Embed Size (px)
Citation preview

1
Condylar FractureA
Dr. Amit T. Suryawanshi
Literature
Click herewww.faceart-clinic.com
Dr. Amit T. Suryawanshi (MDS) Facial Cosmetic SurgeonOral & Maxillofacial SurgeonDental Surgeon & ImplantologistHair Transplant Surgeon (Germany)
Consulting Surgeon in Kolhapur, Sangli, Pune & Mumbai (India) & founder of Face Art International Super specialityat Kolhapur
Cell Phone no. +91 9405622455 Clinic Landline - +91 7758976097 Email– [email protected]

2
Annual Global Road Crash Statistics - Nearly 1.3 million people die in road crashes each year, on average 3,287 deaths a day. An additional 20-50 million are injured or disabled. More than half of all road traffic deaths occur among young adults ages 15-44. Road traffic crashes rank as the 9th leading cause of death and account for 2.2% of all
deaths globally. Road crashes are the leading cause of death among young people ages 15-29, and the
second leading cause of death worldwide among young people ages 5-14. Each year nearly 400,000 people under 25 die on the world's roads, on average over
1,000 a day. Over 90% of all road fatalities occur in low and middle-income countries, which have
less than half of the world's vehicles. Road crashes cost USD $518 billion globally, costing individual countries from 1-2% of
their annual GDP. Road crashes cost low and middle-income countries USD $65 billion annually,
exceeding the total amount received in developmental assistance. Unless action is taken, road traffic injuries are predicted to become the fifth leading
cause of death by 2030.
In the present time, when human beings have to race against time to live a comfortable life,
we need to overlook the danger that may follow and still we are more subjected to trauma.
Also, when the rule of survival of fittest exists, first flights and assaults becomes a feature of
everyday life. Chin, being the most prominent part of the face, has to bear with blows,

3
resulting in fracture of the mandible. Automobile, sports and industrial accidents also
contribute towards fracture of mandible.
The condylar process, forms an important component of the temporomandibular joint and
takes part in proper functioning of the T.M.J. Also proper occlusion and facial appearances
depends upon the integrity of the condylar process.
The oldest study of the condylar fracture was made by Desault in 1805, who recognized the
importance of restoring the contact with the fragment and stated that the union might fail to
take place, if slightest movement of the jaw occurred.
The term condylar fracture can be applied to fracture of the condylar process which occurs
between the sigmoid notch and up to the including articular surface of the condyle.
Condylar fracture may be either unilateral or bilateral and occurs as a result of indirect blow,
i.e. when a blow is sustained centrally upon the point of the chin, the forces of the impact is
transmitted upwards and backwards along the length of the bone, to the point where the
mandible articulates with the skill. Condylar fractures are more common due to the frail neck
of the condyle which snaps when a blow is received on the chin and directed along the
ramous of the mandible. If the degree of the violence sustained is sufficiently serve, the
condylar and may be driven through the roof of the glenoid surface into the middle fossa of
the skull. Fortunately, this does not happen often, since the neck of the condyle which is very
slender, fractures and prevents further damage. Hence it can be called as safely mechanism.
Regarding the treatment of the condylar fracture opinion is divided, some authors advocate
open reduction while others advocate conservative treatment. Also, they differ on the length
of time, the joint should be immobilized. But all authors agree that the treatment must include
restoration of functional occlusion of the teeth, acceptable appearance of the face, and normal
working of the jaws. They achieve these objective, certain basic orthopaedic principles
should be followed. This includes adequate immobilization of the fragments in proper
positioning for sufficient time to allow the fracture to heal.
Whatever method may be used in the treatment of condylar fractures, the surgeon must air at
achieving the best result. It must be properly treated, the complication, like arthritis,
asymmetry, clicking, limitation of jaw movement, open bite and ankylosis and myo-facial
pain dysfunction syndrome may supervene. Utmost care must be taken while treating
children to avoid injury to the condylar growth. If the growth centre is affected, it will cause

4
disfigurement of the face and malocclusion and can lead to emotional disturbance in the child
as age advances. Timely treatment is of utmost importance.
Click herewww.faceart-clinic.com

5
SURGICAL ANATOMY OF TEMPOROMANDIBULAR JOINT

6
The mandible is the largest, strongest, single, horseshoe shaped bone of the facial skeleton, it
houses the mandibular teeth. The body of the mandible lies horizontal with its convex portion
facing anteriorly. Attached to the curve body of the mandible are two broad rami, which
project upwards and have two processes, the coronoid and condylar process.
The TMJ is ginglymoarthrodial joint that allows the mandibular condyle to move freely in
both rotation and translation, with respect to the glenoid fossa. The joint contain superior and
inferior joint spaces separated by the meniscus. The articular surfaces of the condylar head
and glenoid fossa are covered by dense fibrocartilage. A synovial lining is found within both
the upper and the lower joint cavities. Synovial villi is present anterior and posterior to the
meniscus extending from the disk to the temporal bone superiorly and the condylar head
inferiorly.
The meniscus is a biconcave disk consisting of dense, fibrous tissue. It is situated within the
joint space and separates that area in superior and inferior joint space, thereby allowing
translation and rotation, respectively. The central portion of the disk is avascular and
relatively thin. Anteriorly the disk thickens and attaches superiorly to the articular eminence
and superior belly of the lateral pterygoid muscle. Inferiorly the anterior aspect of the disk
attaches to the condylar neck just superior to the insertion of the inferior belly of the lateral
pterygoid muscle. This area is highly vascular, with the auriculotemporal, masseteric, and
deep temporal vessels supplying the lateral pterygoid muscle and joint. Posteriorly the disk
attaches via the bilaminar zone, which is composed of two layers of fibrous tissue with
intervening loose areolar tissue. This area too is highly vascular and richly innervated. The
superior layer of fibers attaches to the tympanic plate of the temporal bone, and the inferior
layer runs from the posterior aspect of the disk to the posterior condylar neck. Medially and
laterally the disk is tightly attached to the medial and lateral poles of the condylar head,
allowing the disk to move with the condylar head during translation. This relationship
becomes displaced medially, carrying the disk with it.
The entire joint is surrounded by a fibrous capsule. It attaches superiorly at the margins of the
glenoid fossa and inferiorly at the condylar neck. The capsule is thickened laterally, forming
the temporomandibular ligament. This increased thickness resists lateral displacement of a
fractured condylar segment from the glenoid fossa. Medially the capsule is relatively thin,
making displacement in medial direction much more likely. Two additional ligaments serve
to support the TMJ, the sphenomandibular and stylomandibular ligaments.

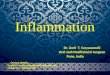
7
Anatomy of the Temporomandibular joint.

8
The sphenomandibular ligament inserts superiorly on the spine of the sphenoid bone and
courses inferolaterally to insert in the medial aspect of the ramus at the lingual. The
stylomandibular ligament passes from the styloid process to the angle of the mandible. These
ligaments act in a manner similar to collateral ligaments in other joints: the contralateral TMJ
ligaments acting like medial collateral ligaments aiding in the prevention of lateral
dislocation of the joint. Overlying the joint, capsule, laterally is the parotidomasseteric fascia,
which is tightly adherent to the inferior aspect of the zygomatic arch. The superficial
investing fascia lies superficial to this. Within the superficial fascia lie the temporal and
zygomatic branches of the facial nerve.
The TMJ lies in a region rich in neural and vascular structures. For two reasons, it is
important to understand the relationship of the structures to the joint. Second, overzealous
ligation of vessels and stripping of the fracture segments lead to unnecessary compromise of
the vascular supply to the condyle and other joint structures. Avascular necrosis of the
condyle is an uncommon but serious complication of fracture treatment.
Special care must be exercised to prevent damaging the neural structures surrounding the
TMJ, particularly the branches of the facial nerve. Sensory deficits, although annoying to the
patients, are usually tolerable, whereas facial paresis may result in devastating cosmetic,
functional, and psychologic consequences.
The primary blood supply to the mandibular condyle derives from branches of the superficial
temporal artery, the transverse facial artery, the posterior tympanic artery, and the posterior
deep temporal artery. The superficial temporal artery is one of the terminal branches of the
external carotid artery that runs deep to the paroid gland, emerging behind the neck of the
condyle. From there, it crosses the root of the zygomatic process of the temporal bone to
ascend to the temporal region of the scalp. The transverse facial artery departs from the
superficial temporal artery at its base and travels across the face on the superficial aspect of
the masseter muscle approximately 1.5 cm inferior to the zygomatic arch. The posterior deep
temporal and posterior tympanic arteries are branches of the maxillary artery that leave this
vessel to enter the anterior and medial aspects of the joint, respectively. Variable degrees of
damage to these vessels are inevitable, secondary to the nature of the injury, but as mentioned
earlier, additional damage should be prevented or, at least, minimized when the surgeon
approaches the condyle.

9
Arterial supply of Temporomandibular joint
Relation of the facial nerve with the condyle

10
The neural structures of primary import are the sensory auriculotemporal nerve and the motor
branches of facial nerve. The auriculotemporal nerve, a branch of the trigeminal nerve, passes
posterior to the neck of the condyle and crosses the zygomatic arch to ascend to the scalp just
anterior to the ear and posterior to the superficial temporal artery. This nerve supplies sensory
fibers to the posterior aspect of the TMJ.
The surgeon must be mindful of the facial nerve’s intimate involvement with the TMJ,
especially when performing surgical approaches to the joint. The temporal and zygomatic
branches are at increased risk during the preauricular approach, as is the marginal mandibular
branch during the submandibular approach. The intraoral approach to the joint has minimal
risk to the branches of the facial nerve as one of its major advantages.
In 1979 Al-Kayat and Bramley studied anatomic dissection of 56 cadaveric facial halves with
the intent of identifying the branches of the facial nerve and determining the distances
between these branches and readily identifiable landmarks of external auditory canal and the
postglenoid tubercle .Their aim was to determine areas of increased risk during surgical
dissection in the region of the TMJ. They found that the temporofacial division and the most
posterior significant twig of the temporal branch lie within a zone 0.8 to 3.5 cm (average 2.0
cm) anterior to the greatest anterior concavity of the external auditory canal. They also
reported that the point of division of the main trunk into temporofacial and cervicofacial
branches lies within a zone 1.5 to 2.8 cm (average 2.3) below the lowest concavity of the
external auditory canal and within 2.4 to 3.5 cm (average 3.0 cm) inferoposteriorly to the
postglenoid tubercle.
In 1962 Dingman and Grabb, in a similar manner, studied 100 cadaveric facial halves with
the aim of determining the course of the marginal mandibular branch of the facial nerve.
They found that posterior to the facial artery, the marginal mandibular branch of the facial
nerve was observed to run above the inferior border of the mandible in 81% of cases. In the
remaining 19%, the nerve coursed in the arc with the lowest point being within 1 cm of the
inferior border. Anterior to the artery, the nerve ran above the inferior border in 100% of
cases. They also observed that contrary to the majority of anatomy texts, the marginal
mandibular branch of the facial nerve is composed of several branches in the majority of
cases. In only 21%of cases was a solitary branches in 9%, and four branches in 3% of cases
studied. These measurements should serve as useful guides for the surgeon performing
surgical dissection in the region of the TMJ.

11
Alkayat-Bramly study showing the relation of the facial nerve with the TMJ

12
INCIDENCE & ETIOLOGY
The incidence of fracture involving the mandibular condyle varies throughout the literature
and is influenced by factors such as age, geographic location, and socioeconomic level of the
study population. Early reports revealed an incidence as low as 8% of mandibular fractures,
with later reports claiming an incidence as high as 76%. In any event fracture involving the

13
condylar process are by no means uncommon and probably make up between one quarter and
one third of all mandibular fractures.
Injury to the condyle may be caused by a variety of mechanisms, which also vary according
to the characteristics of the group studied. In adults motor vehicle accidents account for the
majority of condylar fractures, and interpersonal violence, work-related incidents, sporting
accidents, and falls play important but lesser roles. In children falls and bicycle accidents also
contributing significantly. Different still are the elderly, in whom falls again constitute the
primary factor, followed by assault and automobile accidents. Other less obvious causes of
injury to the TMJ include orotracheal intubation, whiplash injury, childbirth, and weight
lifting.
Lindahl divided traumatic forces causing condylar injury into three categories. The first is
energy imparted on a static individual by a moving object. This type of injury is typified by a
blow to the face by a fist, a baseball bat, or another object. The second type of force is that of
a moving individual striking a static object, such as a child falling and striking the chin
against the pavement. This mechanism is also seen in the classically described “parade
ground fracture.” The third classification is energy developed by a combination of the first
two mechanisms. This type of force is typical of that generated during an automobile accident
in which the individual is moving forward and the instrument console is moving in the
opposite direction following impact. This type of force is usually the greatest and produces
the most severe injury patterns.
A belief exists that the presence or absence of the dentition and the status of the mandible
(i.e., open versus closed) at the moment of impact also influence the type and severity of
fracture. He correlated this finding with the relatively high incidences of condylar fractures in
automobile accidents, presumably because the mouth is open because of screaming or fear at
the time of impact.
In 1977 Lindahl, however, noted in his study that no correlation existed between the presence
of, or status of, the dentition and the type of fracture observed, stating that all fracture types
were seen regardless of the occlusion. Furthermore, he found no influence on the degree of
the fracture by the most distal occlusal contact.
In any event, the type of fracture produced following an injury depends in part on the age of
the patient and in part on the direction and magnitude of the force. Certain mechanism

