Embed Size (px)
Citation preview

Critical Care Human Resources and Delivery Models
Kim Macfarlane - Fraser Health, Clinical Nurse Specialist Tertiary Critical Care
Contributors:Karen Watson – Fraser Health, Program
Director Critical Care Dr Bill Henderson, President, BC Society of
Critical Care Medicine
March 7, 2012

Context
• With an increasing and aging population, the demand for critical care services continues to rise
• This is juxtaposed with multiple factors including:– The public’s expectations for timely access and high
quality care– High utilization of critical care beds– Increasing costs and finite healthcare dollars– Current and alarming projected shortages in all care
healthcare professionals including nurses, respiratory therapists, intensivists and so on!

Overview of Components Underpinning Care Model Redesign
• Population geographics, demographics and needs• Finite healthcare dollars• Levels of ICUs and patient flow• Multi-professional shortages• Scopes of practice• Unit design• Technology• Recruitment and retention• Quality and other metrics

**Data requires updating based upon new (2012) Census results

Source: BCStats

**Data requires updating based upon new (2012) Census results

International and National Critical Care Beds
• Internationally, critical care services vary dramatically between countries with considerable differences in both numbers of beds and volume of admissions
• Canada has about 6.7 critical care beds per 100,000 persons. This value is somewhat higher than England’s (4.7 per 100,000) and substantially lower than the United States (25 per 100,000)
• In part, these differences are attributable to the variation in the definition of an ICU patient and thus bed. The number of ICU beds per capita is not strongly correlated with overall healthcare expenditure, but does correlate strongly with mortality [Wunsch, H., Angus, D., Harrison, D., Collange, O., Fowler, R.,et al.; (2008). Variation in critical care services across North America and Western Europe. Crit Care Med. 36: 2787-293]

BC Critical Care Beds
• BC population of 4.6 million (BCStats, Oct/11)• The annual all-inclusive cost of one ventilator bed
is 1.2 million dollars• Survey data: 255 critical care beds across health
authorities (Critical Care Survey Analysis PCCWG/MoHS Oct 2010 Oct/10):
***Data requires refresh

BC Levels of Critical Care Units

BC Distribution of Levels of Critical Care Units
Critical Care Survey Analysis PCCWG/MoHS Oct 2010 Oct/10

Opportunities and Challenges• High and increasing demand for critical care services• Population access – hospital proximities, suburban vs. rural/remote
areas• Timeliness of access – reliance on BC Ambulance services for initial
and subsequent transport• Hierarchical levels of critical care:
– Ensuring patient needs are matched with interdisciplinary expertise (e.g. synergy model)
– Necessary for critical mass, quality outcomes and cost containment• ICU patient utilization and flow
– Levels of units – network of provincial/regional beds– Admission/Discharge criteria– Development of high acuity units at larger centres– ICU outreach programs
• Increasing need for a variety of metrics - ICU database

Critical Care Services within Multi-Professional Shortages

Projected Nursing Shortage
• The nursing shortage is an international problem• Like Canada, the United Kingdom, United States
and several other countries have reported alarming projections
• The United States is projecting a shortfall of up to half a million nurses by 2024
• A recent report published by the Canadian Nurses Association (CNA, 2009) is predicting that Canada “will be short almost 60,000 full-time equivalent nurses by 2022”

Fraser Health Critical Care Nursing Workforce
• 338 nursing fulltime equivalents (FTEs) across 8 ICUs
• 7% vacancy rate (all forms)• 4.7% turnover rate• National critical care nursing turnover rate
27% (O’Brien-Pallas, Tomblin, Murphy & Shamian, 2008)

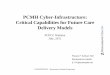
Fraser Health Critical Care Nursing Demographics (N= 653)

Fraser Health Critical Care Nursing Demographics
• Further contributing to the shortage is the high levels of upcoming retirements
• Out of the total 653 nurses, there are 152 (23.3%) who are age 50 or older and thus 5 or less years away from potential retirement
• Also, this age distribution identifies the high number of nurses who are within child bearing age and thus there is the potential for a number of annual absences through maternity leaves

Nursing Education and Workforce• Nationally, educational institutions continue to add seats,
but have high attrition rates• Up to 40% of new graduates leave the workplace and/or
profession within the first seven years• Critical care practice requires “prior experience” or
additional specialty education, but entry to practice varies nationally
• Provincial work is underway to establish specialty program core competencies and streams (e.g. tertiary, rural etc.)
• Currently within BC, the total cost of fulltime enrollment for a nurse in the critical care program is approximately $33,000.00; the total cost of fulltime enrollment for a nurse in the high acuity is approximately $16,300.00

