Embed Size (px)
Citation preview

SYMPOSIUM ON ANTIMICROBIAL THERAPY
Current Concepts in Laboratory Testing toGuide Antimicrobial Therapy
Stephen G. Jenkins, PhD, and Audrey N. Schuetz, MD, MPH
Abstract
Antimicrobial susceptibility testing (AST) is indicated for pathogens contributing to an infectious process that warrantsantimicrobial therapy if susceptibility to antimicrobials cannot be predicted reliably based on knowledge of their identity.Such tests are most frequently used when the etiologic agents are members of species capable of demonstrating resistance tocommonly prescribed antibiotics. Some organisms have predictable susceptibility to antimicrobial agents (ie, Streptococcuspyogenes to penicillin), and empirical therapy for these organisms is typically used. Therefore, AST for such pathogens isseldom required or performed. In addition, AST is valuable in evaluating the activity of new and experimental compoundsand investigating the epidemiology of antimicrobial resistant pathogens. Several laboratory methods are available to charac-terize the in vitro susceptibility of bacteria to antimicrobial agents. When the nature of the infection is unclear and the cultureyields mixed growth or usual microbiota (wherein the isolates usually bear little relationship to the actual infectious process),AST is usually unnecessary and results may, in fact, be dangerously misleading. Phenotypic methods for detection of specificantimicrobial resistance mechanisms are increasingly being used to complement AST (ie, inducible clindamycin resistanceamong several gram-positive bacteria) and to provide clinicians with preliminary direction for antibiotic selection pendingresults generated from standardized AST (ie, �-lactamase tests). In addition, molecular methods are being developed andincorporated by microbiology laboratories into resistance detection algorithms for rapid, sensitive assessment of carriagestates of epidemiologically and clinically important pathogens, often directly from clinical specimens (ie, presence of vanco-mycin-resistant enterococci in fecal specimens).
CME Activity
Target Audience: The target audience for Mayo Clinic Proceedings is pri-marily internal medicine physicians and other clinicians who wish to advancetheir current knowledge of clinical medicine; and who wish to stay abreastof advances in medical research.Statement of Need: General internists and primary care providers mustmaintain an extensive knowledge base on a wide variety of topics coveringall body systems as well as common and uncommon disorders. Mayo ClinicProceedings aims to leverage the expertise of its authors to help physiciansunderstand best practices in diagnosis and management of conditions en-countered in the clinical setting.Accreditation: College of Medicine, Mayo Clinic is accredited by the Ac-creditation Council for Continuing Medical Education to provide continuingmedical education for physicians.Credit Statement: College of Medicine, Mayo Clinic designates this Jour-nal-based CME activity for a maximum of 1.0 AMA PRA Category 1Credit(s).™ Physicians should claim only the credit commensurate withthe extent of their participation in the activity.Learning Objectives: Educational objectives. On completion of this article,readers should be able to: (1) interpret the results generated by the variousstandardized methods of antimicrobial susceptibility testing commonly em-ployed by clinical microbiology laboratories; (2) evaluate findings generatedfrom phenotypic methods used for detection of antimicrobial resistance;and (3) explain the rationale for use of molecular methods for detection andcharacterization of antimicrobial resistance determinants.Disclosures: As a provider accredited by ACCME, College of Medicine,Mayo Clinic (Mayo School of Continuous Professional Development) mustensure balance, independence, objectivity and scientific rigor in its educa-tional activities. Course Director(s), Planning Committee Members, Faculty,and all others who are in a position to control the content of this educa-tional activity are required to disclose all relevant financial relationships with
any commercial interest related to the subject matter of the educationalactivity. Safeguards against commercial bias have been put in place. Facultyalso will disclose any off label and/or investigational use of pharmaceuticalsor instruments discussed in their presentation. Disclosure of this informationwill be published in course materials so those participants in the activity mayformulate their own judgments regarding the presentation.In their editorial and administrative roles, William L. Lanier, Jr., MD, Scott C.Litin, MD, Terry L. Jopke, Kimberly D. Sankey, and Nicki M. Smith, MPA,have control of the content of this program but have no relevant financialrelationship(s) with industry.Drs Jenkins and Schuetz have no financial disclosures relevant to thismanuscript. Two drugs mentioned in the article are off-label use for anti-microbial therapy.Method of Participation: In order to claim credit, participants must com-plete the following:1. Read the activity.2. Complete the online CME Test and Evaluation. Participants must achieve
a score of 80% on the CME Test. One retake is allowed.Participants should locate the link to the activity desired at http://bit.ly/zchWvb. Upon successful completion of the online test and evaluation, youcan instantly download and print your certificate of credit.Estimated Time: The estimated time to complete each article is approxi-mately 1 hour.Hardware/Software: PC or MAC with Internet access.Date of Release: 3/1/2012Expiration date: 2/28/2014 (Credit can no longer be offered after it haspassed the expiration date.)Privacy Policy: http://www.mayoclinic.org/global/privacy.htmlQuestions? Contact [email protected].
© 2012 Mayo Foundation for Medical Education and Research � Mayo Clin Proc. 2012;87(3):290-308
asdYork, NY.
290 Mayo Clin Proc.
A ssessment of the antimicrobial suscepti-bility patterns of significant bacterial iso-lates is among the primary responsibili-
ties of the clinical microbiology laboratory. From i
� March 2012;87(3):290-308 � doi:10.1016/j.mayocp.2012.01.007 �
practical perspective, clinicians often perceiveuch test results to be at least as important asetermination of the etiologic agents of patients’
From the Department ofPathology, Weill CornellMedical College, New
nfections. In the face of ever-escalating antimi-
© 2012 Mayo Foundation for Medical Education and Researchwww.mayoclinicproceedings.org

LABORATORY TESTING TO GUIDE ANTIMICROBIAL THERAPY
crobial resistance and the frequent need for treat-ment with newer, often more expensive antibiot-ics, antibacterial susceptibility testing (AST)results take on an increasingly important role.1
DILUTION METHODS FOR ASTAgar and broth dilution methods may be used todetermine the minimum concentrations of antibiot-ics that are required to inhibit or kill microorgan-isms. Drugs under study are typically tested at2-fold doubling (log2) serial dilutions (eg, 4, 8, 16�g/mL, and so on), with the lowest concentration ofeach antibiotic that inhibits visible growth of organ-isms designated as the minimum inhibitory concen-tration (MIC). In the United States, results are usu-ally reported in micrograms per milliliter, whereasin some other parts of the world results may be re-ported in milligrams per liter. The concentrationranges tested vary with the antimicrobial agent, thepathogen under study, and the infection site. Rangesshould encompass the concentrations used to definethe interpretive categories (susceptible, intermedi-ate, and resistant) of the antimicrobial agent and theranges of expected MICs for reference quality con-trol organisms. Alternative dilution methods mayinclude only a single or a selected few concentra-tions of antibiotics, such as breakpoint AST and sin-gle-drug concentration screening. Dilution methodsoffer flexibility in that the standard Mueller-Hintonmedium used for the testing of frequently en-countered pathogens (eg, members of the familyEnterobacteriaceae, staphylococci, enterococci,and some nonfermentative gram-negative bacilli,such as Acinetobacter baumannii and Pseudomonasaeruginosa) may be supplemented or, in somecases, replaced by another medium, allowing foraccurate testing of many fastidious organisms forwhich standardized methods are not availablefor reliable disk diffusion testing. Dilution meth-ods are also amenable for use in automated anti-biotic susceptibility testing systems.
Breakpoints derived by regulatory bodies andprofessional groups are frequently similar. For ex-ample, there are relatively small numbers of discor-dant breakpoints between the US Food and DrugAdministration (FDA) and the Clinical and Labora-tory Standards Institute (CLSI), and those discrep-ancies are under active review by both organiza-tions. By comparison, there are sometimes sizabledifferences in the interpretive criteria used in differ-ent countries or regions of the world for the sameantibiotics. Such disparities are sometimes a func-tion of the fact that different dosages and/or admin-istration intervals are used for the same antimicro-bial agents. In addition, some breakpoint-settingorganizations are more conservative than others in
assessing susceptibility to anti-infectives, placingMayo Clin Proc. � March 2012;87(3):290-308 � doi:10.1016/j.mayocwww.mayoclinicproceedings.org
more emphasis on detection of emerging resistancebased on examination of microorganism popula-tion distributions. Technical factors, including in-cubation temperature and atmosphere, inoculumsize, and test medium formulation, can also affectzone diameters and MICs, justifying differentbreakpoints.
Agar Dilution MethodMueller-Hinton agar is the medium recommendedfor routine testing of most rapidly growing aerobicand facultatively anaerobic bacterial pathogens. Thesolvents and diluents that are required to preparestock solutions of antibiotics and the methodsused to perform such testing are defined in theCLSI standard on dilution AST.2 The agar dilutionapproach to susceptibility testing is both wellstandardized and reproducible and may be usedas a reference method in the evaluation of otherdilution assays. This method facilitates the con-comitant and efficient testing of large numbers oforganisms. In addition, population heterogeneity(ie, resistant subpopulations of organisms) and in-oculum contamination (ie, “mixed” cultures) aremore easily detected by agar than by broth testing.The primary disadvantages of this testing approachare the labor-intensive, time-consuming steps re-quired to prepare testing plates, particularly whenthe number of compounds to be tested is high orwhen only a limited number of bacteria are to bestudied, or both. For these reasons, most clinicalmicrobiology laboratories do not use this approachfor routine AST.
Broth Dilution MethodsGeneral approaches to broth dilution testing includeboth macrodilution, wherein volumes of broth intest tubes for each dilution typically equal or exceed1 mL, and broth microdilution (BMD), in whichantimicrobial concentrations are most frequently ofsmaller volumes in 96-well microtiter plates. Thebroth macrodilution approach is both reliable andwell standardized and is of particular utility in re-search studies and in testing of a single antimicrobialagent for 1 bacterial isolate. The method is, how-ever, both laborious and time intensive and, becauseof the ready commercial availability of convenientmicrodilution systems, is not generally consideredpractical for routine use in clinical microbiologylaboratories.
The convenience afforded by BMD has led to itswidespread use in both clinical and reference labo-ratories. This approach is, in fact, now consideredthe reference international testing method.3 Plastic,disposable plates containing a panel of several anti-
biotics to be tested concomitantly may be preparedp.2012.01.007 291

pbifirpdtcbbrctr
pwpm
srbdshiird(restaahlutmpttpc
MAYO CLINIC PROCEEDINGS
292
within the laboratory or, alternatively, purchasedfrom commercial vendors either as freeze-dried orfrozen trays. The BMD technique is also well stan-dardized and reliable. The inoculation and readingprocedures readily lend themselves to the simulta-neous testing of several antibiotics with single bac-terial isolates. Although most commercially avail-able systems use multipoint inoculating devices orautomated inoculation instruments, plates may alsobe inoculated with multichannel pipettors. Testingresults may be determined either visually or throughthe use of semiautomated or automated instru-ments. An example of a commercially availablemanual BMD is Sensititre (TREK Diagnostic Sys-tems, Cleveland, OH). Examples of automated BMDplatforms include the BD Phoenix (Becton Dickin-son, Franklin Lakes, NJ), Microscan (SiemensHealthcare Diagnostics, Deerfield, IL), and Vitek(bioMérieux, Marcy l’Etoile, France).
AGAR DISK DIFFUSION TESTINGIn many clinical microbiology laboratories an agardisk diffusion method is routinely used for the test-ing of common, rapidly growing, and some fastidi-ous bacterial pathogens, allowing categorization ofmost such isolates as susceptible, intermediate, orresistant to a wide range of antimicrobial agents.This approach is particularly common in resource-limited settings and when performed according tostandardized methods, such as those published bythe CLSI, provides accurate direction to cliniciansmaking therapeutic antibiotic decisions.4 With thistesting approach, commercially prepared filter pa-per disks impregnated with specified predeterminedconcentrations of the antibiotics to be assessed areapplied to the surface of a defined agar mediumpreviously inoculated with the challenge bacterialpathogen. The antimicrobial agents then diffusefrom the disks through the agar, and as the distancefrom the disks increases, the drug concentrationsdecrease in a logarithmic fashion, creating gradientsof drug concentrations in the medium around thedisks. Simultaneously with the diffusion of thedrugs, the bacteria inoculated to the agar surface notinhibited by the concentrations of the antibiotics inthe agar multiply, creating a visible lawn of growth.In areas where the test organism is inhibited by theantimicrobial agents, growth fails to occur, resultingin zones of inhibition around each active drug. Theinhibitory zone diameters are influenced by the dif-fusion rates of the various antimicrobial agentsthrough the agar, a function of the molecular sizesand hydrophilicities of the compounds. The zonesizes are inversely proportional to the logarithms ofthe antibiotic MICs. After incubation at recom-mended temperatures, atmospheric conditions, and
times, depending on the pathogen under study, the iMayo Clin Proc. �
diameters of the zones of inhibition are measured inmillimeters and interpreted based on publishedstandards. The most recent criteria for interpretingzone diameters of inhibition for antibiotics ap-proved for use by the FDA are listed in Table 3 of adocument updated annually by the CLSI.5
Such disk diffusion interpretive criteria (break-oints) are chosen after the establishment of MICreakpoints, which is accomplished by plotting the
nhibition zone diameters against the MICs derivedrom the testing of a large number of strains of var-ous species. A statistical approach using a linearegression formula may be used to calculate the ap-ropriate zone diameter intercepts for previouslyetermined MIC breakpoints. An alternative, prac-ical approach to deriving disk diffusion interpretiveriteria is the use of the error rate–bounded methody which the zone diameter breakpoints are selectedased on the minimization of disk interpretive er-ors, particularly very major errors.6,7 This most re-ent CLSI approach focuses on the rate of interpre-ive errors near the proposed breakpoint vs errorates for MICs greater than a single log2 dilution
from the MIC breakpoints.8 The concept of this ap-roach is that errors occurring with organisms forhich MICs closely approximate the MIC break-oints are less of a clinical concern than errors forore highly susceptible or resistant isolates.
The disk diffusion approach for AST has beentandardized primarily for commonly encountered,apidly growing bacterial pathogens and is applica-le to neither anaerobes nor fastidious species thatemonstrate marked variability in growth rate fromtrain to strain.9 The disk diffusion test approachas been modified, though, to allow for reliable test-
ng of several species of fastidious bacteria, includ-ng Haemophilus influenzae and Neisseria gonor-hoeae. There are several advantages to the diskiffusion approach to AST, including the following:1) it is technically easy to perform and results areeproducible, (2) the reagents and supplies are in-xpensive, (3) it does not require the use of expen-ive equipment, (4) it generates categorical interpre-ive results well understood by clinicians, and (5) itllows for considerable flexibility in the selection ofntibiotics for testing. However, this method alsoas a number of drawbacks. For example, only a
imited number of bacterial species can be testedsing this approach. In addition, the disk diffusionest is inadequate for detection of vancomycin-inter-ediate Staphylococcus aureus. Of importance, itrovides only a qualitative result, whereas a quanti-ative MIC result that indicates the degree of suscep-ibility may in some cases be required (eg, whenrolonged or continuous infusion of specific antimi-robial agents is being considered for treatment of
nfections caused by relatively resistant bacteria).March 2012;87(3):290-308 � doi:10.1016/j.mayocp.2012.01.007www.mayoclinicproceedings.org