14
however, consistently reproduce specific fracture pattern. Therefore knowledge of the
mechanisms of injury may yield clues to guide the clinician during the initial examination of
the patient. For example, a direct blow to the TMJ region may result in a fracture of that
condyle. But this fracture is fairly uncommon owing to the protection afforded to the condyle
by the lateral rim of the glenoid fossa. More commonly a blow directed horizontally to the
mandibular body, such as that provided by a fist, results in a fracture of the ipsilateral
mandibular body and also the contralateral condyle. A force applied to the parasymphyseal
region may cause an ipsilateral condylar fracture. When a force is directed axially to the chin
region, such as when the chin strikes the ground after a fall or dashboard during an
automobile accident, force is transmitted along the mandibular body to the condyles. This
typically results in a symphyseal or parasymphyseal fracture combined with unilateral or
bilateral fracture of the condyles. As the condyles are driven superiorly and posteriorly into
the glenoid fossa, there may be concomitant fracture of the glenoid fossa with penetration
into the middle cranial fossa, or fracture of the tympanic plate and damage to the external
auditory canal. In children bone has greater elasticity and therefore a blow to the chin may
result in bilateral “greenstick” fractures of the condyles. The mechanism of injury thus alerts
the clinician to heighten his or her degree of suspension and provides useful insight into the
type of injury to be expected.
Click herewww.faceart-clinic.com

15

16

17
SOFT TISSUE INJURIES
An extensive review of soft tissue injuries involving the TMJ is presented by Goldman. He reviewed a large number of studies related to TMJ dysfunction and found that trauma was a primary causative factor in the majority of instances. He described a division of trauma into two groups: macrotrauma and microtrauma. Macrotrauma includes bruxism or a direct blow to the jaw, whereas microtrauma includes less conspicuous injuries, such as nail biting, yawning, violin playing, scuba diving, and whiplash injury. Depending on the magnitude, direction, and duration of the insult, damage may include mild inflammatory changes, such as synovitis, capsulitis, and inflammation of the surrounding muscles and ligaments. Prolonged abnormal loading of the joint perpetuates the inflammatory process and leads to chondromalacia, internal derangements, alteration of disk and articular cartilage morphology, and eventually degenerative changes. The majority of soft tissue injuries to the TMJ may be successfully treated with conservative measures, such as jaw rest, soft diet, analgesic, and nonsteroidal anti-inflammatory agents. Additional measures including behaviour modification, psychotherapy, bite splints, and occlusal adjustment may also be of benefit in selected circumstances.

18
CLASSIFICATION

19
Fracture of the condylar process of the mandible presents a special problem which has to be treated with care.
In order to plan a treatment of the condylar fracture it is important to classify and group a particular type of fracture to facilitate proper study of the case before deciding on the method of reduction and fixation. The classification of the condylar fractures can be carried out taking some important landmarks into consideration or according to the displacement of the fractured part of the condyle.
Rowe and Killey (1968) taking into consideration the anatomy and clinical findings, classified the fractures in the following way:
A) ANATOMICAL CLASSIFICATIONB) CLINICAL CLASSIFICATION
ANATOMICAL CLASSIFICATION:
SIMPLE:
1) Intra capsular2) Extra capsular3) Fracture associated with injury to the capsule, ligament and meniscus.4) Fracture involving the adjacent bone e.g. roof of the glenoid fossa and tympanic plate.
COMPOUND:
Are those fractures which compounds to the external meatus, middle ear and to nasopharynx through the eustachian tube. Penetrating injury of the joint from a sharp weapon or a gunshot may also compound to the external environment or to oral cavity.
CLINICAL CLASSIFICATION
MacLennan System. In an attempt to establish a more clinically useful classification scheme, MacLennan in 1952 proposed a system based primarily on relationship of the proximal and distal fracture segments to each other. His system consists of four divisions as follows.
1. Type I fracture, non-displaced.

20
2. Type II fracture, fracture deviation. This type consists of a simple angulation of the fracture segments without overlap or separation. This type includes the greenstick fracture commonly seen in children.
3. Type III fracture, fracture displacement. This group of fractures is characterized by overlap of the proximal and distal fracture segments. The overlap may be anterior, posterior, lateral, or medial. However, as mentioned previously, medial displacement is seen most commonly because of the anteromedial pull of the lateral pterygoid muscle.
4. Type IV fracture, fracture dislocation. Here the condylar head is completely outside the glenoid fossa and therefore outside the capsular confines. Again the dislocation may be medial or lateral and rarely anterior or posterior.
Lindahl System. In 1977 Lindahl proposed a system that classified condylar fractures based on factors, including (1) anatomic location of the fracture, (2) the relationship of condylar segment to the mandibular segment, and (3) relationship of the condylar head to the glenoid fossa. His system necessitates that radiographs be obtained at-least two views at right angle to each other. The classification is as follows:
1. Level of condylar fracture
a) Condylar head. Although the exact anatomic confines are somewhat nebulous, the condylar head is usually defined as the portion of the condyle superior to the narrow constriction of the condylar neck. Grays anatomy defines the condylar head as extending a short distance down the anterior aspect of the process, covering the entirety of the superior portion, and extending at-least 5mm down the posterior aspect. Although different to define precisely radiographically, it is relatively easy to identify the constriction of the condylar neck. They may be further classified as vertical fractures, compression fractures, and comminuted fractures.
b) Condylar neck. The condylar neck is the thin constricted area located immediately below the condylar head. It is fairly easy to identify this area radiographically. The condylar neck anatomically is the region where the caudal portion of the joint capsule attaches. These fractures are therefore extracapsular,
c) Subcondylar. This region is located below the condylar neck and extends from the deepest point of the sigmoid notch anteriorly to the deepest point along the concave posterior aspect of the mandibular ramus. Depending on the location of the fracture, these fractures are sometimes described as “high” or “low” subcondylar fractures, perhaps to make reference to the more difficult surgical approach to the low subcondylar fracture.
2. Relationship of the condylar segment to the mandibular fragment
a) Non-displaced.

21
b) Deviated. This involves only an angulation of the condylar fragment in relation to the distal mandibular segment. The fractured ends remain in contact, with no separation or overlap.
c) Displacement with medial or lateral overlap. The fractured end of the proximal condylar segment lies either medial or lateral to the proximal end of the distal mandibular segment. Secondary to the pull of the lateral pterygoid muscle, the medially displaced condylar fragment is the more common variety.
d) Displacement with anterior or posterior overlap; these types are uncommon.e) No contact between the fracture segments.
3. Relationship between the condylar head and the glenoid fossa
a) Non-displaced. The condylar head is in normal relation to the glenoid fossa.b) Displacement. The condylar head remains within the fossa, but there is alteration in
the joint space.c) Dislocation, the condylar head lies completely outside the confines of the fossa. For
this displacement to occur, there must be rupture of the capsule. The lateral capsule is usually quite thick and strong, whereas the medial joint capsule is thin and weak. Therefore the usual location of a dislocation condylar segment, because of the lateral pterygoid pull, is anteromedial.
Richardson and Cohen (1953) classified the condylar fracture in the following manner:-
A) Fracture of the condylar head:1. Incomplete fracture with no displacement.2. Incomplete fracture with dislocation of a segment.3. Complete communited fracture with little displacement.4. Complete communited fracture with dislocation.
B) Fracture of the neck of the condyle:1. Green Stick fracture.2. Slight displacement with good alignment.3. Gross displacement with overriding of the fragments.4. Displacement with rotation of the condyle.5. Complete fracture with dislocation of the codylar head.
C) Subcondylar fractures:This fracture may be green stick, impacted, overriding or displaced.
D) Injury to the meniscus:It may be torn, ruptured or herniated in forward or backward position.Garry presented his own classification:a) Undisplaced condylar fractures.

22
b) Displaced condylar fracture, displacement may take place anteriorly, medially or inferiorly.
c) Condylar fracture dislocation. The dislocation may take place in any direction, but chiefly the condyle herniates through the joint capsule in anteromedial direction.

23
Lindahl’s classifications

24
Thoma (1945) classified fractures in a simple way, taking into consideration the direction of displacement.
A) Codylar fractures:1. Without displacement of condyle:
a) Green stick.b) Intracapsular.c) Extracapsular.
2. With displacement of condyle:a) Lateralb) Medialc) Forwardd) Backward
3. With overriding of fragments4. With dislocation in lateral or medial direction:
a) Intracapsular b) Complete fracture dislocation(40-90 degrees)c) Complete dislodgement of the condyled) Dislocation of the fractured part of the head of the condyle.
5. With dislocation in a forward directions:a) Anteriorly from the articular eminence.b) Posteriorly from the articular eminence.
6. With dislocation and displacement of the meniscus7. With comminution8. Old fracture with deformities:
a) Pseudoarthrosisb) Ankylosis
B) Sub-condylar fracture:i) Without displacement of the fragmentii) With displacement of the fragment
Fracture line either extending through head or base of the condyle or neck has been called condylar fracture by Thoma, whereas in sub-condylar fracture, the line runs transversely over ascending ramus.
Roentgenographic studies were considered for classification of condylar fractures by Blevins and Groves (1961). They believed that incorrect plane of roentgen may mislead the diagnosis.

25
They classified the condylar fractures as follows:
CLASS I:- Medial displacement.
a) Anterior positionb) Posterior position
CLASS II:- Lateral displacement
a) Anterior positionb) Posterior position
CLASS III:- Medial override
a) Anterior positionb) Posterior position
CLASS IV:- lateral override
a) Anterior positionb) Posterior position
CLASS V:- Green Stick fracture.
Many other workers like Berger (1924), Blair and Ivy (1936), Walker (1942) have also classified condylar fractures in different ways.
ARCHERS CLASSIFICATION OF FRACTURES
Single fractures: Bone is fractured only in one place, usually unilateral. Rarely seen in mandibular fracture, when seen it may pass through the neck of the condyle.
Multiple fractures: Bone is fractured in two or more places. Bilateral are more than other types of fractures occurring in mandible and maxilla.
If the fracture occurs through the neck of the condyle on one side, there is usually a fracture through the mental foramen on the contralateral side. If it occurs through the mental foramen on one side, it may occur through the angle formed by the ramus and body on the other side, or through the neck of the condyle. Multiple fractures may also be unilateral, the bone being fractured into several segments on side only.
Simple fractures: More commonly found as fracture of the ramus of the mandible or at the angle formed by the ramus and the body of the mandible. In these type of fractures, the fractured bone is not in contact with the secretions of the oral cavity and the fractured bone

26
does not communicate with the external surface os the face through a laceration in the investing soft tissues.
Compound fractures: Where the fractured parts of the bone communicates with the oral cavity or external surface of the face through a laceration in the oral mucosa or in the skin. The fractures generally occur anterior to the angle.
Communicated fractures: In this type of fractures, either the bone is shattered or broken up into pieces of fragments.
Complicated fractures: In this type of fracture both maxilla and mandible are involved or in which the maxilla or the mandible is edentulous. There might be marked displacement of the compound communited osseous fragments of either or both the maxilla and mandible, with extensive trauma of the investing and covering soft tissues. There may be an associated fracture of the skull.

27
CLINICAL EXAMINATION
As with examination of any other area or system, clinical examination of the patient
suspected of having a fracture of the mandibular condyle should proceed in a systematic and
orderly manner. An overall examination of the patient with traumatic injury should precede
evaluation of the maxillofacial region. After the patient’s condition has been deemed stable,
and other more serious injuries have been addressed, attention can be directed to the
suspected maxillofacial fracture.

28
The patient with fracture of the mandibular condyle usually has a suggestive history and,
in addition, one or more of the following findings:
1) GENERAL EXAMINATION
AT ARRIVAL: Gain information quickly from the patient, or accompanying person
regarding mechanism of injury, any obvious deformities signs of injury or illness.
PRIMARY SURVEY:
Assessment of patency of airway(breathing)circulation, or any active profuse bleeding
or history of excessive blood loss.
SECONDARY SURVEY:
Vital signs:-
- Radical pulse rate and character should be determined.
- Respiratory rate and character of respiratory should be noted.
- Blood pressure should be measured by auscultation and palpation.
HEAD TO TOE SURVEY:
- Check scalp for cuts, bruises, swelling and other signs of injury. Examine skull for
deformities, depressions and signs of injury including facial bones, eyelids and
orbit.
- Determine pupil size, their equality and reactivity.
- Look for blood, clear fluid, or blood contamination fluid from the ears and nose.
- Examine mouth for obstruction.
- Examine the patient for any injuries to the neck, chest or abdomen and upper and
lower extremities.
It is always better to explain and warn the patient when there is a possibility of pain
during examination at all times go gain the patient’s co-operation.