Fraser Health Respiratory Therapist Workforce
• 266 fulltime equivalents (FTEs) across FH• Highest concentration within critical care• 12% vacancy rate (all forms)• ?? % turnover rate

Fraser Health Respiratory Therapist Demographics (N=266)

Fraser Health Respiratory Therapist Demographics
• Somewhat younger age distribution than nursing
• Out of the total 266 respiratory therapists, there are 37 (13.9%) who are age 50 or older and thus 5 or less years away from potential retirement

Respiratory Therapist Education
• Only one educational institution in BC• Recent graduation data from Thompson
Rivers University (TRU):– 2013 68 – 2012 48 * new 3 yr diploma vs 4 yr Health Science Bachelor degree option
– 2005 – 2009 approx 50 /yr

Respiratory Therapist Education
• Over the past few years, TRU has added about 20 seats to the program with laddering opportunities (e.g. students who have a degree prior to entering the program can ladder into the second year of the program; and all first year students have the option of completing either the three year diploma program or a four year bachelor of health science program)
• This program redesign has created a short-term reduction in graduates: 2012 projected graduates 48; 2013 projected graduates 68; 2014 projected graduates 70

Respiratory Therapist Workforce
• In BC, single certification enhances distribution
• National education programs have differing curriculum
• Variable salaries across the country promote movement; the current hourly wage difference between BC and Alberta is $8.83 (BC $32.67; Alb $41.50)

Intensivist
• Intensivist (Critical Care fellowship) resources are not an issue in BC at this time
• Issue is the opportunity/need to create ICU positions that Intensivists would be appropriate to recruit into
• Intensivist lead ICU s have improved outcomes

Intensivist• Intensivists need closed ICUs where they have some ability to
influence/manage quality of care
• Should there be a push to consolidate units that support the activity (high volume) and level of acuity needed to maintain clinical expertise
• Balancing measure will be timely access and an appropriate number (capacity) of larger sites
• High volume centers should have Intensivist supports inplace to ensure quality work

Key Considerations in Care Model Redesign
• Any planning for the redesign of critical care delivery models must be simultaneously situated within system and local contexts. With the current and projected shortages, the first question becomes a broader one for policy makers within hospital systems
• Where would hospitals like to deploy the highest concentration of skilled professionals? If it is in speciality areas and in this case critical care, then this obligates a further examination and redesign of care models within other hospital units

Key Considerations in Care Model Redesign
• Any form of critical care model redesign must be predicated upon safety, quality, and cost
• At the same time, it must maintain the resilience of patient/family care and relationships among the interdisciplinary team

Baseline Workload Analysis
• Using specific critical care valid/reliable workload tools to establish the breadth of professional work
• Cautionary note in terms of:– Must analyze thinking within task (e.g. bed bath
incorporates nursing assessment)– Safety related redundancies are not duplication

Can Some Activities be Removed, Augmented or Reassigned?
• Opportunities for LEAN methodology
• There needs to be an reanalysis of each profession’s practice and determining what aspects of this work can be eliminated, delegated or augmented within the context of quality patient/family care, interdisciplinary team practice and cost-effectiveness
• Adding more staff to the mix can increase the risk of communication breakdown and sentinel events


Unit Design Constructs and Constrains Care Delivery Models
• Advantages and disadvantages for patients, families and staff
Open
Single Room

Technology• Since the 1970’s, the critical care literature
has made predictions about technologic advances poised to improve patient outcomes and reduce workforce costs
• Certainly, there are many advances that have improved patient outcomes, but there are none to replace critical care clinicians
• In many respects, the introduction of multiple patient monitoring and interventional technologies has added another layer of prerequisite knowledge and complexity to interdisciplinary critical care practice

eICUs• This system uses a combination
of technologies, such as remote patient monitoring and two-way audio/video teleconferencing to monitor patient status and direct patient care, as appropriate. From a remote location, either in a central hub within an ICU or from an off-site command centre, critical care nurses and/or physicians oversee all aspects of patient care and can converse with caregivers

Nursing Recruitment Strategies
• Experienced ICU nurses (increasingly rare)• Clinical laddering• Medical/surgical nurses who are recruited and
graduate from specialty education• New graduates – highly selective process with
established mentors and then completion of specialty education
• International nurses

A Renewed Emphasis on Retention
• The AACN has developed standards for “healthy workplaces”
• “Magnet Hospital” research has identified a series of key strategies with proven outcomes: lower turnover rates and higher levels of job satisfaction
• On the Canadian scene, there is an abundance of literature published the CNA and other professional organizations. There is new document on teamwork. In addition, provincially-based Ministries of Health have published a number of white papers on recruitment and retention

Discussion• Our future will look different than present day practice:
– What are our major concerns?– What are our learnings and successes?– Where are the opportunities?– How can we collaborate provincially?