NmmmAtisdpofTtltlsbtd
LABORATORY TESTING TO GUIDE ANTIMICROBIAL THERAPY
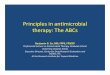
GRADIENT DIFFUSION METHODSThe M.I.C.Evaluator (Oxoid, Cambridge, UK) andEtest (bioMérieux, Durham, NC), are commerciallyavailable gradient diffusion systems for quantitativeAST. Both systems use preformed antimicrobial gra-dients applied to 1 face of a plastic strip to generatediffusion of drug into an agar-based medium. Theassays are performed in a manner similar to that fordisk diffusion using a suspension of test organismequivalent in turbidity to that of a 0.5 McFarlandstandard to inoculate the surface of an agar plate.Following recommendations for incubation temper-atures, times, and atmospheric conditions, the MICis read directly from a preprinted scale on the top ofthe strip at the point at which the ellipse of organismgrowth inhibition intercepts the strip. An exampleof an isolate tested for antimicrobial susceptibilityby both Etest and disk diffusion is shown in theFigure. Several strips containing different antimi-crobial agents may be applied in a radial arrange-ment to the surface of large round plates, or theymay be placed in opposite directions on large rect-angular plates. Minimum inhibitory concentrationsgenerated by these methods generally agree wellwith those obtained using standard agar and brothdilution methods.10-12 Such gradient methods aresimilar in flexibility and simplicity to the disk diffu-sion approach, but they enable one to determinequantitative MICs. Significant advantages of the agargradient diffusion systems include the ability to gen-erate quantitative MIC results for infrequently testedantimicrobial agents and the option to test fastidiousand anaerobic organisms, for which reliable diskdiffusion methods and/or commercial systems are
FIGURE. Manual susceptibility testing of Pseu-domonas aeruginosa by Etest and disk diffusion.Various patterns of susceptibility and resis-tance are seen.
not available, through the use of specific enriched M
Mayo Clin Proc. � March 2012;87(3):290-308 � doi:10.1016/j.mayocwww.mayoclinicproceedings.org
media. Gradient diffusion strips are, however, con-siderably more expensive than the paper disks usedfor diffusion testing.
METHODS FOR FASTIDIOUS BACTERIAMany fastidious bacterial species do not grow satis-factorily using standard in vitro susceptibility test-ing approaches with unsupplemented media. Forseveral of the more frequently encountered patho-gens (eg, Streptococcus pneumoniae and Streptococcusspp other than S pneumoniae, N gonorrhoeae, and
eisseria meningitidis, and H influenzae and Hae-ophilus parainfluenzae), modifications have beenade to the standard CLSI MIC and disk diffusionethods to allow laboratories to perform reliableST. Such modifications typically involve the use of
est media with supplemental nutrients, prolongedncubation times, and/or incubation in an atmo-phere with an increased concentration of carbonioxide. Specific MIC and zone diameter break-oints have been established by the CLSI for suchrganisms, as have recommended acceptable rangesor the testing of applicable quality control strains.he CLSI has also published guidelines for AST of
he fastidious and/or infrequently recovered bacteriaisted in the Table.13 Methods for the standardizedesting of potential agents of bioterrorism (eg, Bacil-us anthracis, Francisella tularensis, Brucella spp, Yer-inia pestis, and Burkholderia pseudomallei) have alsoeen developed, and specific conditions for theiresting are defined in Table 2 of the CLSI M45-A2ocument.13 Currently, specific recommendations
for several other fastidious bacteria, including Legion-ella and Bordetella spp, do not exist, partially becauseinfections caused by these species typically respondwell to the recommended drugs of choice, they arerelatively uncommon isolates in clinical laborato-ries, and they require special complex media for re-covery in vitro, presenting unique problems in thedevelopment of AST assays.
For the most part, breakpoints for these bacteriawere predicated on interpretive criteria establishedfor other organisms as published in CLSI standardsand adapted based on published literature and theexperience of the authors of the document. This is insharp contrast to the extensive body of clinical mi-crobiologic, pharmacokinetic, and pharmacody-namic information typically used for the establish-ment of breakpoints as published in other CLSIstandards. Because of the limited testing and natureof the potential agents of bioterrorism and Helico-bacter pylori, the interpretive recommendations andtesting approaches for these organisms were re-cently transferred from the standard CLSI M100documents to the M45 guideline.13
As mentioned, in addition to standard disk and
IC methods, many species of fastidious bacteriap.2012.01.007 293

ai
lapFbtlno
bfAft
MAYO CLINIC PROCEEDINGS
294
may be tested by a gradient agar technique. TheEtest method permits placement of strips on mediaoptimal for the growth of the organism being testedand allows the use of various incubation conditions.A major limitation, however, to such an approach islack of approval for such testing by the FDA.When FDA clearance has not been awarded, theresults of such testing should be interpreted withcaution, and an applicable qualifying commentshould be an integral component of any resultantpatient report.
SUSCEPTIBILITY TESTING OF ANAEROBICBACTERIAThe importance of anaerobic bacteria as participantsin and causes of significant infections and the needfor specific antibiotic therapy for bacteremia andsurgical prophylaxis against anaerobes are welldocumented.14-19 As a rule, AST is considered anecessity for effective guidance of antibiotic ther-apy, but how and when susceptibility testing ofanaerobic bacteria should be performed havebeen topics of debate, in part owing to a numberof misconceptions and confounding factors.20-24
Specimens collected from infections in which anaer-obes are involved are typically polymicrobic, ren-dering isolation and identification of individual or-ganisms slow and the results of AST too delayed tohave a consistent positive effect on individual pa-tient outcomes. For clinicians, the combination ofsurgical intervention and broad-spectrum antibiot-ics has limited the correlation of potential antibac-terial resistance with outcome, directing many clin-
TABLE. Clinical and Standards Laboratory Institute PTesting of Fastidious and/or Infrequently Recovered B
Abiotrophia and Granulicatella spp (once referred to as tstreptococci)
Aeromonas spp
Bacillus spp other than Bacillus anthracis
Campylobacter coli and Campylobacter jejuni
Corynebacterium spp
Erysipelothrix rhusiopathiae
The group of bacteria previously referred to as the HAAggregatibacter aphrophilus, Cardiobacterium hominis,
Facultatively anaerobic Lactobacillus spp
Leuconostoc spp
Listeria monocytogenes
Moraxella catarrhalis
Pasteurella spp
Pediococcus spp
Plesiomonas shigelloides
ical microbiology laboratories away from the routine
Mayo Clin Proc. �
performance of anaerobic susceptibility testing.There is considerable evidence, though, that antibi-otic resistance is common among many anaerobicspecies and that patient treatment with inactiveagents results in poor clinical responses and in-creased rates of mortality.14,16,19,25,26 Results ofAST have also indicated that substantial differencesexist in resistance patterns among hospitals on a lo-cal, regional, and national basis, suggesting that onemedical center’s patterns may not be applicable tothose of other facilities.27-30 Therefore, the need fornaerobic AST is of far more importance today thann the past.
If practical, individual hospitals should estab-ish antibiograms for the more frequently recoverednaerobes on a periodic basis and test individualatient isolates as needed to assist in patient care.or purposes of presenting cumulative antimicro-ial susceptibility data, an attempt should be madeo include the results from 80 to 100 anaerobic iso-ates with recognized important resistance mecha-isms (eg, clindamycin resistance among membersf the Bacteroides fragilis group). Ideally, following
CLSI guidelines for preparation of antibiograms, 30isolates for each genus or species should be in-cluded.31 When this is not possible, an effort shoulde made to present data for 30 isolates from the B
ragilis group and at least 10 strains for other genera.ntibiotics in the report should reflect the hospital
ormulary. A recent CLSI document included an an-ibiogram for members of the B fragilis group gener-
ated from the results of testing of isolates collectedat many health care facilities across the United
hed Guidelines for Antimicrobial Susceptibilityria
ependent, pyridoxal-dependent, or nutritionally variant
organisms (Aggregatibacter actinomycetemcomitans,ella corrodens, and Kingella kingae)
ublisacte
hiol-d
CEKEiken
States by 3 reference laboratories.32 Clinicians
March 2012;87(3):290-308 � doi:10.1016/j.mayocp.2012.01.007www.mayoclinicproceedings.org

afllibtd
dmwptbb
LABORATORY TESTING TO GUIDE ANTIMICROBIAL THERAPY
may refer to this document when prescribing em-pirical therapy for suspected or proven B fragilisgroup infections in settings in which anaerobicAST is not available.
To assist in management, anaerobic susceptibil-ity testing should be performed when (1) the selec-tion of an antibiotic to which the isolate is suscepti-ble is critical for treatment of the patient, (2) long-term therapy is under consideration, (3) anaerobesare recovered from specific, usually sterile, bodysites (eg, bone, blood, joint, or brain), or (4) treat-ment with an antimicrobial agent typically activeagainst the organism has failed.
The agar dilution susceptibility testing ap-proach, which uses Brucella blood agar as the me-dium, has been designated the reference method bythe CLSI anaerobe working group.33 Because of thetime-consuming, labor-intensive nature of thismethod, it is not generally considered practical forroutine use in most clinical microbiology laborato-ries but serves as the reference method to whichother more practical testing approaches can be com-pared. Alternative testing methods currently usedinclude BMD (only standardized for members of theB fragilis group), limited agar dilution, and gradientstrip diffusion assays, such as Etest. Disk diffusionand broth disk elution testing should not be usedbecause the results generated from such methodsdo not correlate with the CLSI reference agar di-lution method.33 Although of limited use, �-lac-tamase testing may be of value for some organismsif therapy with ampicillin or penicillin is beingconsidered.
METHODS FOR SUSCEPTIBILITY TESTINGOF NOCARDIA SPP AND OTHER AEROBICACTINOMYCETESSusceptibility testing of Nocardia spp and other aer-obic actinomycetes (Rhodococcus spp, Streptomycesspp, Gordonia spp, and Tsukamurella spp) should beperformed on clinically significant isolates. Suscep-tibility testing results serve to guide initial therapeu-tic choices and may document emergence of drugresistance. No commercially available broth sys-tems have yet been cleared by the FDA for Nocar-dia spp or other aerobic actinomycetes. The CLSIBMD is the reference method for testing.34 Rec-ommended drugs for primary testing are amika-cin, amoxicillin-clavulanate, ceftriaxone, cipro-floxacin, clarithromycin, imipenem, linezolid,minocycline, moxifloxacin, trimethoprim-sulfa-methoxazole, and tobramycin. Second-line drugsfor testing include cefepime, cefotaxime, and doxy-cycline. Vancomycin and rifampin results shouldalso be reported on isolates of Rhodococcus equi be-cause these drugs are particularly useful therapeuti-
cally. Microbiological breakpoints were establishedMayo Clin Proc. � March 2012;87(3):290-308 � doi:10.1016/j.mayocwww.mayoclinicproceedings.org
in 2003 and are available for Nocardia spp only.34
When aerobic actinomycetes other than Nocardiaspp are tested, the susceptibility categories shouldbe listed as tentative. The breakpoints for S aureusshould be adapted as provided in the current CLSIM100 document (M100-S21) for R equi, but theyshould also be reported as tentative. Susceptibilitytesting results for most aerobic actinomycetes areavailable within 3 to 5 days, whereas results for Requi and some isolates of Tsukamurella spp may beread at 24 or 48 hours.
Challenges in the identification and AST of No-cardia spp have become apparent within the past 10years. Before the year 2000, conventional pheno-typic methods were largely used to identify Nocardiaspp; however, molecular identification is now thepreferred means of reliable identification to the spe-cies level.35 Both 16s ribosomal RNA sequencingnd matrix-assisted laser desorption/ionization-time ofight are among the techniques currently used, but
imitations exist.36 Because routine molecular test-ng is difficult to implement in many clinical micro-iology laboratories, isolates typically must be sento a reference laboratory for identification. To ad-ress this issue, Wallace et al37 proposed a series of
various susceptibility patterns that could predictplacement of Nocardia spp within particular groups,but, as new strains are identified, these groupingshave not proved to be valid, particularly for the No-cardia nova complex.
The method for susceptibility testing of Nocar-ia spp also presents a challenge to many clinicalicrobiology laboratories because BMD is some-hat impractical owing to cost, availability of sup-lies, and expertise needed to perform and interprethe results. Moreover, false resistance with BMD haseen noted for ceftriaxone when testing Nocardiarasiliensis and imipenem when testing Nocardia far-
cinica.34 In addition, sulfonamide results are incon-sistent when using BMD; for this compound, diskdiffusion testing with sulfisoxazole may be per-formed concurrently. Investigators have evaluateduse of the Etest method compared with BMD, withvarying results.38 However, both lack of agreementwith BMD and the absence of standardized methodshave restricted routine use of the Etest. The CLSI hasproposed that the agar proportion method be usedto confirm questionable results from commercialbroth systems and to test additional antibiotics orconcentrations of drugs.
The major taxonomic revisions within the last10 years have further complicated testing becauseclinical and epidemiological differences existamong species. Furthermore, resistance to trim-ethoprim-sulfamethoxazole and other antimicro-
bials is increasing among various species; thus,p.2012.01.007 295