29
2)LOCAL EXAMINATION:
SIGNS AND SYSTOMS:
1. Evidence of trauma, which may include facial contusions, abrasions, laceration of the
chin, and ecchymosis and/or hematoma in the TMJ region .these injuries should alert
the clinician not only to possible fractures in the area of direct injury but also to
indirect injury to the ipsilateral and the contralateral TMJ.
2. Bleeding from the external auditory canal. This finding may indicate fracture of the
anterior tympanic plate from a posteriorly displaced condyle.
3. A noticeable or palpable swelling over the TMJ may be
4. a laterally dislocated condylar head that is directly visible under the skin.
5. Facial asymmetry may be the result of soft tissue edema or may be a result of
foreshortening of the ramus caused by overlap of the proximal and distal fracture
segments.
6. Pain and tenderness to palpation over the affected TMJ. There may also be notable
pain on attempted manipulation of the jaw by the patient or the clinician.
7. Crepitation over the affected joint secondary to friction of the irregular fracture ends
sliding over one another during manipulation.
8. Malocclusion may be a useful clue to the type of injury sustained. A unilateral
condylar fracture usually results in ipsilateral premature contact of the posterior
dentition secondary to foreshortening of the ramus on the side. This foreshortening
may also result in a contralateral posterior open bite because of the canting of the
mandible. Bilateral condylar fractures may result in a marked anterior open bite and
retrognathia. The medial pterygoid and masseter muscles exert a superior and
posterior pull on the distal mandiblular segment, causing it to telescope past the
condylar segments. This telescoping results in premature contact in the posterior
occlusion with rotation of the mandible around this point and anterior open bite.
Gagging on the posterior teeth may also occasionally be seen because of the
posteriorly positioned mandibular segment.
9. Deviation of the mandible midline may be seen both at rest and with attempted
excursion of the mandible. At rest, because of shortening of the ipsilateral ramus , the

30
mandible may deviate toward the fractured side. In a unilateral fracture, with
attempted opening of the mouth, the lateral pterygoid on the fracture side is unable to
effect pull on the mandible, and the unaffected contralateral muscle function normally.
This inequality of function causes an exaggeration of the deviation toward the
fractured side. Similar deviation is seen with protrusive movements. Attempts to move
the mandible laterally away from the fractured side are met with great difficulty
because of the ineffective lateral pterygoid muscle. Bilateral condylar fractures may
result in little deviation of the midline because both condyles are involved. As,
mentioned, an anterior open bite will be seen with retrognathia in addition to severely
limited range of motion.
10. Muscle spasm(“splinting”)with associated pain and limited opening.
11. Dentoalveolar injuries.
Any one or combination of these findings should raise the clinician’s index of
suspicion as to the possibility of unilateral or bilateral condylar fractures in addition to
other maxillofacial injuries.
INSPECTION
Inspection of fracture site may reveal oedema, ecchymosis and deformity in the region of
fracture. Soft tissue injuries in the joint region should be examined for perforation in the joint
region. The presence of blood in the external auditory canal may indicate perforation injury
of the joint, presence of cerebrospinal fluid may give to suspicious involvement of middle
cranial fossa
The facial asymmetry, or any obvious bulge or depression in the preauricular area may
indicate the displacement of a fragment or a fracture dislocation. A shift in the midline of the
teeth may be apparent, or a lateral displacement of chin in the edentulous patient with
unilateral condylar fracture may be observed.
Abnormal movements of the jaw can occur during opening and closing movements of the
jaw.
An intraoral inspection within a few hours of injury will reveal the presence of blood
stained saliva. The buccal and lingual sulci is examined to note any breach in continuity of
mucosa and the existence of ecchymosis or sublingual haematoma. The alignment and the

31
occlussal plane should be noted for the presence of any step deformity, suggestive of a
fracture of the underlying bone.
PALPATION:
Palpation should be started from the temporomandibular joint region and should proceed
along the entire length of the mandibular posterior and inferior border noting any tenderness
or breach in the continuity.
By means of palpation we can determine the pain due to pressure at the joint or the
protrusion of the displaced or dislocated fragment. Crepitations may be noted during jaw
movements due to rubbing of the fracture ends together.
In all cases of suspected condylar fractures it is helpful to place the little finger into the
external auditory meatus, in order to detect any movement or lack of movement of the
condylar head, when the mandible is moved.
The buccal and the lingual sulcus should be palpated intraorally, for presence of any
tenderness and alterations in the contour, the mandible should then be grasped on either side
of the suspected fracture and a gentle attempt should be made to elicit any abnormal mobility.
Clinically it will be noted that there is asymmetry of the face on the involved side due to,
shifting of the mandible posteriorly and laterally towards the affected side. Premature
occlusion on the involved side is caused by upward pull of the elevator muscle of the
mandible. This result in a class I lever with the fulcrum on the molar teeth on the involved
side. An open bite deformity anteriorly on the opposite side of the mandible is noted.
Tenderness on palpation over the TMJ and in the external auditory canal is a common
finding. Moderate to severe oedema, ecchymosis and occasionally haemorrhage may be
noted in the external auditory canal. If both the mandibular condyles are fractured the patient
will have an anterior open bite deformity with occlusion only on the posterior teeth.
Anterior open bite deformity is caused by upward displacement of ramus and telescoping
of the fractured segments, due to contractions of the strong elevator muscles of the mandible.
In bilateral condylar fractures which occur below the attachment of the lateral pterygoid
muscles, the patient is unable to protrude the mandible. In unilateral fractures at the same
level, the patient is unable to form lateral motions to the opposite side. Lateral movements of
the mandible can be made only towards the affected side, because the lateral pterygoid

32
muscle on the unaffected side shifts the mandible medially and forward, while the muscle is
completely out of function on the affected side.
The patient usually will have dysfunction and pain on attempting the opening movement
of the jaw. If the posterior fragment have been displaced posteriorly, the mandible may shift
forward as the segment of the ramus distal to the fracture rides upward and glides forward on
contact with the condyle fragment. This may produce an open bite with protrusive
relationship of the mandible.
Fractures above the level of the lateral pterygoid muscle insertion do not exhibit
displacement, because of the absence of contracting muscle attached to the proximal segment.
The patient may complain of severe pain in the TMJ, and it will be noted that the teeth are
shifted and do not come into occlusion on the affected side because of the haemorrhage and
oedema in the joint which forces the condyle downwards. It may be several weeks before the
teeth come into their normal occlusal relationship. In this type of fractures, especially in
children the parents should be warned about the possibility of the development of ankylosis,
if proper treatment is not initiated. In some cases, even though ankylosis does not occur the
head of the condyle may be damaged, thus affecting the growth, with subsequent mal-
development.

33
RADIOLOGICAL EXAMINATION
When a patient has a history of trauma and a clinical examination suggestive of condylar
fracture, a radiographic evaluation is mandatory. Maxillofacial radiographic technique
mandates that at least two radiographs be obtained at right angle to each other to adequately
evaluate the TMJ region. In most centres the mandible series consists of a posteroanterior
skull view, two lateral oblique, and a Towne’s view to evaluate the mandible. If available a
panoramic radiograph may added to this series. Interestingly, Charya et al compared the
sensitivity of the “standard” mandibular series with the panoramic radiograph in detecting
mandibular fracture. They found that the panoramic film had a higher accuracy in detecting
all types of mandibular fracture (92% versus 66%) except those in ramus region, where two
studies are of equal value. They cite a decreased cost and low radiation exposure as

34
advantage of the panoramic film compared with the mandible series. The panoramic
radiograph, however, necessitates that the patient be able to stand erect and immobile for an
adequate period of time. Problems with the mandibular series include the increased radiation
exposure, increased cost, and decreased detail secondary to superimposition of other
maxillofacial bony structures. In midfacial injury, however, the panoramic film is of little
value, and the maxillofacial series becomes necessary.
With the advent of newer imaging techniques,(i.e., computed tomography “CT” and
magnetic resonance imaging “MRI”, the standard radiographic survey has largely been
supplanted in the diagnosis of maxillofacial trauma. Computed tomography scans yield
excellent bony detail of the facial skeleton in multiple views and, with adjustment of the
contrast of the machine, give adequate soft tissue detail. An additional advantage is less
dependence on patient cooperation, which is useful in the severely injured or uncooperative
patient. The disadvantages of CT include radiation exposure, the notably higher cost, and the
limited availability in some centers.
Magnetic resonance imaging yields excellent soft detail but less bony resolution compared
with CT. It may be useful as an adjunctive study, if notable soft tissue injury of the joint is
suspected. It has the additional advantages of no ionizing radiation exposure and the ability to
obtain images in any desired plane of view by reconstructing the imaging data. Disadvantage
include the notably higher cost compared with standard plain films and CT and the increased
time required individual images.
In summary in the acutely injured patient, the standard mandibular series suffices as a
screening survey. If further diagnostic information is required, such as in dislocation condylar
fractures, suspected intracranial penetration, notable soft tissue injury, and midfacial trauma,
additional studies including CT and MRI may be indicated.
Following are the type of radiographs that are helpful in diagnosis of condylar fracture.
I) POSTERO - ANTERIOR PROJECTIONS FOR MANDIBULAR
RADIOGRAPHY:
a) POSTERO-ANTERIOR VIEW OF THE MANDIBLE:

35
This view has been long remained the standard type for the mandible, the entire
outline of the mandible is visible in this view. With standard P.A. view it is not
possible to define the condylar head the glenoid fossa because of superior position
of the zygomatic bone and the mastoid shadow, hence only fractures of the
sudcondylar region are seen in this view. For this purpose a modification has been
suggested. In standard P.A. projection the ‘X’ Ray beam passes parallel to the
orbitomeatal plans which is oriented parallel to the horizontal plane, whereas the
modified view the beam passes at 10 degrees to the horizontal plane.
The P.A. view only shows the extent of lateral or medial displacement of the
fractured condyle.
b) THE REVERSE TOWNE’S PROJECTIONS:
This view gives a clear idea of medial or lateral displacement of the condyle and
its relation to the ramus of the mandible. Also the fractures of the condyle neck
are appreciated in this view.
The Reverse Towne’s projection is obtained with the orbitomeatal plane oriented
at 25 to 30 degrees towards the horizontal. The ‘X’ Ray beam is passes from
behind, through the occipital protuberance.
c) ORTHOPANTOMOGRAPHY:
In recent years OPG is fast replacing over views as a standard projection. It
provides the best visualisation of the entire mandible. Its added advantage over
other P.A. views is that the condyle and the glenoid fossa are well defined. It gives
an idea of the extent of anterior displacement of the fractured condyle. Fractures
of the condylar head are seen well in the OPG.
Horwitz et al suggested the use of Computerised Tomography to determine the
exact location of the fracture line in condylar fracture. They claim that a coronal
computerised tomographic view defines the head, neck as well as subcondylar
regions extremely as well as, the relation of the fractured condyle to the ramus.
II) THE ANTERO-POSTERIOR PROJECTIONS:
a) TRANS ORBITAL VIEW:

36
This determines an excellent localised view of the condylar neck and the
subcondylar region. The condylar head may be obscured, however, with this view
it is difficult to judge the relation of the condylar fragment to the ramus .
The ‘X’ Ray film is placed behind the patients head and the ‘X’ Ray beam
passes from the orbit on the same side at 10 degrees to the sagittal plane to the
film.
b) TOWNE’S VIEW:
It is also known as 30 degree fronto-occipital projections. The patient seats with
his back to the film. The orbitomeatal plane is oriented parallel to the floor the
beam passes at 30 degrees towards the floor from above the nasion. If the patient
opens his mouth the condylar head outline can be traced.
III) LATERAL PROJECTIONS
a) THE LATERAL OBLIQUE VIEW:
The outline of the mandible may be visualised from the first premolar to the
condyle, it is advisable to specify the area of fracture to the radiologist. If taken
meticulously, may provide a good view of the condylar neck subcondylar area and
the relations of the condyle to the antero-posterior direction. Overlapping of the
condyle by the shadows of the cervical vertebrae and radiolucency of the
pharyngeal air spaces is disadvantages.
b) TRANSCRANIAL VIEW:
Provides an excellent view of the intracapsular fractures of the condylar head
if any and the relation of the condylar head to the glenoid fossa.
The diagnosis of fracture of the condyle is usually made on clinical examination
and confirmed by roentgenographic findings.

37

38

39
PHYSIOLOGICAL & HISTOLOGICAL
CONSIDERATION OF FRACTURE HEALING
The two remarkable properties that distinguish the bone tissue from other structural tissues
are:
- The property of altering its local mechanical characteristics is response to changes
in functional demand.
- The capacity to heal itself through a repair process that results in no scar
formation, a capacity to heal itself through actual regeneration.

