating agents);• Incision and drainage• Oral antibiotic treatment is recommended in the early stages of the disease.• Severe spreading soft tissue infection should be treated with intravenous
antibiotic therapy• Abscess formation is an indication for formal drainage. After the abscess has
discharged, surgically or spontaneously, topical treatment is preferable.• Topical antibiotics active against staphylococcus are usually prescribed• Insertion of a wick into the ear canal facilitates treatment in the presence of
severe canal oedema and narrowing

• Glycerol and ichthammol solution has a specific antistaphylococcal action6, 7 and is hygroscopic, thus causing dehydration of the canal tissue.
• Aluminium acetate solution is an astringent as well as a hygroscopic agent.

For patients suffering generalized recurrent furunculosis
• Eradication therapy with nasal mupirocin.• Eradication therapy with oral flucloxacillin for 14 days.• Bacterial interference therapy: deliberately implanting a nonpathogenic strain of S. aureus(strain 502A is the most popular) to recolonize the nares and skin.
• It has been reported that correction of specific biochemical abnormalities (e.g. hypoferraemia, low serum zinc) may lead to a marked reduction in the frequency of infections.

Bullous myringitis
• Bullous myringitis (myringitis bullosa haemorrhagica) is the finding of vesicles in the superficial layer of the tympanic membrane
The vesicles occur between the outer epithelium and thelamina propria of the tympanic membran

AETIOLOGY
• Influenza virus or by Mycoplasma pneumoniae (No evidence for this)• occurs in all age groups

SYMPTOMS
• Sudden onset of severe• usually unilateral• often throbbing pain in the ear is the most common presentation
• The symptoms usually set in during or following an upper respiratory tract infection
• A bloodstained discharge can be present for a couple of hours
• A hearing impairment (conductive and/or sensorineural) is common in the affected ear.

SIGNS• Otoscopy— blood-filled, serous or serosanginous blisters involving the tympanic membrane Serosanginous secretion can be seen if the blisters rupture
The tympanic membrane is intact• In young children with bullous myringitis, middle ear fluid was present in the majority (97 percent) but is an uncommon finding in other age groups.
• The site of the sensorineural hearing loss is the cochlea; however, the pathogenic base is not understood.

DIAGNOSIS
• based on physical examination.• Vesicles in the superficial layer of the TM.• The main differential diagnoses Acute otitis media, Herpes zoster oticus orRamsay Hunt syndrom

Investigations• Inspection of the ear using a microscope is essential for diagnosis.• Pneumatic otoscopy and tympanometry help determine whether the middle ear contains fluid
• Clinical evaluation of the cranial nerves and, in particular, the facial nerve must be carried out for to distinguish from herpes zoster oticus or Ramsey Hunt syndrome
• Pure-tone audiogram• Cultures from blisters are not necessary in the management of uncomplicated cases
• A serologic sample for herpes zoster is of value in cases with sensorineural hearing loss and may be of help in the differential diagnosis

OUTCOMES
• In the vast majority of cases a complete recovery is seen within days.
• a sensorineural hearing impariment of more than 15 dB in two frequencies was reported in 65 percent of 18 patients referred to an ENT clinic for bullous myringitis.

MANAGEMENT OPTIONS• In cases without middle ear affection and without sensorineural
hearing loss only analgesics are recommended.
• When the middle ear is affected antibiotics can be used as in the treatment of acute otitis media.
• In children less than two years of age, acute bullous myringitis should be treated as acute otitis media.
• in cases with sensorineural hearing impairment- Antibiotics have also been recommended

Effect of management
• Spontaneous resolution of the blisters and middle ear effusion, if present, is the norm.
• Complete recovery of the sensorineural impairment within three months occurred in between 60 and 100 percent of affected patients treated with amoxicillin.
(this study was not controlled)

Granular myringitis
Granular myringitis is a specific form of external otitis.
It is characterized by granulation tissue on the lateral aspectof the tympanic membrane with possible involvement ofthe external ear canal.
various names Granulating myringitis, Myringitis granulosa,Otitis externa granulosa,Otitis externa with granulations, Granulomatous otitis externa,Granulomatous myringitis,Acute granulomatous myringitis,Chronic myringitis




PATHOLOGY
• Microscopic examination--oedematous granulation tissue with capillaries and diffuse infiltration of chronic inflammatory cells
• Large areas of the granulation tissue have no covering epithelium
• It has been suggested that a nonspecific injury involving the lamina propria of the tympanic membrane suppresses epithelialization which leads to the development of granulation tissue.