bcimmtsstupidtbtt
bcramiwbcascimw
tmtaiie
MAYO CLINIC PROCEEDINGS
296
identification of isolates to the species level re-mains imperative.39
METHODS FOR SUSCEPTIBILITY TESTINGOF MYCOBACTERIAAccording to the most recent Centers for DiseaseControl and Prevention mycobacterial suscepti-bility testing guidelines, initial isolates from pa-tients with tuberculosis should be tested for sus-ceptibility to isoniazid, rifampin, ethambutol, andpyrazinamide.40 This guidance overrides the priorpractice of performing susceptibility testing for only3 drugs (isoniazid, rifampin, and ethambutol) andthen only when a pulmonary or infectious diseaseclinician requested it. Current guidelines also statethat susceptibility testing should be repeated after 3months if the patient remains culture-positive de-spite appropriate therapy. However, susceptibilitytesting may be performed earlier if the patient ap-pears to be failing to respond to therapy or if in-tolerance to the drug regimen is evident. First-linesusceptibility test results should be available forisolates of the Mycobacterium tuberculosis complexwithin 15 to 30 days of original receipt of thespecimen in the laboratory.41 However, ideally,susceptibility results should be available within 7to 14 days of specimen receipt.34 If resistance toany of the 4 initially tested agents is discovered,testing of secondary drugs should be performedas soon as possible. If the isolate is resistant onlyto pyrazinamide, Mycobacterium bovis should beruled out because most M tuberculosis isolates aresusceptible to pyrazinamide. Further specificguidelines regarding secondary drug testing andfollow-up are outlined in CLSI M24-A2.34
The agar proportion approach has traditionallybeen considered the standard method for antimyco-bacterial susceptibility testing, but as an agar-basedsystem, the time to result reporting is lengthy (ap-proximately 3 weeks).42 Both the agar proportionmethod and the radiometric method define resis-tance as growth of more than 1% of the inoculum ofbacterial cells in the presence of an antituberculardrug. The antitubercular drugs are inoculated atspecific in vitro concentrations, the values ofwhich correlate to clinical responsiveness. If morethan 1% of the bacterial population grows in thepresence of a drug, that particular drug will not beof therapeutic utility.42 The agar proportionmethod is used primarily to confirm results fromcommercial liquid broth systems and to test addi-tional drugs that may not be available for testingusing other systems. The FDA-cleared broth sys-tems for M tuberculosis testing have shorter incu-bation times than the agar proportion method;however, these commercial testing systems are
only cleared for certain drugs.43 aMayo Clin Proc. �
There are several molecular assays that haveeen developed for the detection of mutations asso-iated with drug resistance in M tuberculosis, includ-ng both real-time polymerase chain reaction (PCR)
ethods and line probe assays.44 Molecular-basedethods for detection of M tuberculosis drug resis-
ance are more rapid than traditional methods ofusceptibility testing. Mutations associated with re-istance to isoniazid or rifampin are typically de-ected by such methods. These tests may be runsing growth from positive cultures but may also beerformed directly on acid-fast smear-positive spec-
mens if the patient is highly suspected of havingrug-resistant tuberculosis. It is currently suggestedhat molecular testing of drug susceptibility beacked up by culture, with performance of pheno-ypic culture-based drug susceptibility testing whenhe isolate is retrieved from culture.34
Susceptibility testing of nontuberculous myco-acteria (NTM) should be performed on isolatesonsidered clinically significant. The American Tho-acic Society criteria for clinical significance of NTMre positive cultures from at least 2 sputum speci-ens or 1 bronchial wash or bronchial lavage spec-
men. Alternatively, a transbronchial or lung biopsyith histopathologic findings consistent with myco-acteria and positive on culture for NTM is suffi-ient to be interpreted as clinically significant. Inddition, NTM isolates from usually sterile bodyites, such as cerebrospinal fluid, are consideredlinically significant. However, routine susceptibil-ty testing need not be performed on Mycobacteriumarinum because acquired resistance is uncommonith this organism.34 Initial susceptibility testing of
Mycobacterium kansasii to isoniazid, rifampin, andethambutol need not be performed but can be of-fered if treatment has failed.
The standard susceptibility testing method forNTM is BMD. The American Thoracic Society andCLSI guidelines exist for susceptibility testing ofmembers of the Mycobacterium avium complex, Mkansasii, M marinum, and the rapidly growing my-cobacteria.34 However, accurate susceptibility predic-tions for other slowly growing mycobacteria cannot bemade. The macrolides are the only antimicrobial agentsthat should be tested against M avium complex be-cause they are the only agents for which correlationshave been demonstrated between in vitro suscepti-bility tests and clinical response.45 Because the mu-ation leading to resistance is the same for clarithro-ycin and azithromycin, only 1 drug need be
ested. Generally, clarithromycin is tested becausezithromycin demonstrates poor solubility. If thesolate is macrolide resistant, testing for susceptibil-ty to the secondary agents moxifloxacin and lin-zolid may be considered. Susceptibility testing of M
vium complex may also be performed if the patientMarch 2012;87(3):290-308 � doi:10.1016/j.mayocp.2012.01.007www.mayoclinicproceedings.org

bmi
rboat
stfca
m
DI
a
wtt
LABORATORY TESTING TO GUIDE ANTIMICROBIAL THERAPY
relapsed while undergoing macrolide therapy. Inaddition, susceptibility testing should be repeatedafter 3 months of therapy for patients with dissem-inated M avium complex disease and after 6months of therapy for patients with chronic pul-monary disease caused by M avium complex.Commercially available broth systems have notyet been cleared by the FDA for slowly growingNTM.
PHENOTYPIC AND GENOTYPIC METHODS FORDETECTION OF ANTIMICROBIAL RESISTANCEA number of phenotypic tests are available to theclinical microbiology laboratory to characterize apathogen’s susceptibility to an antibiotic by screen-ing for a specific resistance mechanism or pheno-type. Although such screening tests do not result indetermination of an MIC, some have sufficient spec-ificity and sensitivity that confirmatory testing is notrequired and the screening test result can be re-ported without further testing. Other assays requireadditional or confirmatory testing. For example, testsfor inducible clindamycin resistance among staphylo-cocci and screening tests for high-level gentamicinand streptomycin resistance in enterococci are gen-erally considered to be comparable to standardmethods for the detection of clinically significantresistance, and they do not require confirmatorytesting. By comparison, laboratories that use ertap-enem resistance as a surrogate marker for carbapen-emase production among certain species of Entero-bacteriaceae must confirm resistance to meropenem,imipenem, or doripenem by another more standard-ized approach because ertapenem-resistant strains arenot always resistant to these other agents.
In addition, methods for the direct detection ofantibiotic-resistant bacteria in clinical samples haveprogressed rapidly in recent years, largely because ofthe continued evolution and spread of multidrug-resistant pathogens, such as methicillin-resistant Saureus (MRSA). The development of commercial as-says that facilitate rapid detection of such pathogensdirectly from clinical specimens, often generatingresults in a few hours or less, has positively en-hanced surveillance efforts and patient manage-ment. Other genotypic assays for detection of spe-cific antimicrobial resistance genes in gram-negativebacteria (eg, blaKPC-containing Klebsiella pneu-moniae) have the potential to improve therapeuticpatient decisions and assist in epidemiological in-vestigations of resistance gene dissemination in thehospital and community setting.
�-LACTAMASE TESTSA positive �-lactamase test result indicates that the
organism is resistant to applicable �-lactam agents,Mayo Clin Proc. � March 2012;87(3):290-308 � doi:10.1016/j.mayocwww.mayoclinicproceedings.org
ut a negative reaction is inconclusive because otherechanisms of resistance to the �-lactams may ex-
st. For example, a positive �-lactamase test resultfor a strain of N gonorrhoeae means that the isolate isresistant to penicillin, ampicillin, and amoxicillinand that these drugs would not be appropriate ther-apeutic choices. However, a �-lactamase test onlydetects one form of penicillin resistance in N gonor-rhoeae. Strains with chromosomally mediated resis-tance with penicillin-binding protein modificationscan only be detected by the disk diffusion or the agardilution MIC method.46,47
Three direct �-lactamase tests—the acidomet-ic, iodometric, and chromogenic methods—haveeen widely used. All 3 methods involve the testingf isolates grown on nonselective media, and resultsre typically available within 1 to 60 minutes. Al-hough some bacteria (eg, N gonorrhoeae and H in-
fluenzae) produce �-lactamase constitutively, oth-ers (eg, staphylococci) may produce detectablelevels of enzyme only after exposure to an induc-ing agent, typically a �-lactam.48 Even after induc-tion, though, direct �-lactamase tests may not beufficiently sensitive to detect �-lactamase produc-ion in all staphylococci.49 Therefore, for serious in-ections that require penicillin therapy, clinical mi-robiology laboratories should perform both MICnd induced �-lactamase tests on all subsequent iso-
lates from the same patient. In addition, PCR testingof the isolate for the presence of the blaZ �-lacta-
ase gene may also be an option.
ETECTION OF METHICILLIN RESISTANCEN STAPHYLOCOCCUS SPPThe most common currently used method for thedetection of MRSA is culture.50 Traditional MRSAdetection methods consist of culture from a selectiveliquid or solid medium. Recently, chromogenicagars have shown improved sensitivity and specific-ity over nonchromogenic media for detection ofMRSA.51 Chromogenic agars contain selective anti-biotic(s) and various chromogenic substrates, whichprovide easy visual identification of colonies. An ad-ditional advantage of chromogenic agar is the fastertime to detection of the organism. MRSA is oftendetected within 20 to 48 hours on chromogenic me-dia, with a high percentage of cases identified within24 hours.52 Several chromogenic media are avail-ble from different manufacturers.
The use of an overnight preenrichment stepith selective broth medium before inoculation of
he agar has been shown to increase sensitivity of theesting by 15% to 30%.53 However, the delay in
detection of an additional 18 to 24 hours and thecost of the selective broth medium represent
disadvantages.p.2012.01.007 297