40
A fracture disrupts the continuity of a bone, disturbing its mechanical as well as the
biological function. Starting from this initial state, fracture healing is intended to restore the
original structure, and thus the function.
The pattern of healing is governed, to a fair extended, by the amount of motion in the
fracture gap. An essential prerequisite for a rapid and undisturbed healing process is a well
functioning blood supply in the fracture region.
Mechanical conditions immediately after fracture are as follows:
- The fragment and mobility is only limited by soft tissue envelope. The muscles in
the fracture region are contracted, possibly are reflex reaction. These muscle
contractions cause an initial, though incomplete, attempt to immobilize the injured
area. In addition, the sensation of pain prevents large scale active movements.
- The initial biological situation is characterised in the first instance by disturbed
circulation. Soft tissue injuries are partially detached from bone cortex, are
interrupted at the fragment ends, and are closed by blood clotting. During the first
hours after trauma, the area of closed vessels increases in size. Border zones at the
fragment ends are thus left without blood supply. The pattern of non-perfused
regions depends on the possibility of anastomoses to occur in the bone. It may
happen that entire fragments, or fragment ends with sharp points, have no
circulation. A more or less extensive hematoma will be produced between the
fragment ends by the bleeding from interrupted vessels.
- Bone heals by primary or secondary intention
BONE HEALING BY PRIMARY INTENTION:
This occurs when the fractures bones are in excellent anatomic position and the fractured
fragments are rigidly fixed, thereby preventing the interfragmentary movement due to muscle
activity.
Primary bone healing occurs in two different ways:

41
a) Contact healing
b) Gap healing
a)Contact healing:
The contact healing takes place by haversian remodelling or intracortical remodelling. It
is the mechanism the replaces compact cortical bone step by step, by new bone of the same
structure. In this process, a group of osteoclasts “drills” a tunnel with a diameter of about
0.2mm in the longitudinal axis of the bone. These osteoclasts are followed by vessels and
mesenchymal cells, and somewhat farther back by a front of osteoblasts. These osteoblasts
are arranged in a funnel shaped. In longitudinal section their arrangement appears V-shaped
and in cross-sections, round. New osteoid is deposited in this canal, which then matures into
lamellar bone. The process of haversian remodelling can take place directly through the
fracture zone if the fragment ends are in close and stable contact. This type of healing occurs
in fractures treated with compression osteosynthesis as claimed by the ASIF School. The
fractured bone is thus replaced by the new lamellar bone, which in its structure corresponds
to a certain extent of the original bone. However, Hutzencheuter et al have shown that even
through compression osteosynthesis was used, a very small gap (0.01 osteons) allowed
intolerable interfragmentary strain to develop, resulting in resorption of the bone ends. This
resorption results in a gap in which interfragmentary strain is dissipated and in which healing
occurs. Luhr et al mentioned that dissipation of interfragmentary strain is not due to
resorption of bone ends, but, due to mechanical deformation of the bone at the fracture site.
b)Gap healing:
Healing of fractures takes place when rigid fixation is used and very small defects of 3 to 4
osteons exists. A fracture scarcely can be realigned in such a way that contact is produced
everywhere. When the plate is applied the interfragmentary compression is not always
homogenously distributed, thus minute gaps may be maintained. Lamellar bone starts
depositing into these gaps, and is comparable to the filling of bone defects. By means of
haversian remodelling, such filled defects are then restructured to result into osteons arranged
in the longitudinal axis of the bone. Callus formation is not seen.
BONE HEALING BY SECONDARY INTENTION:
Initially the mobility of the fragment ends is still too extreme to permit calcification in the
interfragmentary spaces. The continuous motion even results in resorption of the fragments

42
ends, which becomes rounded. Initially, the interfragmentary region is filled by a hematoma.
This is gradually replaced by granulation tissue, which further differentiates into connective
tissue and, in the region between the fragments, into fibrocartilage. The whole shape of the
callus cuff is thus performed soft tissue. At a distance from the fracture, this callus slowly
begins its transformation into fibrous bone, also designated as desmal ossification. The
formation of connective tissue and fibrocartilage already begins about a decrease in the
mobility of the fragments, which allows mineralization of the callus. This is to increase in the
cross section of the bone, and thus to a longer lever arm to counteract the displacing forces.
Thus the demands for the strength of the repair tissues may be reduced. The interfragmentary
fibrocartilage contributes to a damping of motion. The cartilaginous component acts as a kind
of hydraulic pressure pad, such that the fibers absorb tensile forces. The resulting inhibition
of movement permits calcification process in the interfragmentary region as well. The
intercellular substance of the cartilage gradually incorporates mineral and can be replaced by
bone, designated as ‘chondral ossification’. The narrowing of the interfragmentary space
causes a further reduction of the mobility until final bony bridging has occurred. Osteoclastic
resorption balanced with osteoblastic bone formation then gradually changes the cancellous
callus structure back into a cortical tubular bone. As the new cortices become more compact,
the cross-section of the bone is reduced to normal dimensions and a new medullary cavity is
formed.
The great majority of fractures are allowed to heal by secondary intention. The jaws are
immobilized by wiring the teeth together. Even it transosseous wiring is done, a semirigid
fixation is at best achieved, some interfragmentary movement occurs with muscle activity
even though the jaw is rendered non-functional.
Function in the fractured part also plays an important role in the healing process. Sample
evidence shows that a functional limb heals faster and better than the immobilized limb.
Rigid internal fixation when used, drastically the healing period restores early function
to the joint. Ideal conditions for the healing of fractured bones involve rigid fixation and
compression of the fragment without immobilization of the injured part.

43

44
STABLE OSTEOSYNTHESIS THEORETICAL &
TECHNICAL CONSIDERATION
BIOMECHANICAL FUNDAMENTALS:
During the past decade the operative treatment of the mandibular fractures has been
influenced and modified by a variety of experimental studies. In the search for a simple
osteosynthesis, that would guarantee fracture healing without intermaxillary fixation and

45
without compression, the monocorticle plate osteosynthesis of Michelet et al (1973) was
modified and developed into a practical method.
The biomechanical principles of this method are based on the mathematical and
experimental studies carried out in strausbourg at Ecole National Supereieure Des Arts et
Industries. The research goal was to develop a true tension banding system for the mandible
along an ideal osteosynthesis line and an osteosynthesis material with favourable mechanical
properties.
ANATOMICAL AND BIOMECHANICS OF THE MANDIBLE:
The parabola shaped body of the mandible consists of outer and inner cortical layers
with a simple spongiosa. The outer cortex is particularly strong. The trajectories of the
mandible shows that the mandible is strengthened in response to the forces of the muscles of
mastication by development of massive compact, as well as by trajectories of the spongiosa.
The masticatory forces are led up towards the condyle of the crest of the mandibular neck,
which is prominent on the inner side of the ramus and runs from the end of the alveolar
process diagonally towards the head of the mandible.
On an average the outer cortex is 5mm thick in subcondylar fractures the main forces
acting on the condylar fragment is the lateral pterygoid muscle, which is responsible for the
displacement. The outer cortex provides osteosynthesis screws with good anchorage by virtue
of its compact structure. The same principle can be utilized to achieve stable osteosynthesis
in case of subcondylar fracture using a 3 or 4 hole bone plate with monocortical screws
engaging the outer cortex. As soon as the fractured fragments are stabilised by using
monocortical miniplate system the distraction at the fractured site is prevented. It is possible
to place this miniplates in the centre of the condylar region on the lateral aspect, so that the
fracture is stabilised well without any distraction of fragments on the medial or lateral
aspects, due to the tortional forces (this eliminates the need of any additional tension banding
as described for the body of the mandible).
TECHNICAL ASPECTS OF FRACTURED FIXATION:
The screws, plates and instruments should be of the same material, since variation in metal
ions can lead to an oxidation – reduction phenomenon with detrimental tissue effects.

46
The following points must be observed strictly during plate fixation:
1) Drilling must be precise and must be monoaxial, otherwise, an unfavourable cortical
bur hole results.
2) The screws must be self tapping, the drill must be of the width of the screw core.
3) The screw thread must be relatively narrow so that considerable contact is made
between the thread and the bone. The distance between the turns of the thread is more
than 1mm.
CONSIDERATION IN IMPLANT DESIGN
Compression of the fragment ends is an important mechanism for stabilization in bones that
are functionally loaded with high mechanical forces. Specially designed screw holes in the
plate facilitate compression.
In screw design, various engineering and biomechanical aspects come into consideration.
For technical applications in thin sheets, the screw thread gets its grip on outer surface of the
material. In thick layers, the thread design may take different strengths of the materials into
consideration and allow a larger volume for the weaker material. This design characteristic
with asymmetric threads is widely used in screws for bone fixation, and it makes a good
compromise in both thin and thick bones.
Besides the screw design, the mechanical properties of the bone structure determine the
initial holding force. The approximate force may be estimated from the radiological bone
density.
The plate dimension is to be adapted to their planned field of use, where they should
provide sufficient stability. The bone plates used are 1mm thick a width of 6mm. The screw
holes are neutral with a diameter of 2.6mm and a bevel of 30 degrees. The counter sinking of
the screw hole ensures a snug fit between screw and plate causing compression between the
plate and bone, thus increases its stability. The comparatively high elasticity of the material
tolerates easy deformation in all 3 planes so that exact adaptation to the bony surface is
possible.
COMPARISION OF METALS FOR THE PLATE
Selection of an implant material for craniomaxillofacial use involves two important
considerations.

47
a) Whether physical properties of the implant material allows its adaptation and the
application for functional load.
b) Whether biocompatibility of the material, in its loaded or unloaded clinical
adaptation, will be tolerated by the host tissues.
In assessing the performance of a permanent implant, the effect of the body tissues on
functional properties of the implant i.e. ‘biofunctionally’ and the cellular effect on near and
distant tissue i.e. ‘biocompatibility’ must be examined simultaneously.
After implantation of a solid alloplast during normal would healing, fibrous encapsulation
will depend upon the mechanical, chemical and physical chemistry of the implant interface as
well as the stability of the implant at the site during functional loading. These range from
inertness to reactivity in the chemical sense, from stiffness to softness in the mechanical
sense and from solid to porous in regard to physical properties.
The desirable properties of an implantable alloy include primarily corrosion resistance,
malleability and strength. The use of metal is not an absolute requirement in the jaws, since
the mechanical demands could be met by other materials as well. But the ductility of the
metals (as opposed to polymers and composites) is a feature that allows for intra-operative
contouring of the implant according to the clinical need.
The design, processing and handling of metallic implants significantly influence the in
vivo corrosion and stress corrosion behaviour. Metallurgical analysis had shown that fatigue
seems to be major cause of failure of an implant. Fatigue occurs when corrosion weakens an
area of the implant that is subject to functional stress. Defects which lower the corrosion
resistance include high inclusion content, cracks due to cold rolling, pitting of the surface,
poorly sunk holes and molybdenum content below 2% as ASTM specification.
When a alloy has a low corrosion rate in an oxidizing environment, it is said to be
passive. This state is due to the formation of a surface film, which can be explained on the
basis of oxide film theory or adsorption theory of passivity.
The metals commonly used for fixation of maxillofacial fractures include stainless steel
(Champy, AO), Cobalt alloys (Luhr) and titanium (Wurtzberg. Steinhauser ).
Vitallium: It was first used in orthopaedic surgery in 1932 by Venables but its reference in
jaw surgery was made by Winter in 1945.

48
A Cobalt-Chromium alloy has two to three times more tensile strength, 50% greater yield
strength and twice the hardness of titanium or steel Vitallium has remarkable resistance to
corrosion as well as excellent stability properties. Vitallium is also a better metal for screws
than titanium having a higher torque strength. When metal is bent, there is an increase in its
tensile strength and hardness and this is similar for all three metals. However, there is an
increase in yield strength which is slight for titanium but 50% for steel and doubling for
Vitallium. Therefore smaller plates can be made without a compromise in strength.
Titanium: First discovered in 1971, it was in 1930s that its ductility and usefulness as an
implant was realised.
Alloying of titanium to vanadium and aluminium increases its strength. The weight of
titanium is 60% that of steel, is readily machined and manufactured into a variety of shapes
and forms.
Titanium is highly flexible as the modulus of elasticity is half that of stainless steel or
Vitallium. It has excellent ductility and tensile strength fatigue limit equal or greater than that
of steel or Vitallium.
High corrosion resistance is one of its exceptional properties due to formation of titanium
dioxide layer spontaneously with exposure to air, preventing further oxidation. Despite this
corrosion resistance, titanium can still be found in the adjacent soft and hard tissues although
in minute quantities, as compared to Ni-Cr and Co-Cr alloy implants. Its great limitation is its
cost.
Leinbenger system is used as titanium plates for fracture reduction.
Stainless Steel: It is presently the most widely used surgical implant alloy. The primary
constitutions of 316 L are chromium, nickel, manganese, molybdenum and carbon which are
essential trace elements that exist in body fluids under physiologic regulation and with
precise function. 316 L falls within the austenitic range.
It is biologically well tolerated, has a yield strength that is less then Vitallium and titanium
but sufficient enough to withstand the bending and tortional forces of 60-100 DaN. The
stainless steel plates are adaptable and can be miniaturized but its resistance to corrosion is
much less than that of the other metallic implants. However, the corrosion reaction is usually
localized and rarely requires its removal. Maxillofacial implants are not loaded heavily and

49
therefore corrosion due to fretting between screws and plates is minimal. Being cheaper than
other metals, financial considerations dictate the choice of surgical stainless steel as implant
material for screws and plates.
Click herewww.faceart-clinic.com

50

51

52

53
TREATMENT Click here
www.faceart-clinic.com

54
GENERAL PRINCIPLES
The proper management of the fractured mandibular condyle is one of the most controversial
topics – if not the most controversial – in maxillofacial trauma. This controversy is reflected
in wide variety of opinions and proposed treatment modalities offered in the literature. The
commonly accepted and generally agreed on goal of treatment is the reestablishment of the
preoperative function of the masticatory system. This restoration typically involves the
reestablishment of the preoperative relationship of the fracture segments, the occlusion, and
maxillofacial symmetry. Unlike fractures of other bones, however, the exact anatomic re-
approximation of the fracture segments may not be absolutely essential. This fact is certainly
demonstrated in children in whom a conservatively treated displaced or dislocated condylar
fracture can heal with a perfectly functional and often morphologically reconstituted condylar
process despite lack of exact reduction at the time of injury. This is no doubt related to the
remarkable remodelling capacity of bone in children. A similar tendency exists in older
patients, although it is much less pronounced. Therefore a perfect radiographic alignment of
fracture segments should be considered inadequate if the restoration of a fully functioning,
relatively pain-free joint is not simultaneously achieved.
Historically, early management of condylar fractures consisted of various methods and
lengths of time of immobilization of the joint. This situation was based on the relatively good
results obtained and a degree of caution regarding the complications of surgical exposure of
the temporomandibular region. The initial methods of internal fixation also probably had
little advantage to offer over conservative methods. As surgical techniques were improved
and rigid fixation developed, a number of surgeons became comfortable with open
approaches to the joint. From this development evolved an expanding set of indications.
However, controversy followed closely and stimulated a great deal of debate, which still
permeates the current literature.
Treatment is generally divided into two schools: conservative, or nonsurgical, and
surgical approaches. We discuss the advantages, disadvantages, and indications for each of
these treatment options and surgical access to the TMJ.

