Embed Size (px)
Citation preview

1
Dermatophytes infections
اللطيفعبد ناهض .أ
الشفاء.م-الميكربيولوجىرئيس قسم

2
Abstract• Diagnosis of dermatophytes infections
using two methods:
• 1-Direct microscopic examination (KOH
method)
• 2-Fungal culture on sabouraud dextrose
agar with antibiotics).

3
Introduction• Dermatophytes are fungal organisms that are able
to exist within the keratinous elements of living
skin and which belong to one of 3 genera,
Epidermophyton Microsporum,and
Trichophyton.
• Dermatophytes require keratin for growth and
therefore infect hair, nails, and superficial skin,
with clinical manifestations named for the area
affected.

4

5
• Dermatophytoses occur in all populations
worldwide, but are generally more common among
immunocompromised patients.
• Tinea infections have alternately been called
“ringworm,” because of the lesions that present as a
circular or oval clearing surrounded by a red, scaly,
elevated border (“ring”).

6
• Besides the dermatophytoses,
superficial infections may also result
from infection with other fungi,
including the Malassezia species of
yeast, and candida.
7
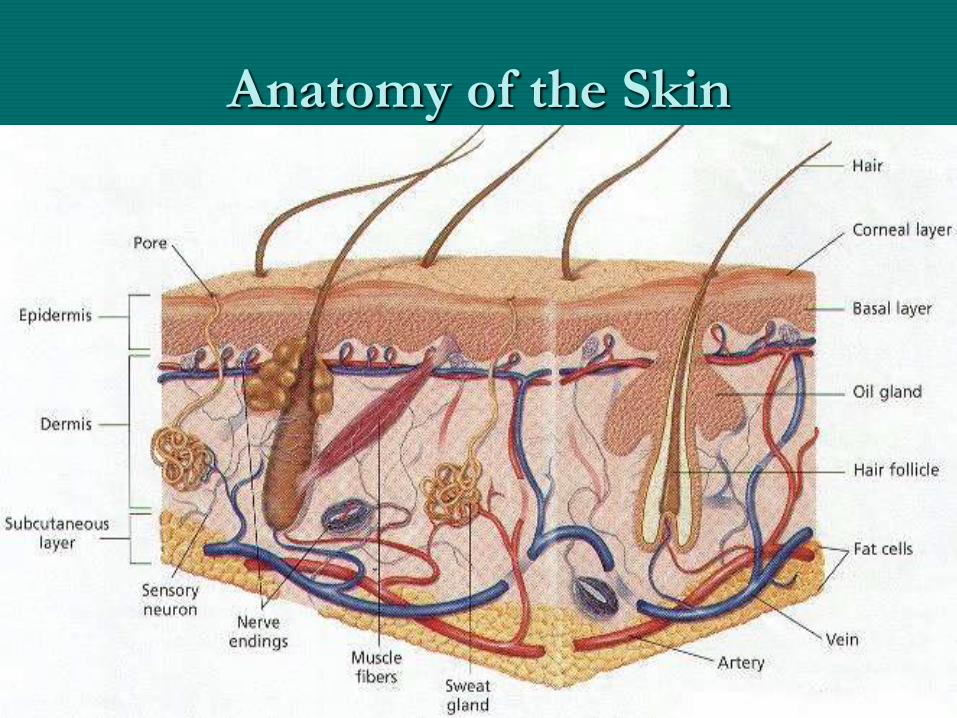
Anatomy of the Skin

8
Epidermis
• Outermost layer of the skin
• Its layers are made of Mostly dead cells.
• Most of the cells of the epidermis undergo rapid
cell division (mitosis).
• As new cells are produced, they push older cells
to the surface of the skin. The older cells
become flattened, lose their cellular contents and
begin making keratin.
• Keratin:- a tough fibrous protein that forms the
basic structure of hair, nails, and skin.

9
Layers of Epidermis

10
Hair Follicles

11
Nails

12
ETIOLOGIC AGENTS• Three fungal genera cause tinea infections:
Microsporum, Trichophyton, and more rarely,
Epidermophyton .
• Species may be grouped by their source of
human infection
• 1-Anthropophilic:from human, the most
frequent causes of onychomycosis and other
superficial dermatophytoses
• 2- Zoophilic:from animals, especially dogs, cat.
• 3- Geophilic: from soil, less commonly,

13
Zoophilic dermatophytoses

14
Zoophilic dermatophytoses

15
Zoophilic dermatophytoses

16
• The major causative species differ geographically and may change in prevalence over time owing to population movements from immigration or travel.
• M. canis is a zoophilic organism frequently picked up by humans from contact with animals such as dogs and cats.
• The Malassezia yeast species are associated with the superficial fungal infections pityriasis (tinea) versicolor (PV) and seborrheic dermatitis (SD).
17
PATHOGENESIS AND
IMMUNOLOGY
• The dermatophytes colonize keratinized tissue
of the stratum corneum; invasion by
anthropophilic species usually result in less
inflammation than that of zoophilic or geophilic
species.
• The epidermis functions as a barrier to
microorganisms, and commensal flora may also
help reduce infection by pathogens .
18
• Entry into the stratum corneum may result from
trauma to the skin or some other breach of the
skin barrier.
• Excessive sweating and occlusive clothing
/footwear aid in providing a warm, moist
environment conducive to tinea infection.
Infection may be transferred from one area of
the body to another. Infection may also be
transmitted between individuals by direct or
indirect contact with scales containing fungal
arthroconidia from infected individuals