AETIOLOGY• Not related to sex, age, systemic disease or season.• High-ambient temperature, swimming, lack of hygiene, local irritants and foreign bodies have all been suggested as causative factors.
• Bacterial and sometimes fungal infection is present in the affected ear in all reports.
• The incidence of granular myringitis has been calculated to be a quarter of that of cholesteatoma
• Granular myringitis is also occasionally seen as a postoperative complication of tympanic membrane grafting.

SYMPTOMS
• Foul-smelling discharge from the affected ear.• There is usually little or no pain.• Some individuals have a sensation of fullness or irritation in the ear.
• The hearing is either not at all or only slightly impaired.
• Associated tinnitus is uncommon. Some patients can be asymptomatic.

SIGNSA moderate amount of purulent secretion is seen in the affected ear .3 The tympanic membrane is covered with secretions that sometimes crust.
After aural toilet the granulation tissue is revealed.
localized form of granular myringitis:most commonSmall areas of the drum are affectedone or more polyps are present
Most commonly, the granulations aresituated posterosuperior on the eardrum and may affect the adjacent canal wall.
Diffuse form:slightly raised carpet of granulations, which covers the tympanic membranePerforation of the tympanic membrane is not present

DIAGNOSIS
• Discharge from the ear is present.• Inflammation and granulation tissue are seen on the lateral aspect of the tympanic membrane with possible involvement of the external ear canal.
• Differential diagnoses: chronic (suppurative) otitis media and diffuse external otitis
• The lack of a conductive hearing impairment and a normal computed tomography (CT) scan excludesm chronic otitis media

Investigations• Microscope• Pneumatic otoscopy and tympanometry should be used to confirm that the middle ear is normal and no perforation is present.
• Pure-tone audiometry should be performed to exclude a conductive hearing impairment due to chronic otitis media.
• Culture:Gram-negative bacteria (Pseudomonas aeruginosa, Proteus species and Staphylococcus aureus) and Candida albicans are most commonly cultured.
The bacterial culture does not differ from specimens found in external otitis and chronic otitis media.
• If there is doubt as to whether the middle ear and mastoid is involved, a high resolution CT scan can help exclude chronic otitis media
• If the granulations do not resolve with treatment, biopsy for histological examination should be carried out to exclude carcinoma
OUTCOMES, NATURAL HISTORY ANDCOMPLICATIONS
• Many patients are asymptomatic• Granular myringitis has a chronic course and granulations may continue to grow slowly for years ,however, healing may happen spontaneously.
• The inflammation in the epithelial layer and lamina propria of the tympanic membrane sometimes leads to replacement with proliferating granulation tissue, fibrosis and an atresia forming from the medial part of the ear canal.
• When the fibrosis and atresia has extended laterally, the atresia ceases to grow.

MANAGEMENT OPTIONS

• Topical treatment with ear drops containing steroids and antibiotic and/or antifungal agents based on the results from the culture should be given
• The treatment should be continued for a longer period than in otitis externa.• Various antiseptic agents have been employed, but none of them have been evaluated in a controlled way.
• A solution of 0.5 percent formalin or trichloroacetic acid applied once a week has been given, with good results
• Strong caustic agents may harm the fibrous middle layer of the eardrum and should be avoided.
• Removal of granulations by physical methods should be considered if conservative treatment fails.
• If a perforation does happen, immediate repair with the temporalis fascia should be carried out.

Effect of management
• variable

Benign necrotizing otitis externaBenign necrotizing otitis externa is the clinical condition of idiopathic necrosis of a localized area of bone of the tympanic ring, with secondary inflammation of the verlying soft tissue and skin
OTHER NAMES--
•Benign necrotizing otitis externa;•Benign necrotizing osteitis of the external auditory meatus canal;•Benign osteonecrosis of the external auditory meatus;•Aseptic necrosis of the external auditory meatus;•Idiopathic tympanic bone necrosis;•Necrosis and sequestration of the tympanic bone;•Necrosis and sequestration of the tympanic part of the temporal bone;•Focal or circumscribed osteonecrosis of the external auditory meatus.



Malignant otitis externaMalignant otitis externa is an aggressive and potentially life-threatening infection of the soft tissues of the external ear and surrounding structures, quickly spreading to involve the periostium and bone of the skull base.