55
CONSERVATIVE TREATMENT
As mentioned previously, the goal of management in general is restoration of proper form
and function. The surgeon should use the simplest technique that allows this goal to be met
while minimizing complications. The vast majority of data available support the belief that
fractures of the mandibular condyle can be successfully treated, with the establishment of a
functionally acceptable joint, through conservative means.
A number of investigators have published follow-up data on condylar fractures treated
conservatively, and the overwhelming opinion is that this method of treatment is preferred in
nearly all cases. In 1947 the Chalmers J. Lyons group published their data on 140 cases of
condylar fractures, with an average follow-up of 5 years (range 8 months to 19 years). They
found functional disturbance of any kind in only seven cases (5.8%). All these disturbances
were deemed mild, did not interfere with adequate function, and included limitation of
motion in lateral excursion, deviation in opening, interocclusal mal-relationship, and mild
joint noise during function. In 1952 MacLennan followed 180 cases for 14 to 37 months. He
reported an overall complication rate of approximately 20%, including 29 patients with
deviation on opening and 7 with visible deformity. In 1953 Kromer reported on 154 cases of
condylar fractures with an unspecified follow-up interval and found only 14 cases with
persistent functional disability (9.1%). In his series, there was one case of ankylosis in a 12
year old boy as a result of a bomb blast, with major damage and foreign body penetration of
the TMJ. In 1961 Blevins and Gores compiled data on 90 cases through clinical and survey
follow-up. A 14% complication rate was found. Finally, in 1989 Dahlstrom et al studied 36
patients with a follow-up of 15 years. In 14 children there was good masticatory function, no
disturbance in the growth of the maxillofacial region, and no evidence of earlier fracture. In
the adults examined, there was markedly less restitution of the condyle, with major signs of
masticatory dysfunction. This dysfunction, however, was not bothersome to the patients.
Teenagers in their series lay somewhere intermediate to the adult and children. Again there
were few subjective symptoms. Taken together the average complication rate over all these
studies was approximately 15%.
These authors and others derived several conclusions, including: 1) there is no correlation
between radiographic findings and either preoperative symptoms or postoperative function,

56
2) complications are uncommon with conservative therapy, and 3) the majority of evidence is
in favour of conservative treatment.
There are also animal data to support the effectiveness of conservative therapy in the
management of condylar fractures. Surgically induced condylar “fractures” were studied, and
a remarkable degree of regenerative capacity in the components of the injured joint was
found. A workable, usable mandibular articulation resulted regardless of whether the
condylar was left remaining at a right angle to the ramus, was pushed medially or anteriorly,
or was reduced and maintained by transosseous wiring. Each mandible produced a
morphologically identifiable condyle in the upright position. There was little sacrifice of
mandibular growth or symmetry. In another study, comparison was made between three
different treatment groups, which included reduction with wire fixation and immobilization,
closed reduction with immobilization, and no treatment. No difference was found between
the three groups with respect to time of healing.
The conservative management of condylar fractures may be as simple as observation
and soft diet or may encompass variable periods of immobilization followed by intense
physiotherapy. If the patient is able to establish and maintain a normal occlusion with a
minimal amount of discomfort, no active treatment may be needed. The patient should be
encouraged to adhere to a soft diet and maintain as nearly normal function as possible. Close
supervision is mandatory – and at the first sign of occlusal instability, deviation with opening,
or increasing pain – both clinical and radiographic re-evaluation should be performed. Any
one of these findings may signal the conversion of a non-displaced fracture to a displaced one
requiring active treatment. Only responsible patients who are committed to a period of close
follow-up should be considered for the “observation only” treatment regimen.
In general some degree of malocclusion, deviation with function, and/or pain is present
when some form of immobilization is required. Immobilization usually involves
intermaxillary fixation with arch bars, eyelet wires, or splints. The period of immobilization
is controversial and must be long enough to allow initial union of the fracture segments but
short enough to prevent complications, such as muscular atrophy, joint hypomobility, and
ankylosis. In the past, periods of as long as 8 weeks were used but have since shown to be
unnecessarily long. Currently the period of immobilization ranges from 7 to 21 days. This
period may be increased or decreased based on concomitant factors, such as age of the

57
patient, level of the fracture, degree of displacement, and presence of additional fractures.
Children require special consideration, which is discussed in a subsequent section.
Probably more important than the length of immobilization is management following the
release of postimmobilization treatment. This therapy allows a return of mandibular range of
motion and functional movements that were hindered by the injury and assists the
neuromuscular system in adapting to alterations in occlusion, joint position, or morphology.
Following the release of intermaxillary fixation, there is usually some degree of deviation,
and guiding elastics should be used to direct the mandible to its maximal intercuspation. The
patient is encouraged to function as normally as possible and is also instructed in range of
motion exercises. The guiding elastic are placed lightly during the day to promote increased
mobility and more tightly at night to maintain the occlusion. As the functional capabilities of
the patient improve with time, the period of elastic guidance is decreased. It may be
necessary for the patient to wear the elastics only at night while sleeping. Once the occlusion
remains stable and there is minimal pain with function, the elastics may be discontinued, and
the arch bars removed.
Until the mid 1980s, there is a large body of evidence to support closed reduction
techniques for treatment of condylar fractures. However, with the improvement in internal
rigid fixation coupled with a better understanding of the surgical anatomy and access to the
TMJ, there has been a resurgence in the literature advocating open reduction techniques,
citing earlier return of joint function and improved range of motion with less dietary
disturbance as benefits over closed reduction techniques.

58
Management with closed reduction
Erich arch bar
Ivy Loops

59
Gunning splint
MMF screws

60
OPEN REDUCTION OF CONDYLAR FRACTURE
The vast majority of available of available data support closed reduction as the treatment of
choice for condylar fracture. In an attempt to avert the complications associated with closed
reduction, many surgical approaches and methods of reduction and fixation have been
advocated. Surgeons supporting these methods have supplied few long term follow-up data,
however, to establish these methods as being superior to closed reduction. The complication
rates that have been reported are often higher than those attained with closed reduction.
Surgical reduction also introduces new complications not seen with closed techniques,
including damage to the facial nerve and unaesthetic scar formation.
Konstantinovic and Dimitrijevic compared 26 surgically and 54 conservatively treated
unilateral condylar fractures with regard to clinical function and radiographic reduction of the
fracture segments. After 1 year, there was no significant difference clinically between the
groups with regard to maximum opening (surgical mean, 39mm; conservative mean, 39
mm)and lateral or protrusive movements. No complications were seen in the conservative
group, and a 15.4% rate of complications was found in the surgically treated group.
Takenoshita et al also compared functional recovery after closed and open repair, with a 2-
year follow-up. They found that at 1 month following the release of intermaxillary fixation,
there was no difference in the maximum opening more quickly than did those treated
surgically. At the conclusion of the study, the average opening was comparable with the
conservatively treated group (50mm) and the opening of the surgically treated group (39mm).
All patients attained good occlusion with minimal pain during function. No cases of infection
or ankylosis were found.
Work by Ellis has indicated that open techniques for condylar reduction and fixation
produce more reliable occlusal results when treated open rather than closed. In a study of 137
patients with unilateral condylar injuries, 77 patients were treated closed and 65 patients were
treated open. Patients treated by closed reduction techniques had a notably greater percentage
of malocclusion compared with open reduction despite the fact that the severity of the initial
injuries was greater than in the group treated by open reduction. Throckmorton and Ellis
showed that patients treated with open reduction achieve normal incisal opening and
excursive movements sooner than patients treated with closed reduction. In a study of 130
patients, 74 were treated closed and 62 were treated open with 52 control subjects. Normal
values of interincisal opening were seen in all subjects after 3 years. However, the rate of

61
recovery is significantly faster in the group treated with open reduction versus closed
reduction (0.43mm/month and 0.15mm/month, respectively).
The most common reason that closed reduction techniques are favoured is related to
prevention of postsurgical complications. The most common complications from open
reduction of condylar fractures are facial nerve palsy and unsightly facial scarring. However,
in a study by Ellis evaluating the complication rate in 178 patients, 93 were treated by open
techniques. At 6 weeks postoperatively, 17.2% of patients had some degree of facial
weakness; the majority of these had resolved by 6 months. Surgical scarring was also judged
as wide or hypertrophic in 7.5% of cases. Their conclusion was that surgical complications of
open treatment of condylar fractures that lead to permanent dysfunction or deformity are
uncommon.
Ellis demonstrates further support for open reduction to re-establish anatomic
orientation of the condylar process. In a study of 146 patients, 81 were treated by closed
techniques and 65 treated by open techniques. Towne’s and panoramic radiographs taken at
serial intervals were used to qualify the degree of displacement. Of the condylar process and
ramal height post treatment. Patients treated by closed reduction had significantly shorter
posterior facial height on the side of injury, leading to a greater degree of facial asymmetry
than in the group treated by open reduction.
Re-establishment of preoperative occlusion is the gold standard in any fracture reduction
method. Ellis et al showed that patients treated with open reduction versus closed reduction
had consistently better occlusal results.
Despite a current body of evidence to support open techniques for all condylar fractures,
there does seem to be a specific group of individuals who will benefit from surgical
intervention. Zide and Kent, Raveh et al, and others have proposed a set of both absolute and
relative indications for open reduction of the fractured mandibular condyle. They stress,
however, the need for careful evaluation of each case on an individual basis. The current
indications for open reduction are as follows:
Absolute Indications
1. Displacement of the condyle into the middle cranial fossa
2. Impossibility of obtaining adequate occlusion by closed techniques
3. Lateral extracapsular dislocation of the condyle

62
4. Foreign bodies within the capsule of the TMJ
5. Mechanical obstruction impeding the function of the TMJ
6. Open injury (penetrating, lacerating, and avulsive) to the TMJ that requires immediate
treatment.
Relative Indications
1. Bilateral condylar fractures in an edentulous patient when splints are unavailable or
impossible because of severe ridge atrophy
2. Unilateral or bilateral condylar fractures when splinting is not recommended because
of concomitant medical conditions or when physiotherapy is not possible
3. Bilateral fractures associated with comminuted midfacial fractures
4. Bilateral fractures associated with other gnathologic problems
Displacement of the condyle into the middle cranial fossa severely limits the mandibular
range of motion and may cause intracranial damage. Most authors think that the condylar
segment should be surgically addressed. Some, however, advocate leaving the segment
intracranially and achieving a functional joint via condylotomy. This procedure will be
discussed later in the section on complications. The inability to obtain adequate occlusion
may be secondary to mechanical obstruction caused by severely displaced fracture segments.
In addition, delay in repair may allow soft tissue in growth into the fracture, inhibiting
reduction of the segments and resulting in persistent malocclusion. Severe displacement or
dislocation fractures may also be impossible to adequately reduce manually with closed
techniques, necessitating open reduction. Lateral displacement of the condylar segment
impedes proper function by creating a mechanical stop. Invasion of the TMJ by a foreign
body (e.g., a gunshot wound) usually causes comminution of the bony segments. These
fragments may interfere mechanically with proper joint function, act interfere mechanically
with proper joint function, act as a nidus for infection, and increase the risk of ankylosis. It is
generally recommended that surgical removal of foreign bodies be delayed foe 7 to 10 days
to allow edema to subside and some fibrosis to occurs around the foreign body. This fibrosis
may aid in localization and removal of the fragments.
Relative indications include edentulous patients with bilateral fractures in whom splints
are not available or are not usable, as in the patients have no reference point with which to
establish the proper condyle-fossa relationship; therefore direct visualization may aid in

63
attaining adequate reduction. Bilateral fractures with concomitant fractures pose a similar
problem in that no stable reference point exists for reconstructing the midfacial complex. The
mandible is repaired first with the use of open reduction and internal fixation to provide a
stable platform on which the remaining midfacial fractures are repaired. The presence of
other important medical conditions may make it impossible to use intermaxillary fixation or
to perform physiotherapy. Some of these conditions include uncontrolled seizure disorders,
psychiatric problems, alcoholism, mental retardation, and neurologic injury. Some believe
that severe chronic obstructive pulmonary disease and other respiratory conditions are also
relative indications for open reduction because of the increased upper airway resistance that
results from intermaxillary fixation.
Once the decision is made to use an open technique, the next step in treatment planning
is to select a surgical approach. Over the years, many approaches to the TMJ have been
developed, including horizontal incisions over the zygomatic arch and intraoral, preauricular,
endaural, postauriclar, submadibular, retromandibular, and rhytidectomy approaches. Each
has its own advantages, disadvantages, and complications. Many of these approaches have
fallen from use, and only the preauricular, submandibular, and retromandibular incisions with
various modifications, and occasionally the intraoral route, are routinely employed in most
centers.
The location of the fracture and the degree of displacement are the prime determinants in
the selection of the approach used to access the joint. If the fracture is intracapsular or high
on the condylar neck, the preauriclar or endural approach is preferred. Either one offers better
access, greater visibility of the fracture site, ease of manipulation of the soft tissue within the
joint, and relative ease of placement of fixation devices. The major disadvantages of these
approaches include the possibility of damage to the facial nerve and the presence of a facial
scar. Fractures located lower on the condylar neck and subcondylar fractures may be more
easily accessed via a submandibular approach. The danger of this technique is possible
damage to the marginal mandibular nerve, with subsequent weakness of the depressor
muscles of the lower lip. In some cases, a combination of these approaches must be used to
gain adequate access to reduce and fixate the fracture segments. Several authors have
advocated an intraoral approach to fractures of the condyle. This approach offers the
advantages of visualization of the fracture reduction and the occlusion simultaneously,
minimal risk of damage to the facial nerve, and the prevention of an unaesthetic facial scar.