mgtautpi
cb
wcatemciahHa
iAtsa
DETpcimUtn
tmtgtiagt
MAYO CLINIC PROCEEDINGS
298
Early diagnosis of MRSA in the laboratory is cru-cial in guiding appropriate antimicrobial therapy.Rapid molecular methods of MRSA detection areincreasingly used and are available for testing from avariety of sources.54 Traditional detection of MRSAfrom automated blood culture instruments is time-consuming because 24 to 72 hours are required forsubculture, biochemical identification, and AST ofthe isolate once the result turns positive. Severaltechniques are available for identification of MRSAdirectly from blood culture bottles that have flaggedas positive for growth when gram-positive cocci inclusters are seen on Gram stain.55 Several commer-cial molecular methods are available, including nu-cleic acid amplification and hybridization assays.51
A commercial penicillin-binding protein 2a latex ag-glutination kit, which facilitates the detection ofthe protein product expressed by the mecA gene,is available for detection of MRSA directly fromblood culture.56 Other systems are currently un-der investigation.50
HIGH-LEVEL AMINOGLYCOSIDE RESISTANCEIN ENTEROCOCCISuccessful treatment of enterococcal endocarditisand other serious enterococcal infections requiresthe use of an aminoglycoside with a cell wall–activeagent, such as ampicillin, penicillin, or vancomycin.All enterococci demonstrate innate low-level resis-tance to aminoglycosides because of their facultativeanaerobic metabolism, which reduces transmem-brane potential, thereby limiting drug uptake. How-ever, the bactericidal combination of an aminogly-coside and a cell wall–active antimicrobial, whichallows for markedly enhanced uptake of the amino-glycoside, leads to enhanced killing of the organismin the absence of high-level aminoglycoside resis-tance (HLAR).
The CLSI recommends HLAR screening of en-terococci with both gentamicin and streptomycinfrom blood cultures or other specimens submittedfor the evaluation of endocarditis, such as heartvalve tissue. The BMD may be performed by assess-ing growth of the organism in the presence of 1000�g/mL of streptomycin or 500 �g/mL of gentamicinin brain heart infusion broth.5 The recommendedscreening concentrations for streptomycin andgentamicin using other methods are also cov-ered.57 Performance data of commercially avail-able media and systems for HLAR screening havebeen reviewed.58
In enterococci, HLAR is mediated by aminogly-coside-modifying enzymes (AMEs), which modifythe aminoglycoside by acetylation, adenylation, orphosphorylation. The most prevalent AME geneamong enterococci with HLAR to gentamicin is
aac(6’)-Ie-aph(2”)-Ia, which has both acetyltrans- vMayo Clin Proc. �
ferase and phosphotransferase activity.59 This com-on AME confers resistance to all available amino-
lycosides, except streptomycin. Commonly, HLARo streptomycin is mediated by either ant(6’)-Ia ornt(3’’)-Ia; in such cases, streptomycin should not besed in combination with a �-lactam agent. Detec-ion of HLAR to both gentamicin and streptomycinrecludes the use of aminoglycosides for synergism
n any clinical situation.Enterococcus faecium possesses a naturally oc-
urring AME, resulting in moderate resistance to to-ramycin (MICs, 64-1000 �g/mL). The presence of
the aac(6’)-Ii gene precludes synergistic treatmentith tobramycin, kanamycin, netilmicin, or sisomi-
in. In addition, many enterococci possess theph(3’)-IIIa gene, which confers high-level resis-ance to kanamycin and abolishes any synergisticffect with amikacin. Thus, gentamicin and strepto-ycin are the only 2 aminoglycosides to test and
onsider for synergistic therapy. Novel genes carry-ng AMEs mediating resistance to gentamicin, suchs aph(2’’)-Ib, aph(2’’)-Ic, aph(2’’)-Id, and aph(2’’)-Ie,ave been discovered and may further complicateLAR testing because the susceptibilities to various
minoglycosides differ.60 Because of the large num-bers of AME-encoding genes, molecular HLARscreening in enterococci remains investigational andhas not yet been widely available in clinical micro-biology laboratories.61
Issues that continue to challenge HLAR screen-ng in enterococci include the isolation of multipleMEs within single enterococcal isolates, isolates
hat harbor infrequent AMEs but do not demon-trate the HLAR phenotype, and the increasing prev-lence of various HLAR enzymes in enterococci.
ETECTION OF VANCOMYCIN-RESISTANTNTEROCOCCIhe vancomycin-resistant enterococci (VRE) are im-ortant opportunistic pathogens in many healthare facilities and common colonizers of the gastro-ntestinal tract. The VRE are among the most com-
on causes of hospital-acquired infections in thenited States, and patients colonized with VRE in
he gastrointestinal tract may serve as reservoirs forosocomial transmission.62,63
Two common patterns of enterococcal resis-ance exist, both of which result in elevated vanco-ycin MICs. The first, and most clinically impor-
ant, is vancomycin resistance due to acquisition ofenetic information, usually on a plasmid or otherransmissible genetic element.64 This acquired traits most commonly observed in strains of E faeciumnd Enterococcus faecalis harboring the vanA or vanBenes that encode for high-level vancomycin resis-ance. Expression of the vanA gene results in ele-
ated vancomycin MICs (�128 �g/mL) and is theMarch 2012;87(3):290-308 � doi:10.1016/j.mayocp.2012.01.007www.mayoclinicproceedings.org

qiidVstmasit
tt
haVtrpomtlpt
iasam
CACttaacssmttte
dm
LABORATORY TESTING TO GUIDE ANTIMICROBIAL THERAPY
dominant resistance factor in enterococci. By com-parison, expression of the vanB gene results in lowervancomycin MICs, typically in the range of 16 to 64�g/mL. The second pattern of resistance, intrinsic(inherent) in nature, is characteristically seen in En-terococcus gallinarum and Enterococcus casseliflavus.Most frequently encoded by vanC, this pattern ofresistance may also be due to the expression of genesother than vanC (eg, vanE, vanG, and vanL) and re-sults in either low-level resistant or intermediateMICs, typically in the 2- to 16-�g/mL range.65 Con-tact precautions are generally only required for pa-tients harboring enterococci with acquired resis-tance, such as E faecium or E faecalis. Guidelines forsusceptibility testing of enterococcal pathogenswhen grown in culture from blood or other siteshave remained fairly standard over time. How-ever, there have been several recent advances inboth culture-based and molecular-based screen-ing of stool for VRE, facilitating identification ofpatients who are potential reservoirs for infectionand transmission.
The CLSI guidelines for vancomycin suscepti-bility testing of enterococci isolated from varioussites suggest the use of standard BMD or disk diffu-sion testing.5 If disk diffusion or Etest is performed,the susceptibility plates must be held for a total of 24hours to obtain accurate readings. Organisms forwhich vancomycin MICs are in the range of 8 to 16�g/mL should be further identified by biochemicaltesting because infection control precautions willdiffer based on identification of the organism as anEnterococcus sp other than E faecalis or E faecium.Accordingly, isolates with intermediate zones ondisk testing should be tested by an MIC methodand/or further identified by biochemical and otheridentification tests to guide appropriate infectioncontrol practices.
A variety of culture-based and molecularmethods have been studied to support active sur-veillance efforts to identify VRE from the gastroin-testinal tract.66,67 Although culture-based methods arenot as rapid as molecular-based screening methods,isolates obtained from culture can be stored for fur-ther study or identification. Molecular-based VREscreening methods decrease the time to identifica-tion but are costly. Culture remains the screeningmethod of choice for VRE stool screening, but mo-lecular methods are becoming increasingly recog-nized and used. Some investigators advocate theuse of a broth enrichment step before inoculationof a culture plate or a molecular assay to increasesensitivity.66
Traditional screening agars for VRE from stoolspecimens include Campylobacter medium with 5antibiotics, including 10 �g/mL of vancomycin, and
various types of bile esculin azide agar with vanco- oMayo Clin Proc. � March 2012;87(3):290-308 � doi:10.1016/j.mayocwww.mayoclinicproceedings.org
mycin.68,69 The traditional VRE screening agars re-uire 24 to 48 hours to identify colonies preliminar-
ly, with additional time required for confirmatorydentification and susceptibility testing and up to 5ays to final identification. Various chromogenicRE media demonstrate adequate sensitivity andpecificity, with reduced turnaround time to resultshrough early visual colony identification. There areany selective and differential chromogenic VRE
gars that appear promising for use in VRE stoolcreening. However, performance data vary accord-ng to whether prior overnight broth enrichment ofhe specimen in liquid media was performed.67
Real-time PCR is a sensitive and rapid approacho the identification of VRE from gastrointestinalract specimens.66 Recently, the BD GeneOhm VanR
(BD Diagnostics, Spark, MD) and Xpert vanA/vanB(Cepheid, Sunnydale, CA) assays, which detect iso-lates carrying vanA and vanB genes within 2 to 4
ours, have been introduced.70 Most FDA-clearedssays have been marketed for direct detection ofRE from rectal or perianal swabs, although detec-
ion from stool specimens has shown comparableesults. Some studies have demonstrated improvederformance of molecular assays after overnight aer-bic or anaerobic preenrichment of stool in brothedia; however, the preenrichment step increases
he turnaround time to results.70 Occasionally,ower specificity has been shown with the use oferianal sampling due to the presence of anaerobeshat carry the vanB gene.69
In summary, there are a variety of VRE screen-ng methods available, the most promising of whichppear to be chromogenic media and molecular as-ays, due to rapid result reporting. However, somessays require an overnight preenrichment step toaximize sensitivity.
LINDAMYCIN RESISTANCE IN STREPTOCOCCIND STAPHYLOCOCCIlindamycin and erythromycin resistance in strep-
ococci may either be due to erm genes, which leado the production of macrolide ribosomal methyl-ses, or to expression of the mef gene, which encodesn efflux pump targeting only the macrolides. Byomparison, erm enzymes methylate the 23S ribo-omal RNA component of the 50S bacterial ribo-omal subunit, which causes decreased binding ofacrolides, lincosamides (clindamycin), and strep-
ogramin B antibiotics (designated the MLSB pheno-ype). In staphylococci, inducible clindamycin resis-ance is also due to the MLSB phenotype, but itsfflux pump is encoded by the msrA gene.
The MLS resistance phenotype can be either in-uced or constitutively expressed. Inducible clinda-ycin resistance cannot be detected by routine MIC
r disk testing of clindamycin.71 Therefore, the 14-
p.2012.01.007 299

tapmr
D
EMimamcad
MAYO CLINIC PROCEEDINGS
300
and 15-member macrolides, which are better induc-ers of clindamycin resistance than is clindamycinitself, must be used for induction of clindamycin inthe clinical laboratory.72 Testing of streptococci andstaphylococci for inducible clindamycin resistanceis important because clindamycin is frequently usedto treat staphylococcal, group B streptococcal, andgroup A streptococcal infections. In addition, resis-tance to clindamycin is increasing in prevalence,with a recent estimate of 12.8% inducible clindamy-cin resistance among S aureus in the United States.73
Both inducible and constitutive clindamycin resis-tance has likewise become increasingly commonamong �-hemolytic streptococci, with less resis-tance reported for group A streptococcal than forgroup B streptococcal infections.74
The CLSI has recommended 2 different meth-ods for detection of inducible clindamycin resis-tance in staphylococci and �-hemolytic strepto-cocci.5 One method is the disk approximation test,also known as the D-zone test. With this approach,separate erythromycin and clindamycin disks areplaced specific distances apart on an agar plate, de-pending on whether staphylococci or streptococciare being tested. If there is flattening of the zone ofinhibition between the 2 disks and the zone resem-bles the letter “D,” the test result is interpreted aspositive for induction of clindamycin resistance.The second method suggested by the CLSI is the useof a single-well microdilution test containing botherythromycin and clindamycin. Whenever induc-ible MLSB resistance is detected, clindamycin treat-ment should be avoided, if possible. However, theCLSI states in their guidelines that clindamycin maystill be clinically effective in some patients, despite apositive induction test result.
Automated methods for identification of induc-ible clindamycin resistance have also recently beenintroduced.75 Molecular assays using primers forvarious erm genes have been used in various re-search settings for the purpose of following resis-tance trends or validating BMD assays.71 However,PCR assays for inducible clindamycin resistance arenot currently considered the standard of care in theclinical microbiology laboratory.
Constitutive or inducible resistance to clinda-mycin may also be seen in S pneumoniae due to ex-pression of a ribosomal methylase encoded by theermB gene. The methylase alters the binding site onthe ribosomes for the macrolides and clindamycin,similar to that seen for �-hemolytic streptococci andstaphylococci.76 Clindamycin is recommended as asecond- or third-line antibiotic choice for pediatricpatients receiving long-term antibiotic therapy forsome conditions, such as pneumococcal osteomy-elitis and/or joint infections.77 Because pneumo-
cocci are capable of expressing inducible clindamy-Mayo Clin Proc. �
cin resistance, some authors suggest that isolatesof S pneumoniae be tested for erm-mediated resis-ance in certain clinical situations involving pedi-tric patients. Jorgensen et al77 recently assessederformance of the CLSI-suggested disk and BMDethods for detection of inducible clindamycin
esistance in pneumococci.
ETECTION OF EXTENDED-SPECTRUM�-LACTAMASE PRODUCTION AMONG
NTEROBACTERIACEAEembers of Enterobacteriaceae (and other organ-
sms, including P aeruginosa) can produce �-lacta-ases, referred to as extended-spectrum �-lactam-
ses (ESBLs), capable of hydrolyzing penicillins, theonobactam aztreonam, and cephalosporins (in-
luding expanded-spectrum cephalosporins, suchs cefotaxime, ceftriaxone, ceftizoxime, and ceftazi-ime).78 The CLSI guidelines specify screening cri-
teria and confirmatory testing approaches for detec-tion of ESBL production by Escherichia coli, Kpneumoniae, and Proteus mirabilis.5 For organismssuch as Enterobacter spp and Serratia spp, whichproduce AmpC-type enzymes, ESBL screeningshould not be performed because false-negative re-sults can occur. These screening and confirmatorytests were necessary because standard disk diffusionand MIC tests did not uniformly identify isolatesproducing ESBLs. Because ESBLs are usually inhib-ited by clavulanic acid, the CLSI made use of thisproperty in developing the tests recommended toclinical laboratories for their detection and recom-mending that isolates producing ESBLs be reportedas resistant to all penicillins, cephalosporins, andaztreonam. On establishment of new, lower inter-pretive criteria for many of these compounds,largely based on pharmacokinetic and pharmacody-namic principles and limited clinical data, the CLSIrevised their recommendations for reporting.5
When the new breakpoints are adopted by clinicallaboratories, the CLSI recommends that results forspecific cephalosporins and aztreonam be reportedand interpreted as they are tested and that the ESBLscreening and confirmatory tests need only be per-formed for epidemiological and infection controlpurposes. By comparison, although the EuropeanCommittee on Antimicrobial Susceptibility Testing(EUCAST) breakpoints for the cephalosporins aresimilar to those now recommended by the CLSI,EUCAST recommends that laboratories continue toscreen and confirm ESBL production due to the lim-ited supporting clinical data and that cephalosporinreports be changed from susceptible to intermediateor intermediate to resistant if an isolate tests positive
for ESBL production.79March 2012;87(3):290-308 � doi:10.1016/j.mayocp.2012.01.007www.mayoclinicproceedings.org