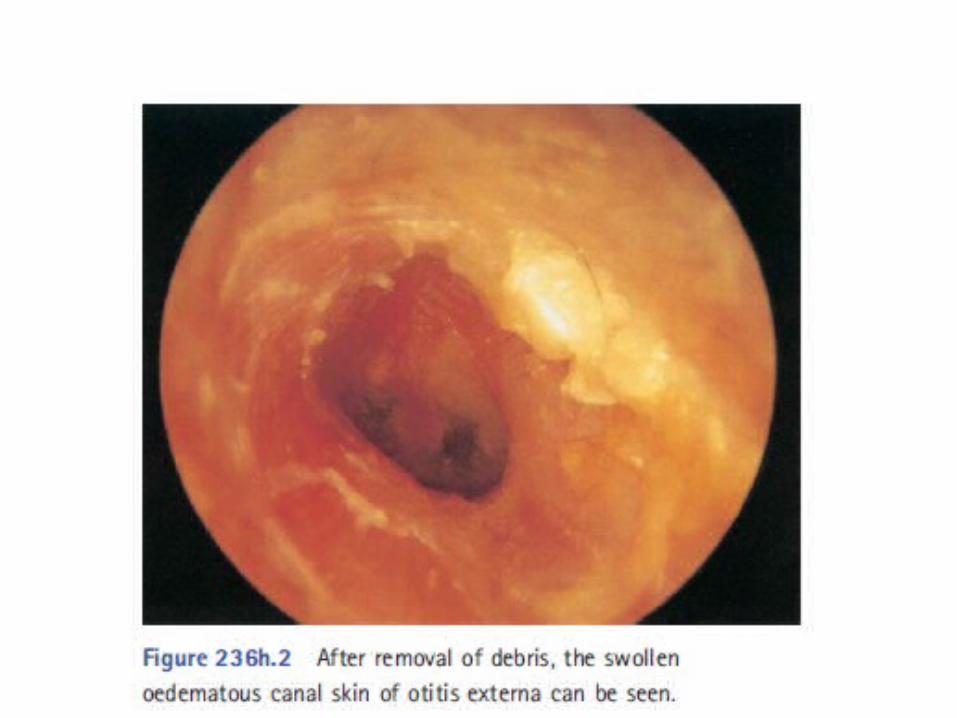
Otitis externa

Fungal otitis externa




otomycosis


aspergillosis

Candida albical

Aspergillus fumigatus

otomycosis

Perichondritis of external ear



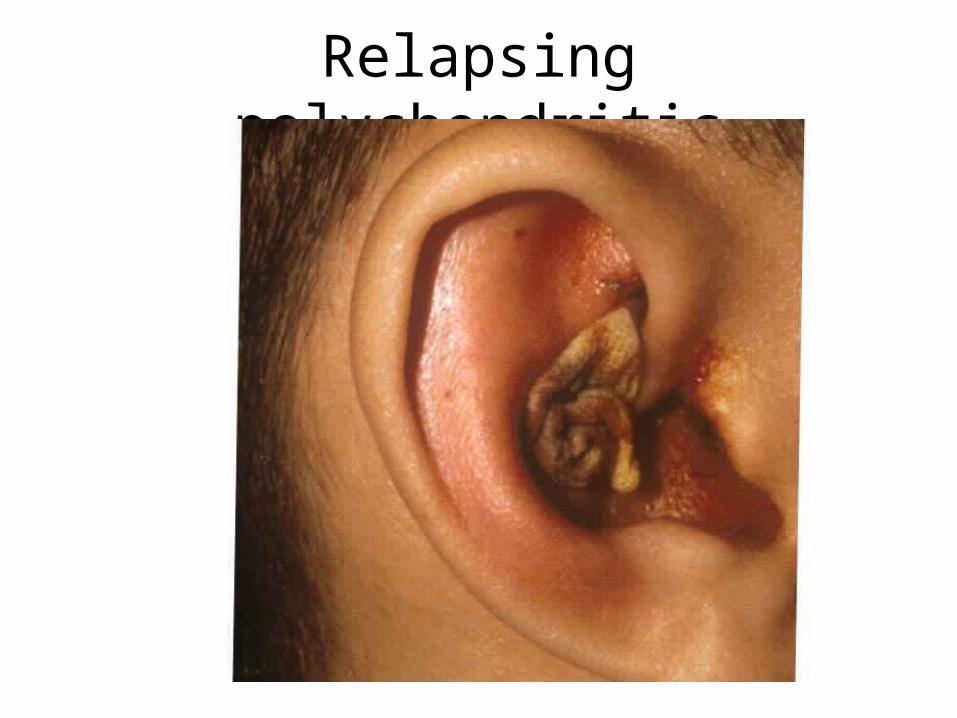
Relapsing polychondritis


Exostosis of external auditory canal

