64
The disadvantage include more limited access, especially in high subcondylar and condylar
neck fractures, and difficulty in placing certain fixation devices.
PREAURICULAR APPROACH.
This preauricular incision has been widely used for approaching the ear and the TMJ.
Historically an early description was provided by Blair, who used an inverted L incision,
beginning within the temporal hairline and progressing inferiorly just anterior to the anterior
auricle. Since then many modifications of the basic incision have been made. Dingman and
Grabb modified the incision by making the angle between the vertical and the superior
portions of the incision more obtuse and rounding the angle of intersection. Others, including
Lempert and Shambaugh, modified the incision by carrying it to varying degrees behind the
tragus and into the external auditory canal, creating the endural incision.
When the preauricular approach is performed, a cotton pledget moistened with mineral
oil is placed into the external auditory canal to prevent debris and hemorrhage from
accumulating and possibly damaging the tympanic membrane. Next, anesthetic solution is
infiltrated into the preauricular skin and the joint capsule to aid in hemostasis. The incision is
begun within the hairline of the temporal skin approximately 1.5 to 2.0cm anterosuperiorly
to the superior attachment of the helix. The incision is made through the skin, passing in a
gentle curve to the superior attachment of the helix, where it is continued inferiorly within the
skin crease just anterior to the auricle. The incision is continued in this crease to the junction
of the inferior helix and the skin of the cheek. Care should be exercised in the lower extent of
the incision so as not to penetrate too deeply, as the main trunk of the facial nerve passes
within several centimetres of the earlobe before it enters the posterior aspect of the paroid
gland.
In the area superior to the zygomatic arch, incision is deepened to the level of the
temporal fascia. Immediately over the zygomatic arch, the incision is carried to the
periosteum over the bone. Below the arch, the incision follows just superficial to the tragal
cartilage. Any vessels encountered during the dissection should be clamped, transacted, and
ligated to allow adequate access.
The temporal fascia is then incised several millimetres anterior to the initial incision.
The dissection is carried anteriorly and inferiorly between the temporal fascia and the muscle
fibres of the temporal muscle. This plane is continued inferiorly to the level of the

65
decussation of the temporal fascia into the superficial and deep layers. At this point, the
dissection is continued to the superior edge of the zygomatic arch within the fatty tissue
pocket between the two layers of the temporal fascia. Thus in the superior region of the
dissection, a flap is created consisting of the skin, subcutaneous tissue containing the
superficial temporal vessels and branches of the facial nerve, the superficial layer of the
temporal fascia, and more superiorly the temporal fascia. The branches of the facial nerve are
well protected within this soft tissue flap.
When the zygomatic arch has been reached, an elevator is used to reflect the periosteum
from the lateral aspect of the arch. Reflection can be carried anteriorly as far as the glenoid
tubercle. This reflection should be done carefully, as the periosteum, temporal fascia, and
subcutaneous tissue coalesce to form a single layer in this region, and the temporal branch of
the facial nerve lies within this tissue as it passes over the arch toward the scalp.
Below the arch, the dissection is continued beneath the parotidomasseteric fascia, which
is a continuation of the temporal fascia from above. The flap is lifted anteriorly, as a single
unit, thus exposing the joint capsule and temporomandible ligament. The dissection is carried
inferiorly as needed until the fracture site is carried inferiorly as needed until the fracture site
is adequately exposed. Inferiorly the parotid gland is reflected anteriorly with the skin fascial
flap, protecting the gland and facial nerve.
The endural approach is similar but differs in that the initial incision is made to pass
along and just inside the lateral aspect of the tragus. The remainder of the skin incision is the
same. The dissection in the area of the tragus is carried to the root of the zygomatic arch in a
plane just above the perichondrium of the tragal cartilage. Once the dissection reaches the
level of the arch, it is similar to the preauricular approach. This incision has the added
advantage of a less conspicuous scar compared with the preauricular incision.
SUBMANDIBULAR APPROACH.
The submandibular, or Risdom, incision is the approach of choice for low subcondylar
fractures. It allows good exposure to the level of the neck and coronoid notch. The incision
has been modified by Blair to expose the parotid gland for procedures on the same. There is a
reduced risk of injury to the temporal and zygomatic branches of the facial nerve but an
increased risk of damaging the marginal mandibular branch.

66
The incision is made within the relaxed skin tension lines approximately 2cm inferior to
the inferior border of the mandible in the region of the angle. The Blair modification places
the incision slightly posterior to this point and curves slightly superiorly behind the angle.
The incision is made through the skin and sudcutaneous tissue. Depending on the location of
the incision, the posterior fibres of the platysma muscle may be identified. Near the posterior
aspect of the incision, the strenocleidomastoid muscle is visible with its fibres running in a
posterosuperior to anteroinferior direction. A nerve stimulator may be useful in locating the
marginal nerve, the cervical nerve, and possibly the main trunk of the facial nerve as the
dissection proceeds. The platysma muscle is divided, and the dissection is continued bluntly
in a superior and medial direction. At this point, the angle of the mandible should lie fairly
close to the surface. External jugular, retromandibular, and facial vessels may be encountered
during this approach and may require ligation. Once the inferior border of the mandible is
reached in the region of the angle, the fascia of the pterygomasseteric sling is sharply incised.
A periosteal elevator is used to reflect the periosteum over the lateral aspect of the angle and
ramus, extending superiorly to the sigmoid notch. This length of reflection should allow
adequate exposure of most subcondylar and some low-neck fractures. If additional access is
necessary, the tissue at the posterior aspect of the incision may be further released, allowing
the pored gland with its contained facial nerve to be further retracted anteriorly. Greater care
must be exercised during any dissection in the deeper tissue just inferior to the auricle, as this
is the location of the main trunk of the facial nerve as it courses from the styloid foramen to
the posterior aspect of the parotid gland.
RETROMANDIBULAR APPROACH.
From its original description by Blair for access to an ankylosed TMJ, the
retromandibular approach to the TMJ is becoming increasing popular. It is a versatile
approach to fractures of the body, angle, and subcondylar fractures to the level of the
coronoid notch. This approach also allows distraction of the angle of the mandible, allowing
fracture reduction and fixation. With the use of transfacial trocars this approach may also be
used to rigidity fixate high level condylar fractures. As compared with the sudmandibular
approach, the retromandibular approach is associated with significantly less injury to the
marginal mandibular branch, temporal, and zygomatic branches of the facial nerve.

67
The incision is placed in the resting tension lines in the lateral neck. The incision is
typically 2 to 3 cm in length and placed 1 cm inferior and posterior to the angle of the
mandible. The incision is placed through skin and subcutaneous tissue. The posterior aspect
of the playsma may be identified and carefully divided. Through the subplatysmal plane, the
superficial layer of the deep cervical fascia is encountered. Peripheral nerve testing should be
employed to identify the cervical and marginal mandibular branch of the facial nerve. The
cervical branch runs vertically, usually out of the surgical field. However, the marginal
mandibular branch may run transversely across the surgical field and limit exposure of the
mandible. If the marginal branch is encountered, it should be dissected free from the adjacent
soft tissue to facilitate its retraction. Further blunt dissection reveals the sternocleidomastoid
muscle posteriorly and the capsule of the submandibular gland anteriorly. The tail of the
parotid gland may be encountered in this time. Dissection into the parotid capsule should be
avoided to prevent inadvertent injury to the facial nerve. The retromandibular space is then
entered with blunt dissection. This space lies at the midpoint between the anterior surface of
the sternocleidomastoid muscle and the posterior aspect of the submandibular gland. The
angle of the mandible should be palpable at this point. The external jugular vein, posterior
facial artery, retromandibular veins, and facial artery may be encountered and require
ligation. Once the retromandibular space is entered, the dissection is carried superiorly to
encounter the angle of the mandible. The pterygo-masseteric sling is encountered and sharply
incised along the aponeurosis to expose the lateral border of the mandible. The overlying soft
tissue including the paroid gland is then retracted to facilitate further fracture exposure. The
main advantages of this technique are the ease and rapidity with which the dissection can be
performed. Compared with the submandibular incision, the retromandibular incision is placed
closely to the angle of the mandible. Therefore the extent of soft tissue dissection required to
expose the mandible is limited. The posterior position of this approach is associated with a
reduced risk of facial nerve injury.
RHYTIDECTOMY (FACE-LIFT).
The rhytidectomy or face-lift approach to the mandible ramus and condylar region is a
variant of the retromandibular approach. The main difference is the placement of the incision.
The approach can provide greater exposure to high–level condylar fractures, providing
excellent cosmesis. However, it requires additional time for closure. The initial incision is
placed through skin and subcutaneous tissue. A skin flap is then raised superficial to the
superficial musculo-aponeurotic sheath (SMAS). The dissection is extended toward the angle

68
of the mandible with tenotomy scissors to create a widely undermined subcutaneous pocket
that extends 2cm anterior to the posterior border of the mandible. The plane superficial to the
SMAS is relatively avascular without major anatomic structures. Just below the SMAS lies
the greater auricular nerve (C2-C3). Once the skin flap is raised and retracted, the underlying
lateral surface of the mandible can be visualized. The remainder of the dissection is identical
to the retromandibular approach.
POSTAURICUALR APPROACH.
Although rarely used this approach does have certain advantages. The postauricular
approach provides excellent exposure to the entire TMJ. The ability to camouflage the scar in
a postauricular fashion is beneficial, especially in patients who have a tendency to form
hypertrophic scars. The main disadvantage of this procedure is auricular stenosis. The
postauricular approach is contraindicated in the presence of joint infection or chronic otitis
externa. The incision is placed 3 to 4 mm posterior to the auricular flexure and extended
toward the mastoid fascia. Superior to the mastoid fascia, the incision exposes the superior
and posterior circumference of the external auditory canal. Blunt dissection below the
external auditory canal creates a plane running anteriorly to separate the pinna. A blade is
then used to transect the external auditory canal and retract the ear anteriorly. Dissection is
then carried through the superficial layer of the temporalis fascia to the root of the zygoma.
Once the joint surgery is completed, the ear canal is reapproximated by closure of the
overlying skin flap only.
INTRAORAL APPROACH.
Steinhauser first described an intraoral approach to the fractured condyle in 1964.
Others, including Niederdellmann, Jeter et al, and Lachner et al, also advocate the use of this
approach. Lachner initially described the technique for the treatment of low subcondylar
fractures but later expanded its use to all extracapsular fractures.
An incision is made along the anterior border of the ascending ramus, extending
anteriorly along the external oblique and ending in the vestibule adjacent to the second molar.
A full-thickness mucoperiosteal flap including the masseter muscle is reflected, exposing the
lateral aspect of the mandible to the posterior border. The subperiosteal dissection is
continued superiorly to the level of the sigmoid notch. A retractor can be placed in the
sigmoid notch to aid in access. The proximal condylar fragment is then identified and

69
reduced. It may be necessary to distract the mandible inferiorly to locate a medially displaced
condyle. The periosteum of the condylar segment is stripped, with care taken to elevate only
enough periosteum to allow placement of fixation plates or wires. This minimal stripping
prevents unnecessary compromise of the vascular supply to the condyle. Intermaxillary
fixation is then applied with the condyle reduction into its proper position. One advantage of
this technique is that the condylar segment can be directly visualized during the application of
the intermaxillary fixation. Proper reduction is confirmed by inspection and palpation of the
posterior border with an instrument.
There are circumstances in which none of the mentioned surgical approaches are
sufficient to gain exposure to the mandible condyle. For example, one circumstance is a
fracture-dislocated mandibular condyle displaced into the middle cranial fossa. There are
only approximately 30 reported cases in the literature of this unusual event. To facilitate
fracture reduction, a combined hemicoronal or bicoronal incision allows exposure for
reduction and fixation. A multidisciplinary approach with neurosurgical consultation allows
for transcranial repair of the glenoid fossa and dural perforations concomitantly with condyle
fracture reduction and fixation.