19
CLINICAL MANIFESTATIONS• 1-Tinea Pedis :
• Tinea pedis is dermatophytoses of the feet, and may
involve the interdigital spaces.
• Tinea pedis is also called athlete’s foot and ringworm
of the feet.
• There are three common presentations recognized in
tinea pedis: interdigital, moccasin, and vesicobullous
• This infection is most commonly produced by T.
rubrum and T.mentagrophytes.
• Secondary bacterial or yeast infection is also possible.

20

21
Tinea Manuum• Tinea manuum is a rare form that primarily
affects the palmar areas of the hands, and
presents as chronic, dry, scaly, hyperkeratotic
skin with minimal erythema .
• Infections are most frequently caused by T.
rubrum. Tinea manuum may accompany tinea
pedis or onychomycosis, and a two feet–one
hand syndrome has been noted to occur .

22

23
Tinea Corporis• Tinea corporis is a superficial dermatophyte infection
of the glabrous skin, excluding the scalp, beard, face,
hands, feet, and groin.
• Infection of the skin of the trunk, legs and arms with
a dermatophyte.
• Infection frequently contracted from a household
pet.
• May follow infection of another body site.
• Person to person transmission may occur in contact
sports.
• M. canis from cats and dogs most frequent.

24

25
Tinea Corporis

26
Tinea Cruris:-
• tinea cruris is a dermatophyte infection of the
genitalia,pubic area, perineal skin, and perianal skin .
• The scrotum and labia majora are typically not
affected. Infection is more common in men than in
women.
• Often transferred from another infected body site.
• Highly contagious via contaminated towels, floors,
etc.
• Anthropophilic dermatophytes Epidermophyton
floccosum and Trichophyton rubrum are most
common.

27

28
Tinea Capitis• Infection of the scalp involves hyphal
proliferation in the stratum corneum that
extends into the hair follicle orifice and hair
shaft.
• Inflammatory tinea capitis is associated with
zoophilic,Anthropophilic or geophilic species .
• Mild scaling lesions to widespread alopecia.

29
• Kerion: highly inflammatory, suppurating lesion
caused by black dot appearance seen with ectothrix
hair invasion.
• Favus is a distinctive infection with grey, crusting
lesions.
• Asymptomatic carrier state recognized, may promote
spread of infection.
• Affected hair may appear grey due to coating with
arthroconidia.
• infection is associated with Microsporum and
Trichophyton species.

30

31
Ectothrix

32
Onychomycosis
• The term onychomycosis is used to describe infection of the nails with fungi. In addition to the dermatophytes and Candida spp. there are a group of filamentous moulds that can invade nail tissue.
• No specific clinical features; the nail becomes lustreless and thickened. Small pits and streaks may appear in the nail plate, which is at first white, then yellow, brown, green or black
• Multiple nails may be affected, and varying degrees of nail plate area may be covered .
• infections are usually caused by T. soudanense or T. violaceum, other yeast and non dermatophyte molds.

33
34
Tinea Unguium• Tinea unguium, a dermatophyte infection of the nail.
• 19 Risk factors for this infection include aging,
diabetes, poorly fitting shoes, and the presence of
tinea pedis.
• Toenails more often infected than fingernails.
• Infection often follows infection of another body site.
• Most commonly caused by anthropophilic species
Trichophyton mentagrophytes and T. rubrum.
• Affects up to 8% of adult population.

35
Tinea Unguium

36
Tinea Barbae• Tinea barbae involves the skin and coarse
hairs of the beard and mustache area. This
dermatophyte infection occurs in adult men
and hirsute women.
• The usual cause is a zoophilic organism, farm
workers are most often affected.
• Tinea barbae may cause scaling, follicular
pustules, and erythema.

37
Tinea Barbae

38
Tinea Faciei• Tinea faciei tends to occur in the non
bearded area of the face. The patient
may complain of itching and burning,
which become worse after sunlight
exposure.

39
Tinea Faciei

40
NON-DERMATOPHYTE MOLDS
• Several molds demonstrate an ability to invade
keratinous tissue and cause conditions
resembling dermatophytosis.
• The infection caused by these organisms are
clinically indistinguishable from those due to
dermatophytes .

41
Pityriasis Versicolor• Pityriasis versicolor presents as well-defined lesions,
with a fine scale from desquamation, that are either hyper pigmented or hypo pigmented .
• There is a large variation in lesion size from macules to entire trunk coverage .
• Lesions are predominant in areas with a high number of sebaceous glands such as the scalp, chest, and back, as well as upper arms and face
• Facial lesions are more common in children than adults .
• Due to Malassezia yeasts (M. furfur M. globosa, and other species.