ptc
C
soAbMt
madmm
sqdr
TTlicf
LABORATORY TESTING TO GUIDE ANTIMICROBIAL THERAPY
DETECTION OF CARBAPENEMASE ACTIVITYAMONG ENTEROBACTERIACEAECarbapenemases, enzymes that hydrolyze carba-penem class antibiotics (ertapenem, imipenem,meropenem, and doripenem), usually hydrolyzeall other currently available �-lactams, with theexception of aztreonam for some metallo-�-lactamases. The genome encoding for the produc-tion of these enzymes may be located on plasmids(eg, K pneumoniae carbapenemases), a feature thatmakes them of particular concern from an infec-tion control perspective. There are 3 classes ofcarbapenemases: serine class A (including KPC,SME, IMI, GES, and NMC), class B enzymesknown as the metallo-�-lactamases (such as VIM,IMP, and NDM), and the class D OXA enzymes.80
Carbapenemases have been identified in a widerange of gram-negative genera. The KPC enzyme,the most frequently identified class A carbapen-emase in the United States, is most often found inthe Enterobacteriaceae but has also been detectedin P aeruginosa.81 Metallo-�-lactamases are mostfrequently seen in Acinetobacter spp and P aerugi-nosa, but recently NDM has become widespreadin some regions of the world among species ofEnterobacteriaceae, particularly K pneumoniae.OXA carbapenemases are most frequently foundin Acinetobacter spp but have also been reportedamong isolates of Enterobacteriaceae.
In 2009 the CLSI Subcommittee on Antimi-crobial Susceptibility Testing (SAST) recom-mended the modified Hodge test for the detectionof carbapenemase activity in Enterobactericeae.82
Advantages of this assay include its ease of perfor-mance, the ability to test several isolates on a sin-gle plate, and the detection of different classes ofcarbapenemases with one test.83,84 The primarydisadvantages are subjectivity in reading the re-sults, its inability to differentiate the various car-bapenemases (potentially useful from an epidemi-ological perspective), and the false-positiveresults that can occur with some organisms pro-ducing AmpC or ESBL enzymes.
The modified Hodge test was originally rec-ommended for the detection of carbapenemasesin bacteria for which carbapenem MICs were ele-vated but still fell within the susceptible range.When isolates tested positive, the SAST recom-mended that they be designated carbapenemase-producing strains in the patient report with awarning indicating that the therapeutic outcomesof patients infected with such organisms andtreated with the relevant carbapenem were un-known, particularly when alternative dosing reg-imens were used (eg, continuous or prolongedinfusion). In 2010, though, the SAST lowered the
carbapenem breakpoints to capture most carba- rMayo Clin Proc. � March 2012;87(3):290-308 � doi:10.1016/j.mayocwww.mayoclinicproceedings.org
enemase-producing strains, which would nowest either as resistant or intermediate to theseompounds.5 Implementation of the revised break-
points eliminates the need for laboratories to rou-tinely perform the modified Hodge test, althoughsuch testing may in some cases still be of value froman epidemiological or infection control perspective.A number of phenotypic tests allow detection anddifferentiation of class A (eg, inhibition by boronicacid) and class C (eg, inhibition by chelating agentssuch as ethylenediaminetetraacetic acid) carbapen-emases, but these tests fail to detect class D (OXA)and are primarily used for strain characterizationrather than for clinical purposes.
DETECTION OF PLASMID-MEDIATEDAMPC-TYPE �-LACTAMASES
hromosomally mediated, inducible, AmpC-type�-lactamases are produced by several gram-negativepecies. Often referred to as the ASPACE or ASPICErganisms, these include, but are not restricted to,eromonas spp, Serratia spp, P aeruginosa, Acineto-acter spp indole-positive Proteae (Providencia spp,organella morganii, and Proteus vulgaris), Citrobac-
er spp, and Enterobacter spp.85 Resistant to the cur-rently available �-lactamase inhibitors, such astazobactam, sulbactam, and clavulanic acid, these en-zymes result in resistance to a wide range of �-lactamantibiotics. The combination of a porin deletion withan AmpC-type enzyme can result in resistance to car-bapenems. The genome encoding AmpC-type �-lacta-
ases may also be harbored on transmissible plasmidsnd has been reported among a number of species thato not naturally produce inducible chromosomallyediated AmpC-type enzymes, including K pneu-oniae, E coli, P mirabilis, and Salmonella spp.86 Similar
to the plasmids carrying the genes encoding ESBLs,those with AmpC-type genes often harbor resistancedeterminants for multiple classes of drugs.
Because detection of plasmid-mediated AmpC-producing pathogens may have epidemiological andinfection control importance, several assays havebeen developed in an attempt to accurately detectthis resistance type.87-94 None, however, has beenufficiently standardized or tested against an ade-uate number of organisms producing plasmid-me-iated AmpC-type enzymes to be considered supe-ior in performance to the other assays.
ESTING TO DETECT BACTERICIDAL ACTIVITYhe AST methods used in the clinical microbiology
aboratory typically assess only the inhibitory activ-ties of antimicrobial agents. This is generally suffi-ient for patient management for most bacterial in-ections encountered by clinicians. In some, albeit
are, situations it may also be of value to determinep.2012.01.007 301

asbtnct
TATttoattctpao
cffibaaumoiwtboSMw
MAYO CLINIC PROCEEDINGS
302
the bactericidal activity of an antibiotic against aspecific patient bacterial pathogen. Serious infec-tions in which a bactericidal effect is generally con-sidered necessary for optimal treatment include bac-teremia in neutropenic patients, patients withchronic osteomyelitis, and patients with bacterialendocarditis.95-97
Minimum Bactericidal Concentration TestingAfter determination of MICs in a broth system understandard conditions, measured aliquots of growthmedia may be subcultured quantitatively to solidmedia to assess bactericidal activity. To calculate theextent of killing at each antibiotic concentration,plates are incubated under appropriate conditions,colony counts are performed, and results are com-pared to that of the growth control tube or well. Theaccepted definition of the minimum bactericidalconcentration (MBC) is the lowest concentration ofantibiotic at which a 99.9% (3 log) or greater reduc-tion in growth compared with the initial inoculum isobserved.98 As with the MIC, the antibiotic MBC isreported in micrograms per milliliter or in some re-gions of the world in milligrams per liter. Determi-nation of the MBC allows one to detect potentialtolerance by the patient’s specific isolate to an anti-biotic usually considered bactericidal, a phenome-non reportedly leading to clinical failure amongsome patients.99-101 Tolerance occurs when the an-tibiotic MIC for an organism is low (within the sus-ceptible range) but the MBC is elevated, frequentlyat a concentration beyond that generally consideredclinically achievable from a pharmacokinetic per-spective. Tolerance is specifically defined as an MBC32-fold or more higher than the MIC for the antibi-otic under consideration.98,100 Failure to demon-strate at least a 3-log10 decrease in colony-formingunits per milliliter in the time-kill assay is also con-sidered to represent tolerance.98
Time-Kill Kinetic AssaysTime-kill assays allow one to assess the rate of bac-tericidal activity at varying antibiotic concentrationsover time. Although these assays are time-consum-ing and laborious to perform because they requiresubculture of media at specific times during a 24-hour period, results of combinations of antimicro-bial agents can also be assessed. In 1999, standardmethods for performance of the assay were pub-lished by the CLSI (previously the National Com-mittee for Clinical Laboratory Standards).98 Resultsof time-kill assays are typically presented graphi-cally, plotting colony counts for each antimicrobialagent and concentration tested at each time point atwhich subcultures were performed (usually at 0, 4,
8, 12, and 24 hours). As with the MBC, bactericidalMayo Clin Proc. �
ctivity is defined as a 99.9% or greater killing at apecified time. When antibiotics are tested in com-ination using the time-kill approach, synergy isypically defined as a 2-log decrease or more in theumber of colony-forming units achieved with theombination of antibiotics when compared withhat achieved by the most active agent tested alone.
ESTS FOR ASSESSMENT OF INTERACTIONSMONG ANTIMICROBIAL AGENTShe value of in vitro testing to assess antibiotic in-
eractions (ie, synergy testing) remains highly con-roversial. With a few bacterial species and antibi-tic combinations, synergistic bactericidal activity isctually predictable and need not be routinely de-ermined (eg, ampicillin, penicillin, or a glycopep-ide plus gentamicin or streptomycin against sus-eptible strains of enterococci). When synergyesting is performed, the results should be inter-reted with caution because they do not take intoccount drug interactions from a pharmacokineticr a patient safety (adverse effect) perspective.
The checkerboard BMD test, wherein 2 antimi-robial agents are serially diluted in a 2-dimensionalashion to include all combinations during a speci-ed clinically relevant range, is a somewhat less la-or-intensive approach to assessing antibiotic inter-ctions in vitro than the time-kill assay. This samepproach to drug interaction testing can be takensing an agar dilution approach, although theethod is even more laborious. Using these meth-
ds, one is able to recognize synergistic, additive,ndifferent, or antagonistic interactions occurringith the agents being tested. By this method, a frac-
ional inhibitory concentration (�FIC) is calculatedy comparing the MIC of each drug alone to the MICf that drug in combination with the second agent.ynergy is usually defined as a 4-fold decrease in theIC of the agents in combination when comparedith the antibiotics tested alone.102 The FIC is cal-
culated and interpreted as follows:
�FIC � FIC of agent A � FIC of agent B
FIC of agent A �MIC of agent A in combination
MIC of agent A alone
FIC of agent B �MIC of agent B in combination
MIC of agent B alone
Synergy is defined as �FIC � 0.5
Indifference is defined as 0.5 � �FIC � 4
Antagonism is defined as �FIC � 4
Some investigators consider compounds additive
when �0.5 �FIC �1.March 2012;87(3):290-308 � doi:10.1016/j.mayocp.2012.01.007www.mayoclinicproceedings.org