70
Surgical approaches to the Condyle
Pre auricular incision
Modifications of pre auricular incision

71
Endaural approach

72
Al-kayat Bramley incision

73
Submandibular incision
Post ramal incision

74
REDUCTION AND FIXATION OF THE FRACTURE SEGMENTS.
Following adequate exposure of the fracture site, the segments must be reduced to their
preinjury position. In the case of minimal displacement, this reduction is accomplished by
manipulating the proximal fragment into position with a haemostat or another instrument.
When the condylar segment is more notably displaced, or is dislocated from the fossa,
reduction becomes more difficult. Owing to the pull of the lateral pterygoid muscle, the
condylar fragment is usually located anterior and medial to the mandible. Distraction of the
mandible in an inferior direction – via a clamp, towel clip, or stainless steel wire placed at the
angle – aids in visualizing and manipulating the condylar segment. The condylar segment is
then grasped and reduced into its proper location at the mandibular ramus. In 1991 Stewart
and Bowerman suggested inserting a Moule pin into the condyle to assist in positioning this
small fragment. Once the fragment is reduced and secured, the pin is removed before wound
closure. For severe medial dislocation of high condylar fractures that cannot be adequately
reduced with other methods, Mikkonen et al and Ellis and Dean advocate a submandibular
approach for access and a vertical ramus osteotomy with subsequent removal of the posterior
ramus. This procedure allows increased access to and visibility of the medially positioned
condyle. The surgeon then grasps and removes the condylar fragment while keeping the
capsule and disk intact. The posterior ramus and condyle are then taken to the back table,
where they are placed into their proper anatomic relationship and secured with a single
obliquely placed 2.0mm lag screw. The ramus condyle then is treated as a free autologous
bone graft, returned to the field, and secured with two small bone plates. The concern here is
the necessary extensive stripping of the vascular supply to the condyle and the possibility of
avascular necrosis. Both Mekkonen and Ellis reported little dysfunction in the joint that were
operated on and no radiographic evidence of irreversible changes. Arthritic changes were
minimal. They also make reference to the fact that in tumour surgery requiring mandibular
resection, if the condyle is found to be uninvolved, it is repositioned within the fossa with
generally good results. In addition, work with rhesus monkeys has demonstrated no histologic
difference between the condylar cartilage that underwent subcondylar osteotomy and
detachment followed by repositioning and the condyles not operated in the same subjects.
The next step is the choice of a fixation technique to maintain the position of the
segments achieved through open reduction. Some surgeons choose not to apply any fixation
following reduction of the condyle. This option is not advisable in that the same muscular

75
pull that caused the initial displacement or dislocation will be free to re-dislocate the reduced
fragment. Such a situation would be unfortunate indeed.
Historically a wide array of fixation techniques have been used, including suture
ligatures, external fixation, K wires, osteosynthesis wire, axial anchor screws and rigid plates
and screws. With advances in biomaterials, downsizing of hardware, and availability of
instrumentation in most operating rooms, rigid fixation with plates and screws is the most
common method currently in use. These plates offer increased stability in three dimensions
versus osteosynthesis wires or K wires. Placement can usually be accomplished through any
of the commonly used incisions. Percutaneous trocars have also been developed to facilitate
accurate screw placement in areas in areas of difficult access.
Early reports of open repair of condylar fractures typically used various nonrigid
fixation techniques. Wire ligature fixation in various configurations was described by Henny,
Thoma, Messer, and Tasanen and Lamberg. Wire fixation is usually employed in conjuction
with some length of intermaxillary fixation. Tasanen and Lamberg treated 27 patients via a
submandibular approach with some form of transosseous wiring combined with
intermaxillary fixation (average length, 22.6 days). Follow-up was on average 11.6 months.
Postoperatively, average maximum opening was 41.5mm. They noted a slight deviation on
opening in about half of the cases, and lateral mandibular excursions were within normal
limits. Three cases displayed slight weakness of the marginal mandibular nerve.
Radiographic evaluation showed some shortening and remodeling in most cases. Slight
angulation of the segments was found in about half of the cases. Joint function was
determined to be normal in 24 of 27 cases.
In an attempt to attain more stable fixation, several techniques involving Kirschner wires
were developed. In 1952 Stephenson and Graham initially described the technique of passing
a Kirschner wire from the inferior border of the mandible, in the angle region, through the
medullary space to exist the fracture site. The pin was then passed into the condylar segment
after proper reduction of the fragment. Lund and Takenoshita and associates also describe
similar techniques with satisfactory results. The technical demands and the possibility of
passing the tip of the wire through the auricular surface of the condylar head have led to the
infrequent use of this method.
Interestingly a technique described initially by Petzel and advanced by Krenkel involves
the use of an axial anchor screw method based on lag screw principles. A biconcave washer

76
is also used, which the investigators claim allows greater tightening of the screw and
increased compression at the fracture site. The procedure is extremely technique sensitive and
necessitates special instrumentation.
The mandible is exposed via a submandibular incision, which allows access to the
inferior border and the entire lateral ramus. A groove is drilled in the lateral ramus to within
several centimetres of the fracture line. Several drill guides are then used to create a hole
2mm in diameter extending to the fracture line. A space for the biconcave washer is also
created within a countersink bur. A smaller diameter drill guide is then fitted and attached to
the sigmoid notch retractor. Following reduction of the condylar segment, a hole 1.5mm in
diameter is prepared into the condylar fragment approximately 1 to 2cm in length, the hole is
then measured and tapped, and a titanium screw is placed and tightened. The screw is a lag
design with a threadless mid portion. Once the screw is tightened, compression is generated
at the fracture site, providing a rigid, stable reduction. Silvernoinen et al used this technique
on seven patients with condylar fractures and found correct reduction in 71% of cases. Three
patients had some complication. In one edentulous patient with thin cortical bone in the
condylar neck, fracture of the bone overlying the screw occurred, with subsequent angulation
of the condyle. In another case, reduction of the condyle was inadequate with an
interfragmentary gap of 1 to 2mm. This complication precluded any compression and
resulted in mobility and pseudoarthrosis. The author suggests that these problems would
probably be overcome with further experience and improved patient selection.
Currently the majority of open reductions are secured using rigid fixation techniques
involving miniature bone plates and monocortical screws. Ellis et al (1989, 1993) use a
submandibular-retromandibular approach. Koberg and Momma (1978) and Chuong and
Piper(1988) use the preauricular approach described by Al-Kayat and Bramley. Jeter et al
(1988) and Lachner et al (1991)prefer an intraoral technique. Lachner et al reported on a
series of 14 patients treated with rigid plate and screw fixation applied through an intraoral
approach. The average follow-up was 12 months and consisted of clinical and radiographic
examinations. A total of 80%of cases displayed adequate reduction radiographically, with a
gap of less than 2mm. All patients had a normal range of motion within 8 weeks. Slight
deviation on maximum opening was seen in about one quarter of patients. A total of 53% of
patients had pain with maximal chewing force but required no analgesics. Four patients
displayed joint noise on the operated side, but two of these also had similar symptoms
preoperatively. At 6 months, all patients were functioning satisfactorily and required no

77
interventions. The author suggested that the results were in general better than those obtained
with closed reduction of similar fractures.
In the severely traumatized TMJ, when the need exists for immediate joint
reconstruction there is controversy regarding which type reconstruction – autologous versus
alloplastic – should be employed.
Autologous reconstruction harvest sites have included metatarsal, scapular, clavicular,
and costochondral. All sites have advantages and disadvantages and are associated with
different donor site morbidity. The literature lends support to the costochondral graft being
the graft of choice for autologous joint reconstruction. The costochondral graft is reported as
having superior functional outcomes, adaptability, and growth potential in the pediatric
population. It is associated with a lower incidence of ankylosis when compared with other
autologous grafts. The disadvantages of autologous grafts include ankylosis; resorption;
unpredictable growth patterns, especially in the pediatric population; and donor site morbidity
the costochondral graft should be avoided in elderly patients and those with significant
respiratory disease. Patients with concomitant thoracic injuries or chronic obstructive
pulmonary disease (COPD) are at notable risk of postoperative morbidity from splinting,
hypoventilation, atelectasis, pneumonia, and respiratory collapse. When autologous
reconstruction is not medically appropriate, alloplastic joint reconstruction is the only viable
option. Alloplastic TMJ implants have rapidly evolved over the last 10 years.
Currently there are only two stock TMJ replacements systems that are in use, the
Biomet prosthesis (Biomet, Jacksonville, Fla) and the Christiansen prosthesis(TMJ Implants,
Golden, Colo). In circumstances of notable destruction of the anatomic structures of the TMJ
region and malar arch, such that a stock prosthesis cannot be adapted or would be too
unstable, the only viable alternative is a custom fabricated CAD/CAM Total
Temporomandibular Joint Reconstruction System (TMJ Concepts, Ventura ,Calif.). Currently
TMJ concepts is the only custom fitted system available and approved by the U.S. FOOD and
Drug Administration (FDA). The advantages of alloplastic TMJ reconstruction in the
traumatized joint include lack of growth potential, no graft remodelling or instability,
immediate fossa integrity, immediate function with postoperative physical therapy, and
prevention of donor site morbidity. Alloplastic joint reconstruction is contraindicated in
pediatric patients with incomplete facial growth, sepsis, or other infectious foci, and obtunded
patients who are unable to perform physical therapy. Although no long-term studies have

78
been performed on alloplastic reconstruction of the TMJ in the traumatized patient, there is
evidence in the patient with a chronic debilitating TMJ that total joint reconstruction is
successful. Mercuri has published 10 year data on the custom CAD/CAM TMJ prosthesis
citing 68% improvement in mean mandibular function and 76% reduction in mean pain
scores.
POST INTERMAXILLARY FIXATION MANAGEMENT.
Postoperatively, depending on the type of fixation used, a variable period of
intermaxillary fixation is required. The more rigid the fixation used, the shorter the period of
fixation. The length of time required should be long enough to allow initial union of the
segments but short enough to prevent the formation of adhesions within the joint. Generally a
period of approximately 7 to 21 days is sufficient, with a shorter period indicated for
children. Once the intermaxillary function has been removed, the occlusion is critically
evaluated as to opening, range of motion, and symptoms during function.
If the occlusion is stable and reproducible and if pain during function is minimal, the
patient should begin a closely supervised regimen of physical therapy. If malocclusion or
notable pain is present, an additional period of fixation or training elastics may be required.
The patient is encouraged to function during the waking hours and is instructed to replace the
elastics st bedtime. This regimen allows for stretching of the muscles and newly forming scar
tissue and guiding the occlusion until neuromuscular adaptation has developed. After 2 to 3
weeks of elastics, the occlusion is again evaluated. If it is stable with little pain, physical
therapy is begun. If occlusion remains unstable, consideration should be given to correction
via equilibration, orthodontics, or osteotomy. Notable pain with function could indicate an
internal derangement of the TMJ. Physical therapy is continued, the patient is placed on
analgesics as needed for pain, and a soft diet is continued. Once the patient is functioning
normally and with minimal pain, the arch bars are removed, and a region of periodontic
follow-up is begun.
Throughout the recovery period, it is imperative that the mandibular range of motion be
maintained to prevent permanent limitation or ankylosis. Preservation of range of motion can
be accomplished through the patient’s performing exercises in front of a mirror, placing
progressively increasing numbers of tongue blades between the central incisors, or the use of
a passive range-of-motion device. In any event, an aggressive, closely monitored and
supervised program of postoperative management is paramount to attaining optimal

79
functional result. Perfect reduction and absolute rigid fixation are useless if the range of
motion is minimal secondary to scarring or ankylosis.

80
Using elevators for reduction
Using condylar rectractors for reduction

81
Reduction with bone holding forceps
Wire osteosynthesis

82
Thoma’s wire osteosynthesis Robinson’s Messer’s
K wire osteosynthesis Axial lag screw

83
Mini plate osteosynthesis

84
CONDYLAR FRACTUREIN
CHILDREN
Click herewww.faceart-clinic.com

85
Facial fractures involving the pediatric population are relatively uncommon. This fact is
believed to be a result of the elasticity of the pediatric skeleton, the relatively small facial size
with respect to the more prominent skull of the child, and the decreased force involved in
most children injuries. With respect to facial fractures, the mandible is the second most
frequently fractured bone, after the nasal bones. In 1972 Hall reported a 20.7% incidence of
mandible fractures in 495 patients younger than 14 years of age. Kaban et al (1977) found
that 32% of 122 pediatric (younger than 16 years) facial fractures involved the mandible,
Carroll et al (1987) studied 268 facial fractures, of which 26.5% were mandibular. The
involvement of the condylar process is somewhat higher than that seen in the adult, ranging
from 40% to 60% (Aramatunga, Hall).
The cause of condylar fractures in the pediatric age group involves mechanisms similar
to those in adults but with altered incidence. Falls, including those from heights and bicycles,
constitute the most common cause of condylar fractures in children, with an incidence
between 30% and 50% of cases. Motor vehicle accidents are second in frequency (26% to
34%), followed by sports-related injuries (15%) and assault(3%). In most series, males are
affected more often than females, in a ratio of about 2 to 1. Not surprisingly, Carroll et al also
noted a seasonal variation in the number of fractures sustained by children, with an increase
during the summer months, when children are more active outdoors.
The increased proportion of condylar fractures may be explained in part by the
morphologic and anatomic differences between the pediatric and the adult condyle. First, the
morphology of the young condyle is unique. Until the age of 2 years, the condylar head is
richly vascular, being penetrated on the auricular surface by numerous small vessels. After 2
years of age, these vessels diminish in number, although the condylar head remains highly
vascular. The cortical bone of the condyle also differs in that it is much thinner than the adult
condyle. The condylar head id broader and fuller , and the neck is thicker than in the mature
version. The glenoid fossa is more shallow than that of the adult, which has a more concave
appearance with a steeper, more pronounced articular eminence. The bone quality is also
different, being softer and more pliable in the child. As the individual progress into
adolescence and adulthood, the condyle becomes less vascular, the bone becomes less
pliable, and the condyle assumes the adult configuration . the increased vascularity, combined
with the thinner cortical bone, makes the child’s condyle more susceptible to “burst” type