42
Pityriasis Versicolor
43
Materials and methods
1-Materials:
• Sterilized scalpels, forceps, Petri dishes.
• Slides ,cover slides & sterile blade.
• Modified Sabouraud dextrose agar with antibiotics
• Instruments :
• incubator at 25-30C, autoclave, light microscope, balance 4 digit, glassware, and other conventional microbiological equipments and chemicals :20% KOH .

44
Materials

45
Clinical Material
• Skin Scrapings, nail scrapings, scalp and
hairs. For a laboratory diagnosis, clinicians
should be aware of the need to generate
an adequate amount of suitable clinical
material. The laboratory needs enough
specimen to perform both microscopy
and culture.

46
Collection procedure• 1-Cleanse the affected area with 70%v/v ethanol.
• 2-Collect skin scales, crusts, pieces of nail, or hairs on
clean slide as follows:
• *Skin scales: Collect by scraping the surface of the
margin of the lesion using sterile scalpel blade.
• *Nail pieces: Collect by taking snipping of the infected
part of the nail using sterile scissors.
• *Hairs: Collect by removing dull broken hairs from
the margin of the lesion using sterile tweezers.

47
Collection procedure

48
Direct microscope• Used to visualizing fungal elements and confirming
the diagnosis of dermatophyte.
• Fungi are usually larger than bacteria, and in material from skin ,hair, or nail ,they can be seen by direct microscopy provided the material is first softened and cleared with strong alkali such as 200g/I(20%w/v)potassium hydroxide(KOH).
• The purpose of the alkali is to digest the keratinsurrounding the fungi so that the hyphae and spores can be seen.
49
Slide preparation with KOH• 1.Place a drop of potassium hydroxide solution on
a slide.
• 2.Transfer the specimen (small pieces)to the drop
of KOH, and cover with cover glass.
• Note: To assist clearing ,hairs should not be more
than 5mm long, and skin scales, crusts and nail
snips should not be more than 2mm across.
• Hairs clear within 5-10minutes.Skin scales and
crusts usually take 20-30minutes. Pieces of nail,
however, may take several hours to clear.

50
Hyphae

51
Hyphae

52
Hyphae

53
Hyphae

54
Malassezia furfur

55
Malassezia furfur

56
Arthrospores

57
Spores

58
Spores: hair

59
Spores :nail

60
Culture
• Useful to confirm the diagnosis of dermatophyte when long-
term oral therapy is being considered, and to identify
dermatophyte species .
• Specimen are cultured as follows:
• Skin scales,crusts,pieces of nail:
• 1.Using a sterile blade or scissors, cut the specimens into
pieces as small as possible.
• 2.Using sterile ,inoculate the small pieces (a few millimeters
apart) ,on the surface of a plate of sabouraud dextrose agar.
• 3.Incubate at incubator (25-30 C). for up to 3 weeks,
examining every few days for growth.

61
Hairs• 1.Using a sterile scissors ,cut the hairs (portion
nearest to the hair root) into small pieces about3-
5 mm long.
• 2.Using sterile tweezers, inoculate the pieces of
hair on the surface of a plate of sabouraud
dextrose agar.
• 3.Incubate at incubator(25-30 C) for up o 3
weeks, examining every few days for growth.

62
Examination of ringworm cultures:
• The colonial appearance (macroscopically) of
the different species of dermatophyte may be
helpful in diagnosis of dermatophytes.
• The identification of the various species is made
by examining microscopically a portion of the
colony for spores and characteristic hyphae as
follows:

63
• 1.Using a sterile needle with 5 mm of its end
bent at a 45 angel, remove carefully a portion of
the colony and transfer it to a drop of saline on
a slide, and cover with a cover glass.
• 2.Examine the preparation using the10X and
40X objectives with the condenser
• Iris diaphragm adjusted to give maximum
contrast.
• 3.Look for the presence of macroconidia,
,microconidia, chlamydospores, and hyphae .

64
Epidermophyton

65
Microsporum canis

66
Trichophyton mentagrophytes

67
Trichophyton rubrum

68
Trichophyton rubrum on
dermatophyte test medium

69
Malassezia furfur on a lipid rich
medium

70
Aspergillus niger

71
Culture tube method

72
Culture tube method

73
Microsporum canis

74
Microsporum canis

75
Epidermophyton floccosum

76
Trichophyton rubrum

77
Epidermophyton floccosum

78
Aspergillus fumigatus

79
Aspergillus

80
Thank You




![Farmaci antifunginei 1] Dermatophytes MicrosporumMicrosporum, Epidermophyton e TrichophytonEpidermophytonTrichophyton 2] Candida 3] Aspergillus 4] Cryptococcus](https://img.dokumen.tips/doc/110x75/5514048e550346d8488b4a99/farmaci-antifunginei-1-dermatophytes-microsporummicrosporum-epidermophyton-e-trichophytonepidermophytontrichophyton-2-candida-3-aspergillus-4-cryptococcus.jpg)