aombapi
cr
e
s
LABORATORY TESTING TO GUIDE ANTIMICROBIAL THERAPY
The time-kill approach appears to correlate moreclosely with in vivo studies of combined antibiotic ef-fects than does the checkerboard method.103,104 Asimpler approach, albeit less standardized, is the use ofEtest strips. Using this method, synergy is again de-fined by the FIC as described earlier.105
SERUM BACTERICIDAL TESTING (SCHLICHTERASSAYS)Another approach to assessing bactericidal activityand determining the effects of antibiotic combina-tions is serum bactericidal testing. Determinationsof serum inhibitory titers and serum bactericidal ti-ters (SBTs) are performed in a manner analogous tothat for MIC and MBC testing, except that thepatient’s serum, rather than serially diluted concen-trations of antibiotic, is used. A guideline outliningthe specifics for performance of SBT testing has beenpublished by the CLSI.106 To perform the testing, 1or more blood samples are collected from the pa-tient (usually attempting to draw the specimenswhen antibiotic peak and trough levels areachieved). Serial 2-fold dilutions of the patient se-rum in pooled, pretested human serum are then pre-pared in tubes or wells of microtiter plates. Eachtube or well is then inoculated with a standardizedsuspension of the patient’s infecting pathogen in anapplicable growth medium. The serum inhibitorytiter is defined as the highest dilution of the patient’sserum preventing visible growth after an appropri-ate incubation period. Similar to MBC testing, quan-titative subcultures are then performed from eachdilution of the patient’s serum that prevented visiblegrowth. The SBT is defined as that dilution resultingin a 99.9% or greater decrease in the original inoc-ulum based on standardized rejection value tables.Results are then reported as titers (dilutions) of thepatient’s serum. The purpose of this assay is to de-termine whether the dosage regimen chosen fortreatment of the infection results in sufficient bacte-ricidal activity in the patient’s blood.96,107 Higherserum titers suggest that adequate patient dosinghas been achieved, unexpected antibiotic elimina-tion has not occurred, and the bacterial pathogen isnot tolerant. A peak SBT of 1:64 or higher and atrough SBT of 1:32 or higher have been shown tocorrelate with rapid bacterial eradication from theblood and optimal time to cardiac vegetation steril-ization in cases of endocarditis.96,108 Lower bacteri-cidal titers, however, do not necessarily predict apoor clinical response. Limited data have indicatedthat in cases of acute and chronic osteomyelitis apeak SBT of 1:16 or higher and a trough SBT of 1:4or higher are predictive of therapeutic efficacy.96,109
Major disadvantages of this assay include its labor-
intensive nature and the requirement to obtain, pre- pMayo Clin Proc. � March 2012;87(3):290-308 � doi:10.1016/j.mayocwww.mayoclinicproceedings.org
pare, and pretest pooled human serum for use in theprocedure.
ANTIFUNGAL SUSCEPTIBILITY TESTINGThere have been major advances in the standardiza-tion and clinical interpretation of antifungal suscep-tibility testing in recent years. The number of anti-fungal agents is increasing as the incidence ofsystemic and other infections due to Candida spp,Aspergillus spp, Zygomycetes, and other filamentousfungi is increasing.110 Susceptibility testing of clin-ically significant isolates, especially those from usu-ally sterile sites, is important both epidemiologicallyand clinically for guiding treatment. Antifungal sus-ceptibility testing standards for yeasts and moldshave been developed by both the CLSI and Euro-pean Committee on Antimicrobial SusceptibilityTesting (EUCAST) for a variety of antifungalagents.111-115
The standard antifungal reference testing methodgainst which many other susceptibility testing meth-ds are measured is the BMD method.112 The BMDethods proposed by different organizations vary
y the media used, supplements and inoculumdded, incubation conditions, and end point inter-retations. The CLSI provides MIC breakpoint and
nterpretive data for Candida spp for several antifun-gal agents, including fluconazole, itraconazole, vori-conazole, anidulafungin, caspofungin, micafungin,and flucytosine.111 The CLSI breakpoints for flu-onazole, voriconazole, and the echinocandins haveecently been revised for Candida species.116-118
The susceptible dose-dependent category for theazoles infers that susceptibility to these antifungalsby Candida spp is dependent on achieving the max-imal possible blood level. In addition, the flucona-zole data for the CLSI breakpoints were gatheredfrom studies involving patients with oropharyngealcandidiasis and invasive candidal infections in non-neutropenic patients. Therefore, the clinical rele-vance of fluconazole breakpoints in clinical situa-tions other than those mentioned has not beenestablished. Interpretive data for the echinocandinclass of drugs are based primarily on experiencewith nonneutropenic patients with candidemia, andclinical relevance of these data in other patient pop-ulations is uncertain. Finally, itraconazole data arebased on experience with mucosal infections only,and data supporting the CLSI breakpoints for inva-sive infections are not available. Although there areno CLSI breakpoints currently approved for ampho-tericin B when testing Candida spp, isolates forwhich the MICs are greater than 1.0 �g/mL are gen-rally considered resistant.111 Although the CLSI
documents only provide guidelines for Candida spp,ome investigators have applied the CLSI break-
oints to Cryptococcus spp, and correlations havep.2012.01.007 303

pinrapvtnrwrpAiaci
MAYO CLINIC PROCEEDINGS
304
been demonstrated between higher MICs and treat-ment failures.119
Because the BMD testing method is difficult toperform in daily practice in clinical microbiologylaboratories, other testing approaches have been in-vestigated. Disk diffusion antifungal susceptibilitytesting is a simple and cost-effective method for bothyeasts and molds. Fluconazole disk diffusion testingof Candida spp has been available for several years.The CLSI has also established guidelines for diskdiffusion testing of filamentous fungi, which is arelatively simple, rapid, and cost-effective alterna-tive to BMD testing.115 Etests are likewise less laborintensive than BMD and are relatively simple andreproducible for the testing of antifungal agents, es-pecially against molds.120 Sensititre YeastOne (TrekDiagnostic Systems) is a colorimetric antifungal sus-ceptibility testing MIC plate that exhibits high agree-ment with the CLSI BMD method.121 A new diskagar diffusion method, the Neo-Sensitabs tablet dif-fusion assay (Rosco, Taastrump, Denmark) has alsobeen developed and tested for antifungal testing ofmolds and yeasts.122 Finally, commercial auto-mated systems for MIC determination of yeasts aresimple alternative methods and are comparable toother established antifungal susceptibility testingmethods.123
Antifungal susceptibility testing of Candida albi-cans and other Candida spp is fairly simple to per-form, with determination of fluconazole susceptibil-ity as the most important first step. If the C albicansisolate is fluconazole resistant or if the isolate isnon–C albicans, further susceptibility testing will of-ten be required. In contrast, antifungal susceptibilitytesting of molds is not currently as useful clinicallybecause of both the long turnaround time of suchtesting and the difficulties in developing accuratebreakpoints for molds.124
CONCLUSIONThe goal of this article was to provide a review ofcurrent concepts in laboratory methods and ap-proaches that serve to assist clinicians in makingoptimal antibiotic decisions for treatment of infec-tions in this era of ever-evolving antimicrobial resis-tance. By its nature, the review could not be all-inclusive. For example, a standard has beendeveloped for the susceptibility testing of Myco-plasma spp and Ureaplasma urealyticum.125 Until re-cently, M pneumoniae, an important cause of com-munity-acquired pneumonia, was thought to beuniversally susceptible to the macrolide class of an-tibiotics. Not only has macrolide resistance nowbeen reported, but it is in fact widespread in somecountries, including China and Israel, renderingavailability of standardized methods for testing,
heretofore of limited value but now of clinical im-Mayo Clin Proc. �
ortance.126,127 A topic that warrants considerations the influence and effect of standards-setting orga-izations (eg, CLSI, EUCAST, and FDA) on AST andeporting. This is, however, beyond the scope of thisrticle but has been addressed in another recentublication.128 Many of the testing approaches re-iewed in these discussions have been used, essen-ially unchanged, for decades. As molecular tech-iques increasingly become a part of the dailyoutine in clinical laboratories, the day may comehen such highly sensitive and specific methods
eplace many of the assays currently being used toredict antimicrobial susceptibility and resistance.s bacterial pathogens continue to exhibit increas-
ng antibiotic resistance and appropriate empiricalntibiotic decisions become more and more diffi-ult, AST will take on an even more important rolen managing patient infections.
Correspondence: Address to Stephen G. Jenkins, PhD,Department of Pathology, Weill Cornell Medical College,East 68th Street, Starr 737A, New York, NY 10065([email protected]). Individual reprints of this articleand a bound reprint of the entire Symposium on Antimi-crobial Therapy will be available for purchase from ourWeb site www.mayoclinicproceedings.org.
The Symposium on Antimicrobial Therapy will continuein an upcoming issue.
REFERENCES1. Boucher HW, Talbot GH, Bradley JS, et al. Bad bugs, no
drugs: no ESKAPE! an update from the Infectious DiseaseSociety of America. Clin Infect Dis. 2009;48(1):1-12.
2. Clinical and Laboratory Standards Institute. Methods for Dilu-tion Antimicrobial Susceptibility Tests for Bacteria That GrowAerobically. Approved standard, 9th ed. Wayne, PA: Clinicaland Laboratory Standards Institute; 2012. CLSI publicationM7-A9.
3. International Organization for Standardization. SusceptibilityTesting of Infectious Agents and Evaluation of Performance ofAntimicrobial Susceptibility Devices, Part 1: Reference Methodfor Testing the In Vitro Activity of Antimicrobial Agents againstBacteria Involved in Infectious Diseases. Vol. ISO/DIS 20776-1.Geneva, Switzerland: International Organization for Stan-dardization; 2006.
4. Clinical and Laboratory Standards Institute. Performance Stan-dards for Antimicrobial Disk Susceptibility Tests. Approved stan-dard, 11th ed. Wayne, PA: Clinical and Laboratory StandardsInstitute; 2012. CLSI publication M02-A11.
5. Clinical and Laboratory Standards Institute. Performance Stan-dards for Antimicrobial Susceptibility Testing. 21st informationalsupplement. Wayne, PA: Clinical and Laboratory StandardsInstitute; 2012. CLSI publication M100-S22.
6. Barry AL, Badal RE, Hawkinson RW. Influence of inoculumgrowth phase on microdilution susceptibility tests. J Clin Mi-crobiol. 1983;18(3):645-651.
7. Metzler CM, DeHaan RM. Susceptibility tests of anaerobicbacteria: statistical and clinical considerations. J Infect Dis.1974;130(6):588-594.
8. Clinical and Laboratory Standards Institute. Development of
In Vitro Susceptibility Testing Criteria and Quality ControlMarch 2012;87(3):290-308 � doi:10.1016/j.mayocp.2012.01.007www.mayoclinicproceedings.org

LABORATORY TESTING TO GUIDE ANTIMICROBIAL THERAPY
Parameters. Approved guideline, 3rd ed. Wayne, PA:
Clinical and Laboratory Standards Institute; 2008. CLSI
publication M23-A3.
9. Bauer AW, Kirby WM, Sherris JC, Turck M. Antibiotic sus-
ceptibility testing by a standardized single disk method. Am J
Clin Pathol. 1966;45(4):493-496.
10. Baker CN, Stocker SA, Culver DH, Thornsberry C. Compar-
ison of the E Test to agar dilution, broth microdilution, and
agar diffusion susceptibility testing techniques by using a spe-
cial challenge set of bacteria. J Clin Microbiol. 1991;29(3):533-
538.
11. Huang MB, Baker CN, Banerjee S, Tenover FC. Accuracy of
the E Test for determining antimicrobial susceptibilities of
staphylococci, enterococci, Campylobacter jejuni, and gram-
negative bacteria resistant to antimicrobial agents. J Clin Mi-
crobiol. 1992;30(12):3243-3248.
12. Pfaller MA, Jones RN. Performance accuracy of antibacterial
and antifungal susceptibility test methods: report from the
College of American Pathologists Microbiology Surveys Pro-
gram (2001-2003). Arch Pathol Lab Med. 2006;130(6):
767-778.
13. Clinical and Laboratory Standards Institute. Methods for An-
timicrobial Dilution and Disk Susceptibility Testing of Infrequently
Isolated or Fastidious Bacteria. Approved guideline, 2nd ed.
Wayne, PA: Clinical and Laboratory Standards Institute;
2010. CLSI publication M45-A2.
14. Goldstein EJ, Citron DM, Merriam CV, Abramson MA. Infec-
tion after elective colorectal surgery: bacteriological analysis
of failures in a randomized trial of cefotetan vs. ertapenem
prophylaxis. Surg Infect. 2009;10(2):111-118.
15. Lassmann B, Gustafson DR, Wood CM, Rosenblatt JE. Re-
emergence of anaerobic bacteremia. Clin Infect Dis. 2007;
44(7):895-900.
16. Robert R, Deraignac A, Le MG, Ragot S, Grollier G. Prog-
nostic factors and impact of antibiotherapy in 117 cases of
anaerobic bacteremia. Eur J Clin Microbiol Infect Dis. 2008;
27(8):674-678.
17. Salonen JH, Eerola E, Meurman O. Clinical significance and
outcome of anaerobic bacteremia. Clin Infect Dis. 1998;26(6):
1413-1417.
18. Wilson JR, Limaye AP. Risk factors for mortality in patients
with anaerobic bacteremia. Eur J Clin Microbiol Infect Dis.
2004;23(4):310-316.
19. Zahar JR, Farhat H, Chacaty E, Meshaka P, Antoun S, Niten-
berg G. Incidence and clinical significance of anaerobic bac-
teremia in cancer patients: a 6-year retrospective study. Clin
Microbiol Infect. 2005;11(9):724-729.
20. Baron EJ, Citron DM, Wexler HM. Son of anaerobic suscep-
tibility testing – revisited. Clin Microbiol Newsletter. 1990;
12(9):69-70.
21. Dougherty SH. Antimicrobial culture and susceptibility test-
ing has little value for routine management of secondary
bacterial peritonitis. Clin Infect Dis. 1997;25(suppl 2):S258-
S261.
22. Finegold SM. Perspective on susceptibility testing of anaero-
bic bacteria. Clin Infect Dis. 1997;25(suppl 2):S251-S253.
23. Rosenblatt JE, Brook I. Clinical relevance of susceptibility
testing of anaerobic bacteria. Clin Infect Dis. 1993;16(suppl
4):S446-S448.
24. Wilson SE, Huh J. In defense of routine antimicrobial suscep-
tibility testing of operative site flora in patients with perito-
nitis. Clin Infect Dis. 1997;25(suppl 2):S254-S257.
Mayo Clin Proc. � March 2012;87(3):290-308 � doi:10.1016/j.mayocwww.mayoclinicproceedings.org
25. Golan Y, McDermott LA, Jacobus NV, et al. Emergence offluoroquinolone resistance among Bacteroides species. J An-timicrob Chemother. 2003;52(2):208-213.
26. Nguyen MH, Yu VL, Morris AJ, et al. Antimicrobial resistanceand clinical outcome of Bacteroides bacteremia: findings of amulticenter prospective observational trial. Clin Infect Dis.2000;30(6):870-876.
27. Hecht DW, Osmolski JR, O’Keefe JP. Variation in the sus-ceptibility of Bacteroides fragilis group isolates from six Chi-cago hospitals. Clin Infect Dis. 1993;16(suppl 4):S357-S360.
28. Snydman DR, Jacobus NV, McDermott LA, et al. Nationalsurvey on the susceptibility of Bacteroides fragilis group: re-port and analysis of tends in the United States from 1997 to2004. Antimicrob Agents Chemother. 2007;51(5):1649-1655.
29. Snydman DR, Jacobus NV, McDermott LA, et al. Nationalsurvey on the susceptibility of Bacteroides fragilis group: re-port and analysis of trends for 1997-2000. Clin Infect Dis.2002;35(suppl 1):S126-S134.
30. Snydman DR, Jacobus NV, McDermott LA, et al. Multicenterstudy of in vitro susceptibility of the Bacteroides fragilis group,1995 to 1996, with comparison of resistance trends from1990 to 1996. Antimicrob Agents Chemother. 1999;43(10):2417-2422.
31. Clinical and Laboratory Standards Institute. Analysis and Pre-sentation of Cumulative Antimicrobial Susceptibility Test Data.Approved guideline, 3rd ed. Wayne, PA: Clinical and Labo-ratory Standards Institute; 2009. CLSI publication M39-A3.
32. Clinical and Laboratory Standards Institute. Acceptable Anaer-obe Control Strain Ranges for Minimal Inhibitory Concentration(MIC) Determination by Broth Microdilution and Agar DilutionTesting and Cumulative Antimicrobial Susceptibility Report forBacteroides fragilis Group Bacteria. Approved standard infor-mational supplement. Wayne, PA: Clinical and LaboratoryStandards Institute; 2009. CLSI publication M11-S1.
33. Clinical and Laboratory Standards Institute. Methods for An-timicrobial Susceptibility Testing of Anaerobic Bacteria. Ap-proved standard, 7th ed. Wayne, PA: Clinical and LaboratoryStandards Institute; 2007. CLSI publication M11-A7.
34. Clinical and Laboratory Standards Institute. Susceptibility Test-ing of Mycobacteria, Nocardia spp., and Other Aerobic Actino-mycetes. Approved standard, 2nd ed. Wayne, PA: Clinicaland Laboratory Standards Institute; 2011. CLSI publicationM24-A2.
35. Brown-Elliott BA, Brown JM, Conville PS, Wallace RJ Jr.Clinical and laboratory features of the Nocardia spp. based oncurrent molecular taxonomy. Clin Microbiol Rev. 2006;19(2):259-282.
36. Verroken A, Janssens M, Berhin C, et al. Evaluation of matrix-assisted laser desorption ionization-time of flight mass spec-trometry for identification of Nocardia species. J Clin Microbiol.2010;48(11):4015-4021.
37. Wallace RJ Jr, Steele LC, Sumter G, Smith JM. Antimicrobialsusceptibility patterns of Nocardia asteroides. AntimicrobAgents Chemother. 1988;32(12):1776-1779.
38. Ambaye A, Kohner PC, Wollan PC, Roberts KL, Roberts GD,Cockerill FR III. Comparison of agar dilution, broth microdi-lution, disk diffusion, E-test, and BACTEC radiometric meth-ods for antimicrobial susceptibility testing of clinical isolates ofthe Nocardia asteroides complex. J Clin Microbiol. 1997;35(4):857–852.
39. Udhe KB, Pathak S, McCullum I Jr, et al. Antimicrobial-resis-tant Nocardia isolates, United States, 1995-2004. Clin Infect
Dis. 2010;51(12):1445-1448.p.2012.01.007 305

MAYO CLINIC PROCEEDINGS
306
40. Centers for Disease Control and Prevention. Initial therapyfor tuberculosis in the era of multidrug resistance: recom-mendations of the Advisory Council for the Elimination ofTuberculosis. MMWR Recomm Rep. 1993;42(RR-7):1-8.
41. Styrt BA, Shinnick TM, Ridderhof JC, Crawford JT, TenoverFC. Turnaround time for mycobacterial cultures. J Clin Micro-biol. 1997;35(4):1041-1042.
42. Kent PT, Kubica GP. Public Health Mycobacteriology: A Guidefor the Level III Laboratory. Atlanta, GA: Centers for DiseaseControl and Prevention; 1985. In: Clinical and LaboratoryStandards Institute. Susceptibility Testing of Mycobacteria, No-cardiae, and Other Aerobic Actinomycetes. Approved standard,2nd ed. Wayne, PA: Clinical and Laboratory Standards Insti-tute; 2011. CLSI publication M24-S2
43. Scarparo C, Ricordi P, Ruggiero G, Piccoli P. Evaluation of thefully automated BACTEC MGIT 960 system for testing sus-ceptibility of Mycobacterium tuberculosis to pyrazinamide,streptomycin, isoniazid, rifampin, and ethambutol and com-parison with the radiometric BACTEC 460TB method. J ClinMicrobiol. 2004;42(3):1109-1114.
44. Hoek K, Van Rie A, van Helden PD, Warren RM, Victor TC.Detecting drug-resistant tuberculosis: the importance ofrapid testing. Mol Diagn Ther. 2011;15(4):189-194.
45. Griffith DE, Askamit T, Brown-Elliott BA, et al. An officialATS-IDSA statement: diagnosis, treatment, and preventionof nontuberculous mycobacterial diseases. Am J Respir CritCare Med. 2007;175(4):367-416.
46. Hindler J. Antimicrobial susceptibility tests. In: Isenberg HD,ed. Essential Procedures in Clinical Microbiology. Washington,DC: American Society for Microbiology; 1997:105-154.
47. Leitch C, Boonlayangoor S. �-Lactamase tests. In: IsenbergHD, ed. Clinical Microbiology Procedures Handbook. Washing-ton, DC: American Society for Microbiology; 1992:5.3.1-5.3.8.
48. Dyke JW. �-Lactamases of Staphylococcus aureus. In: Hamil-ton-Miller JM, ed. �-Lactamases. London, England: AcademicPress; 1979:291-310.
49. Kaase M, Lenga S, Friedrich S, Szabados F, Sakinc T,Feibelkorn KR. Comparison of phenotypic methods for pen-icillinase detection in Staphylococcus aureus. Clin MicrobiolInfect. 2008;14(6):614-616.
50. Tang YW, Stratton CW. Staphylococcus aureus: an old patho-gen with new weapons. Clin Lab Med. 2010;30(1):179-208.
51. Malhotra-Kumar S, Haccuria K, Michiels M, et al. Currenttrends in rapid diagnostics for methicillin-resistant Staphylo-coccus aureus and glycopepetide-resistant Enterococcus spe-cies. J Clin Microbiol. 2008;46(5):1577-1587.
52. Flayhart D, Hindler JF, Bruckner DA, et al. Multicenter eval-uation of BBL CHROMagar MRSA medium for direct detec-tion of methicillin-resistant Staphylococcus aureus from sur-veillance cultures of the anterior nares. J Clin Microbiol. 2005;43(11):5536-5540.
53. Struelens MJ, Hawkey PM, French GL, Witte W, Tacconelli E.Laboratory tools and strategies for methicillin-resistant Staph-ylococcus aureus screening, surveillance and typing: state ofthe art and unmet needs. Clin Microbiol Infect. 2009;15(2):112-119.
54. Marlowe EM, Bankowski MJ. Conventional and molecularmethods for the detection of methicillin-resistant Staphylo-coccus aureus. J Clin Microbiol. 2011;49(9):S53-S56.
55. Paule SM, Pasquariello AC, Thomson RB Jr, Kaul KL, PetersonLR. Real-time PCR can rapidly detect methicillin-susceptible
and methicillin-resistant Staphylococcus aureus directly fromMayo Clin Proc. �
positive blood culture bottles. Am J Clin Pathol.2005;124(3):404-407.
56. Carey BE, Nicol L. The combined oxacillin resistance andcoagulase (CORC) test for rapid identification and predictionof oxacillin resistance in Staphylococcus species directly fromblood culture. J Clin Pathol. 2008;61(7):866-868.
57. Swenson JM, Ferraro MJ, Sahm DF, Clark NC, Culver DH,Tenover FC; National Committee for Clinical LaboratoryStandards Study Group on Enterococci. Multilaboratory eval-uation of screening methods for detection of high-level ami-noglycoside resistance in enterococci. J Clin Microbiol. 1995;33(11):3008-3018.
58. Chen Y, Marshall SA, Winokur PL, et al. Use of molecular andreference susceptibility testing methods in a multicenter eval-uation of MicroScan Dried Overnight Gram-Positive MICpanels for detection of vancomycin and high-level aminogly-coside resistances in enterococci. J Clin Microbiol. 1998;36(10):2996-3001.
59. Chow JW. Aminoglycoside resistance in enterococci. ClinInfect Dis. 2000;31(2):586-589.
60. Watanabe S, Kobayashi N, Quinones D, Nagashima S, Ue-hara N, Watanabe N. Genetic diversity of enterococci har-boring the high-level gentamicin resistance gene aac(6’)-Ie-aph(2’’)-Ia or aph(2’’)-Ie in a Japanese hospital. Microb DrugResist. 2009;15(3):185-194.
61. Yean CY, Yin LS, Lalitha P, Ravichandran M. A nanoplex PCRassay for the rapid detection of vancomycin and bifunctionalaminoglycoside resistance genes in Enterococcus species.BMC Microbiol. 2007;7:112.
62. Salgado CD. The risk of developing a vancomycin-resistantEnterococcus bloodstream infection for colonized patients.Am J Infect Control. 2008;36(10):S175-S178.
63. Tacconelli E, Cataldo MA. Vancomycin-resistant enterococci(VRE): transmission and control. Int J Antimicrob Agents. 2008;31(2):99-106.
64. Cetinkaya Y, Falk P, Mayhall CG. Vancomycin-resistant en-terococci. Clin Microbiol Rev. 2000;13(4):686-707.
65. Courvalin P. Vancomycin resistance in gram positive-cocci.Clin Infect Dis. 2006;42(suppl 1):S25-S34.
66. Gazin M, Lammens C, Goossens H, Malhotra-Kumar S. Eval-uation of GeneOhm VanR and Xpert vanA/vanB molecularassays for the rapid detection of vancomycin-resistant en-terococci [published online ahead of print June 12, 2011]. EurJ Clin Microbiol Infect Dis. doi 10.1007/s10096-011-1306-y.
67. Stamper PD, Shulder S, Bekalo P, et al. Evaluation of BBLCHROMagar VanRE for detection of vancomycin-resistantenterococci in rectal swab specimens. J Clin Microbiol. 2010;48(11):4294-4297.
68. Shigei J, Tan G, Shiao A, de la Maza LM, Peterson EM.Comparison of two commercially available selective media toscreen for vancomycin-resistant enterococci. Am J Clin Pathol.2002;117(1):152-155.
69. Marner ES, Wolk DM, Carr J, et al. Diagnostic accuracy of theCepheid GeneXpert vanA/vanB assay ver. 1.0 to detect thevanA and vanB vancomycin resistance genes in Enterococcusfrom perianal specimens. Diagn Microbiol Infect Dis. 2011;69(4):382-389.
70. Malhotra-Kumar S, Haccuria K Michiels M, et al. Currenttrends in rapid diagnostics for methicillin-resistant Staphylo-coccus aureus and glycopeptide-resistant enterococcus spe-cies. J Clin Microbiol. 2008;46(5):1577-1587.
71. Bowling JE, Owens AE, McElmeel ML, et al. Detection of
inducible clindamycin resistance in beta-hemolytic strepto-March 2012;87(3):290-308 � doi:10.1016/j.mayocp.2012.01.007www.mayoclinicproceedings.org

LABORATORY TESTING TO GUIDE ANTIMICROBIAL THERAPY
cocci by using the CLSI broth microdilution test and
erythromycin-clindamycin combinations. J Clin Microbiol.
2010;48(6):2275-2277.
72. Leclercq R. Mechanisms of resistance to macrolides and
lincosamides: nature of the resistance elements and their
clinical implications. Clin Infect Dis. 2002;34(4):482-492.
73. Richter SS, Heilmann KP, Dohrn CL, et al. Activity of ceftaro-
line and epidemiologic trends in Staphylococcus aureus iso-
lates collected from 43 medical centers in the United States
in 2009. Antimicrob Agents Chemother. 2011;55(9):4154-
4160.
74. Merino Diaz L, Torres Sanchez MJ, Aznar Martin J. Prevalence
and mechanisms of erythromycin and clindamycin resistance
in clinical isolates of beta-hemolytic streptococci of Lance-
field groups A, B, C, and G in Seville, Spain. Clin Microbiol
Infect. 2008;14(1):85-87.
75. Ji M, Lee M, Noh S, Kim MN. Evaluation of the performance
of the MicroScan Pos Breakpoint Combo Panel Type 28 for
susceptibility testing of Staphylococcus aureus: low-range min-
imum inhibitory concentration of vancomycin, cefoxitin
screening, and inducible clindamycin resistance detection.
Korean J Lab Med. 2010;30(6):637-646.
76. Jenkins SG, Farrell DJ. Increase in pneumococcus macrolide
resistance, United States. Emerg Infect Dis. 2009;15(8):1260-
1264.
77. Jorgensen JH, McElmeel ML, Fulcher LC, McGee L, Glennen
A. Evaluation of disk approximation and single-well broth
tests for detection of inducible clindamycin resistance in
Streptococcus pneumoniae. J Clin Microbiol. 2011;49(9):3332-
3333.
78. Dubois V, Arpin C, Noury P, Quentin C. Clinical strain of
Pseudomonas aeruginosa carrying a blaTEM-21 gene located on
a chromosomal interrupted TnA type transposon. Antimicrob
Agents Chemother. 2002;46(11):3624-3626.
79. European Committee on Antimicrobial Susceptibility Testing
website. www.eucast.org/epert_rules. Accessed October 31,
2011.
80. Queenan AM, Bush K. Carbapenemases: the versatile �-lac-
tamases. Clin Microbiol Rev. 2007;20(3):440-458.
81. Villegas MV, Lolans K, Correa A, Kattan JN, Lopez JA, Quinn
JP. First identification of Pseudomonas aeruginosa isolates pro-
ducing a KPC-type carbapenem-hydrolyzing �-lactamase. An-
timicrob Agents Chemother. 2007;51(4):1553-1555.
82. Clinical and Laboratory Standards Institute. Performance Stan-
dards for Antimicrobial Susceptibility Testing. Nineteenth infor-
mational supplement. Wayne, PA: Clinical and Laboratory
Standards Institute; 2009. CLSI publication M100-S19.
83. Anderson KF, Lonsway DR, Rasheed JK, et al. Evaluation of
methods to identify the Klebsiella pneumoniae carbapen-
emase in Enterobacteriaceae. J Clin Microbiol. 2007;45(8):
2723-2725.
84. Lee K, Chong Y, Shin HB, Kim YA, Yong D, Yum JH. Modified
Hodge and EDTA: disk synergy tests to screen metallo-beta-
lactamase producing strains of Pseudomonas and Acinetobac-
ter species. Clin Microbiol Infect. 2001;7(2):88-91.
85. Jacoby GA. AmpC �-lactamases. Clin Microbiol Rev. 2009;
22(1):161-182.
86. Philippon A, Arlet G, Jacoby GA. Plasmid-determined
Amp-C type �-lactamases. Antimicrob Agents Chemother.
2002;46(1):1-11.
87. Coudron PE, Moland ES, Thomson KS. Occurrence and
detection of AmpC �-lactamases among Escherichia coli,
Mayo Clin Proc. � March 2012;87(3):290-308 � doi:10.1016/j.mayocwww.mayoclinicproceedings.org
Klebsiella pneumoniae, and Proteus mirabilis isolates at aveterans medical center. J Clin Microbiol. 2000;38(5):1791-1796.
88. Black JA, Thomson KS, Pitout JDD. Use of �-lactamase in-hibitors in disk tests to detect plasmid-mediated AmpC�-lactamases. J Clin Microbiol. 2004;42(5):2203-2206.
89. Nasim K, Elsayed S, Pitout JDD, Conly J, Church DL, GregsonDB. New method for laboratory detection of AmpC �-lac-tamases in Escherichia coli and Klebsiella pneumoniae. J ClinMicrobiol. 2004;42(10)4799-4802.
90. Black JA, Thomson KS, Buynak JD, Pitout JD. Evaluation of�-lactamase inhibitors in disk tests for detection of plasmid-mediated AmpC �-lactamases in well-characterized clinicalstrains of Klebsiella spp. J Clin Microbiol. 2005;43(8):4168-4171.
91. Yagi T, Wachino J, Kurokawa H, et al. Practical methods usingboronic acid compounds for identification of class C �-lac-tamase-producing Klebsiella pneumoniae and Escherichia coli.J Clin Microbiol. 2005;43(6):2551-2558.
92. Coudron PE. Inhibitor-based methods for detection of plas-mid-mediated AmpC �-lactamases in Klebsiella spp. Esche-richia coli, and Proteus mirabilis. J Clin Microbiol. 2005;43(8):4163-4167.
93. Tan TY, Ng LSY, He J, Koh TH, Hsu LY. Evaluation ofscreening methods to detect plasmid-mediated AmpC inEscherichia coli, Klebsiella pneumoniae, and Proteus mirabilis.Antimicrob Agents Chemother. 2009;53(1):146-149.
94. Tenover FC, Emery SL, Spiegel CA, et al. Identification ofplasmid-mediated AmpC �-lactamases in Escherichia coli,Klebsiella spp. and Proteus species can potentially improvereporting of cephalosporin susceptibility testing results. J ClinMicrobiol. 2009;47(2):294-299.
95. Sculier JP, Klastersky J. Significance of serum bactericidal ac-tivity in gram-negative bacillary bacteremia in patients withand without granulocytopenia. Am J Med. 1984;76(3):429-435.
96. Reller RB. The serum bactericidal test. Rev Infect Dis. 1986;8(5):803-808.
97. DeGirolami PC, Eliopoulos G. Antimicrobial susceptibilitytests and their role in therapeutic drug monitoring. Clin LabMed. 1987;7(3):499-513.
98. Clinical and Laboratory Standards Institute/NCCLS. Methodsfor Determining Bactericidal Activity of Antimicrobial Agents.Wayne, PA: NCCLS; 1999. NCCLS document M26-A.
99. Denny AE, Peterson LR, Gerding DN, Hall WH. Seriousstaphylococcal infections with strains tolerant to bactericidalantibiotics. Ann Intern Med. 1979;139(9):1026-1031.
100. Handwerger S, Tomasz A. Antibiotic tolerance among clinicalisolates of bacteria. Rev Infect Dis. 1985;7(3):368-386.
101. Tuomanen E, Durack DT, Tomasz A. Antibiotic toleranceamong clinical isolates of bacteria. Antimicrob Agents Che-mother. 1986;30(4):521-527.
102. Saiman L. Clinical utility of synergy testing for multidrug-resistant Pseudomonas aeruginosa isolated from patients withcystic fibrosis: ‘the motion for.’ Paediatr Respir Rev. 2007;8(3):249-255.
103. Bayer AS, Morrison JO. Disparity between timed-kill andcheckerboard methods for determination of in vitro bacte-ricidal interactions of vancomycin plus rifampin versus meth-icillin-susceptible and –resistant Staphylococcus aureus. Antimi-crob Agents Chemother. 1984;26;(2):220-223.
104. Cappelletty DM, Ryback MJ. Comparison of methodologies
for synergism testing of drug combinations against resistantp.2012.01.007 307

1
1
1
1
1
1
1
1
1
1
MAYO CLINIC PROCEEDINGS
308
strains of Pseudomonas aeruginosa. Antimicrob AgentsChemother. 1996;40(3):677-683.
105. Pankey GA, Ashcraft DS. The detection of synergy betweenmeropenem and polymyxin B against meropenem-resistantAcinetobacter baumannii using Etest and time-kill assay. DiagnMicrobiol Infect Dis. 2009;63(2):228-232.
106. Clinical and Laboratory Standards Institute/NCCLS. Method-ology for the Serum Bactericidal Test. Wayne, PA: NCCLS;1999. NCCLS document M21-A.
107. Schlichter JG, MacLean H, Milzer A. Effective penicillin ther-apy in subacute bacterial endocarditis and other chronicinfections. Am J Med Sci. 1949;217(6):600-6083.
108. Weinstein MP, Stratton CW, Ackley A, et al. Multicentercollaborative evaluation of a standardized bactericidal test asa prognostic indicator in infective endocarditis. Am J Med.1985;78(2):262-269.
109. Weinstein MP, Stratton CW, Hawley HB, Ackley A, RellerLB. Multicenter collaborative evaluation of a standardizedbactericidal test as a predictor of therapeutic efficacy in acuteand chronic osteomyelitis. Am J Med. 1987;83(2):218-222.
110. Lass-Flörl C. The changing face of epidemiology of invasivefungal disease in Europe. Mycoses. 2009:52(3):197-205.
111. Clinical and Laboratory Standards Institute. ReferenceMethod for Broth Dilution Antifungal Susceptibility Testing ofYeasts. Third informational supplement. Wayne, PA: Clin-ical and Laboratory Standards Institute; 2008. CLSI publi-cation M27-S3.
112. Clinical and Laboratory Standards Institute. Reference Methodfor Broth Dilution Antifungal Susceptibility Testing of Yeasts.Approved standard, 3rd ed. Wayne, PA: Clinical and Labo-ratory Standards Institute; 2008. CLSI publication M27-A3.
113. Clinical and Laboratory Standards Institute. Method for Anti-fungal Disk Diffusion Susceptibility Testing of Yeasts. Approvedguideline, 2nd ed. Wayne, PA: Clinical and Laboratory Stan-dards Institute; 2009. CLSI publication M44-A2.
114. Clinical and Laboratory Standards Institute. ReferenceMethod for Broth Dilution Antifungal Susceptibility Testing ofFilamentous Fungi. Approved standard, 2nd ed. Wayne, PA:Clinical and Laboratory Standards Institute; 2008. CLSIpublication M38-A2.
115. Clinical and Laboratory Standards Institute. Method for Anti-fungal Disk Diffusion Susceptibility Testing of NondermatophyteFilamentous Fungi. Approved guideline. Wayne, PA: Clinicaland Laboratory Standards Institute; 2010. CLSI publicationM51-A.
116. Pfaller MA, Andes D, Arendrup MC, et al. Clinical break-points for voriconazole and Candida spp. revisited: review ofmicrobiologic, pharmacodynamics, and clinical data as theypertain to the development of species-specific interpretivecriteria. Diagn Microbiol Infect Dis. 2011;70(3):330-343.
117. Pfaller MA, Andes D, Diekema DJ, Espinel-Ingroff A. Wild-
type MIC distributions, epidemiological cutoff values and spe-Mayo Clin Proc. �
cies-specific clinical breakpoints for fluconazole and Candida:time for harmonization of CLSI and EUCAST brothmicrodilution methods. Drug Resist Updat. 2010;13(6):180-195.
118. Pfaller MA, Diekema DJ, Andes D, et al. Clinical breakpointsfor the echinocandins and Candida revisited: integration ofmolecular, clinical, and microbiological data to arrive atspecies-specific interpretive criteria. Drug Resist Updat.2011;14(3):164-176.
19. Pfaller MA, Castanheira M, Diekema DJ, Messer SA, JonesRN. Wild-type MIC distributions and epidemiologic cutoffvalues for fluconazole, posaconazole, and voriconazole whentesting Cryptococcus neoformans as determined by the CLSIbroth microdilution method. Diagn Microbiol Infect Dis. 2011;71(3):252-259.
20. Martos AI, Romero A, González MT, et al. Evaluation of theE-test method for susceptibility testing of Aspergillus spp. andFusarium spp. to three echinocandins. Med Mycol. 2010;48(6):858-861.
21. Pfaller MA, Chatuverdi V, Diekema DJ, et al. Clinical evalua-tion of the Sensititre YeastOne colorimetric antifungal panelfor antifungal susceptibility testing of the echinocandinsanidulafungin, caspofungin, and micafungin. J Clin Microbiol.2008;46(7):2155-2159.
22. Espinel-Ingroff A, Arthington-Skaggs B, Iqbal N, et al. Multi-center evaluation of a new disk agar diffusion method forsusceptibility testing of filamentous fungi with voriconazole,posaconazole, itraconazole, amphotericin B, and caspofungin.J Clin Microbiol. 2007;45(6):1811-1820.
23. Peterson JF, Pfaller MA, Diekema DJ, Rinaldi MG, Riebe KM,Ledeboer NA. Multicenter comparison of the Vitek 2 anti-fungal susceptibility test with the CLSI broth microdilutionreference method for testing caspofungin, micafungin, andposaconazole against Candida spp. J Clin Microbiol. 2011;49(5):1765-1771.
24. Klutts JS, Robinson-Dunn B. A critical appraisal of the role ofthe clinical microbiology laboratory in diagnosis of invasivefungal infections. J Clin Microbiol. 2011;49(9):S39-S42.
25. Clinical and Laboratory Standards Institute. Methods for Anti-microbial Susceptibility Testing for Human Mycoplasmas. Ap-proved guideline. Wayne, PA: Clinical and Laboratory Stan-dards Institute; 2011. CLSI publication M43-A.
26. Cao B, Zhao CJ, Yin YD, et al. High prevalence of macrolideresistance in Mycoplasma pneumoniae isolates from adult andadolescent patients with respiratory tract infection in China.Clin Infect Dis. 2010;51(2):189-194.
27. Averbuch D, Hidalgo-Grass C, Moses AE, Engelhard D, Nir-Paz R. Macrolide resistance in Mycoplasma pneumoniae, Israel,2010. Emerg Infect Dis. 2011;17(6):1079-1082.
28. Jenkins SG, Jerris RC. Critical assessment of issues applicableto development of antimicrobial susceptibility testing break-
points. J Clin Microbiol. 2011;49(9, suppl):S5-S14.March 2012;87(3):290-308 � doi:10.1016/j.mayocp.2012.01.007www.mayoclinicproceedings.org