86
fractures, leaving multiple small, highly osteogenic fragments within the joint space, which
may increase the risk for joint ankylosis.
Clinically, fractures of the condyles in children are more difficult to detect. First, the child
placed in the setting of acute injury is often frightened and intimidated by the busy
emergency room and physicians who often are not accustomed to dealing with children.
Second, the child is less able to convey subjective symptoms of his or her injury. Finally the
physical examination is difficult at best. Children are often uncooperative, making detection
of an already subtle injury even more difficult. Radiographs are often hard to obtain in the
child, and because of the “miniaturized” anatomy, superimposition of structures makes
interpretation unreliable. With the advent of more rapid CT scanners and the use of sedation
techniques, the radiographic examination has been somewhat simplified. With the
aforementioned factors in mind, the wise clinician may opt to postpone an in-depth
examination with radiographs for as long as 24 hours to allow the child to overcome the
initial shock of the injury. Otherwise the signs and symptoms of condylar fracture in the child
are similar to those in the adults. These findings includes pain over the fractured joint, limited
opening and lateral excursions, deviation of the mandible toward the fracture in unilateral
cases and malocclusion. Again, bilateral cases result in anterior open bite with retrognathia
and difficulty with mandibular movements.
To understand the unique healing potential of the child, it is necessary to discuss growth
of the mandible in general. As the mandible develops, three growth centers are able to
produce enlargement of this complex bony structure: the condyles, the surface of the ramus,
and the alveolus.
Initially it was believed that the mandible was pushed down and forward by growth at the
condylar growth center. This concept has not been borne out by clinical research, in that the
condylar cartilage in vitro possesses little independent growth potential and produces only a
fraction of the growth pressure of epiphyseal cartilage. In addition, removal of the condylar
cartilage in experimental animals has shown little effect on growth. With the introduction of
the “functional matrix” theory by Moss in 1968, a new understanding of mandibular growth
was born. This theory, simply stated, suggests that the mandible – rather than being pushed
down and forward – is pulled there as a result of changes in the growing soft tissue envelope,
or functional matrix, surrounding it. Therefore growth at the condylar centre is secondary and
compensatory to these primary changes.

87
Numerous studies have appeared in the literature examining the effects of condylar
fractures on the function of the masticatory system, growth potential, and facial aesthetics.
The Chalmers J. Lyons Club, MacLennan and Simpson, Blevins and Gores, Lindahl, Lund,
Gilhuus-Moe, Miller, and animal studies conducted by Walker and Boyne are several of the
more notable. Myall provides an excellent review of the literature for the interested reader.
The conclusions reached by these authors confirm the concept that regardless of the type of
injury, the degree of fracture displacement, or the specific treatment used, the child has an
incredible ability to regenerate a morphologically, anatomically, and functionally normal
condylar articulation. It has also been seen that the younger the individual, up to
approximately 12 years of age, the more complete and rapid the restitution of the condyle. In
adolescents the potential for major regeneration and remodelling is present but to a lesser
degree than that in the younger child. The studies also overwhelmingly support the use of
conservative measures in the treatment of these injuries, with a very brief period of
intermaxillary fixation, approximately 7 to 10 days, being common. This period is followed
by active movement and function of the joint to reduce the formation of scar tissue and
prevent ankylosis. These studies also confirm the distinct paucity of clinically significant
signs or symptoms of masticatory dysfunction following fracture healing.
With this in mind, nearly all cases of condylar fracture in children are treated
conservatively, with immediate function, and analgesics as necessary for comfort. In cases
with significant pain or malocclusion, a brief period of intermaxillary fixation, on the order of
7 to 10 days, may be necessary, followed by active function. Similar to the case in the adult
population, it is essential to establish a closely supervised follow – up schedule. In the
actively growing child, the risk of ankylosis and growth disturbance with resultant facial
asymmetry amplifies this need. Ankylosis prevents the anterior and inferior distraction of the
mandible by its soft tissue envelope (as stated in the functional matrix theory). The opposite
condyle deposits appositional bone along its posterior and superior aspects. This process
results in a shortened ramus on the ipsilateral side and a normal or elongated ramus on the
contralateral side. Facial asymmetry and deviation of the chin midline toward the affected
side are the results. Early mobilization and active physical therapy aimed at maintaining or
increasing the range of mandibular motion prevent ankylosis and subsequent alteration in
growth.

88

89
COMPLICATIONS
Despite the satisfactory results obtained with both closed and open reduction of condylar
fractures, the potential for complications exists. These complications can be divided into
those occurring late in the post-treatment course.

90
EARLY COMPLICATIONS
Complications that occurs concurrent with or early after treatment of condylar fractures
include the following:
1. Fracture of the tympanic plate.
2. Fracture of the glenoid fossa with or without displacement of the condylar segment
into the middle crania fossa.
3. Damage to cranial nerves V and VII
4. Vascular injury.
A force transmitted through the mandible from anterior to posterior through the condyles
will be transferred to the tympanic plate. If force is great enough, fracture of the plate may
occur. Owing to the close proximity of the plate and the external auditory canal, the primary
symptom of this injury is bleeding from the external auditory canal. Injury to the skull base
and other facial structures should always be suspected.
Fracture of the base of the skull occurs in the region of the relatively thin glenoid fossa
and, occasionally, extends through the petrous portion of the temporal bone. When a blow is
received by the mandible, and particularly the chin, the force is transmitted directly to the
condyles and glenoid fossa. It is thought that the unique scroll-like shape of the condyle, with
its larger lateral pole, and the increased thickness of the lateral aspect of the fossa provide
protection against penetration of the condyle head into the cranium. In certain cases,
however, the condyle is more rounded in form, and this feature is thought by some to allow
increased concentration of forces on thin central portion of the glenoid fossa and possible
penetration of the condylar head into the middle cranial fossa.
Clinically, with penetration into the cranium, typical signs and symptoms of condylar
injury are seen in addition to the possibility of contralateral open bite secondary to shortened
ramus on the side of the injury with posterior occlusal prematurity. There is also almost
complete inability to move the jaw owing to locking of the condylar head into the fracture
site. If there was also a posterior component to the force, hemorrhage may occur into the
external auditory canal.

91
With fracture at the skull base, the possibility of cerebrospinal fluid leakage must be
considered. Intracranial hemorrhage is also seen, secondary to tears in the dura or middle
meningeal artery.
Plain radiographs are useful in the diagnosis of intracranial penetration but miss a fair
number of cases. Computed tomography offers increased detail of both bone and soft tissue
compared with standard films. It has the additional advantages of detecting intracranial blood
and other craniomaxillofacial fractures and requiring less patient cooperation. Disadvantages
of CT include radiation exposure and notably greater cost versus that of conventional
imaging.
Management of condylar displacement into the middle cranial fossa is based primarily
on several published case reports. Neurosurgical consultation is warranted to exclude cerebral
damage, intracranial hemorrhage, and cerebrospinal fluid leak. Management of the condylar
fragment has consisted of reduction of the condyle by various means, fixation of the fracture
fragments, and protection of the dura by placement of a cranial bone graft. Others prefer to
leave the condyle within the confines of the cranial vault and merely smooth the edges of the
fracture with a rongeur forceps. Still others report that the condyle should be reduced and
subsequently resected. Following reduction, most cases require some period of
immobilization with intermaxillary fixation. As in other fracture of the condyle, the period of
immobilization should be short, and active use of the joint should be encouraged as soon as
feasible. The early return to fixation may lend merit to the use of bone grafting in the
reconstruction of the fractured glenoid fossa.
When sufficient force is transmitted to the temporomandibular region to cause fracture
of the mandible and/or condyles, the contiguous and adjacent anatomic structures also receive
significant traumatic force. Damage to nervous and vascular structures may occur as a result
of their being stretched during the injury, lacerated or severed by the jagged edge of a
fracture segment, or iatrogenically damaged during surgical intervention. The facial nerve is
especially susceptible to damage during condylar injury and surgical approaches to the TMJ.
If fracture of the skull base occurs, the eighth cranial nerve may be injured, with resultant
neurosensory hearing loss. Overriding of the condylar segment medially may cause injury to
the inferior alveolar nerve as it enters the mandibular foramen at the lingual. The internal
maxillary artery may be damaged as it travels just medial to the neck of the condyle.

92
LATE COMPLICATIONS
Late complications of condylar fractures commonly include the following:
1. Malocclusion
2. Growth disturbances
3. Temporomandibular joint dysfunction
4. Ankylosis
Malocclusion. Malocclusion following condylar trauma may result from alterations in
the condylar “growth center” and/or union of the fracture segments in a position other than
that existing before the injury. A properly timed and supervised program of training elastics
and physiotherapy can avert significant malocclusion in the majority of cases. If a significant
malocclusion persists despite adherence to recommended guidelines, the use of judicious
occlusal equilibration, orthodontics, or orthognathic surgery may be required. Most patients
are amenable to more conservative therapy and are able to compensate for a small degree of
occlusal disharmony. In the edentulous patient, differences in the interocclusal relationship
can be compensated for during the fabrication of new prostheses.
Growth Disturbances. Several factors influence the effect of condylar fracture on the
growth of the maxillofacial skeleton, including the age of the patient, the severity of the
injury, and the period of immobilization. The limitation of normal growth is related to an
alteration in the normal condylar growth center and the tethering effect exerted by scar tissue
on the developing masticatory system.
Earlier theory described the condylar cartilage as being the primary “center” for
mandibular growth. It was believed that the carlilage cap provided the driving force for
forward and downward growth of the mandible. As discussed earlier, the functional matrix
theory has largely replaced this thinking with the concept that changes in the condylar
cartilage are secondary to downward and forward displacement of the mandible by growth of
its surrounding soft tissue envelope. Interference with the displacement of the mandible or the
apposition of bone in the region of the condyle results in disturbances in mandiblular growth,
symmetry, and function.
In any event, the potential for compensatory changes and the restitution of condylar
form are notably influenced by the age of the patient at the time of injury. The ability to

93
regenerate a morphologically and functionally normal condyle is significant until
approximately the age of 12 years. Several authors, including MacLennan and Simpson,
Blevins and Gores, Leake et al, the Chalmers J.Lyons Club, and Posnick, have reviewed the
long-term follow-up data on a large number of patients with condylar fractures. Of the
younger patients in these studies, few experienced any limitation of growth or function. As
the age of the patient increased, the ability to remodel the condyle decreased and an increase
in morphologic and functional disturbances was seen. These findings are supported by the
work of Lindahl and Hollender (1977), who studied the radiographs of 67 patients with 76
condylar fractures. The patients were divided by age into four groups: 3 to 11 years, 12 to 15
years, 16 to 19 years, and 20 years or older. In the youngest age group, 20 of 27 patients
(74%) showed complete restitution of the condyle-fossa relationship by 48 months. In the
adolescent group (12 to 19 years), substantial remodelling occurred but not to the extent seen
in the youngest group. In the adults, minimal remodelling occurred, with primarily functional
adaptation of the joint.
Experimental animal data presented by several authors support this conclusion.
Surgically induced condylar fractures in young rhesus monkeys, with medial and anterior
displacement of the fracture segments, showed that regardless of the degree of dislocation of
the fragments or the method of treatment, bony union with an upright functional condylar
process was obtained. No growth disturbance was noted in any of the animals studied.
As can be seen in the previous discussion, the ability to maintain normal condylar
position and size is important in the normal growth pattern of the mandible. Condylar fracture
in the young patient rarely alters these relationships to a significant degree, and thus growth
disturbances are also relatively uncommon. When they do occur, however, the consequences
can be devastating functionally, aesthetically, and psychologically.
If normal growth is disrupted, the affected ramus height is reduced and the unaffected
side is allowed to grow normally. This inequality results in a shortened, lower facial height
on the affected side, with an elongated inferior mandibular border and flattened facial contour
on the contralateral side. A bowing of the inferior border occurs on the fracture side, resulting
in the notable antegonial notching often seen in this situation. In addition, a number of
dentoalveolar compensations occur as the patient attempts to establish a workable occlusion.
Posterior crossbite on the fractured side is common. Contralateral hypereruption of the
posterior teeth may be seen if an open bite was present at the time of injury and was not

94
adequately corrected. This situation yields a canting of the maxillary occlusal plane. Tilting
of the dentoalveolar segments may also be seen with buccoversion of the mandibular teeth
and palatal inclination of the maxillary posterior dentition. These abnormal relationships may
cause functional disturbances as well. Additionally, as may be expected, the psychological
implications for the patient with facial asymmetry and aesthetic deformity are significant
indeed.
The formation of fibrous scar tissue in the area of temporomandibular injury may have a
tethering effect on the downward and forward displacement of the mandible during growth.
This effect can also lead to disturbance of normal growth, asymmetry, and functional
disturbances. Following injury, a properly timed and supervised program of training elastics
and physical therapy, as has been stressed previously, can decrease the formation of thick
bands and allow an increased range of motion and increased growth potential. Thus a closely
supervised follow-up regimen, especially in those younger than 12 years of age, should be
implemented following condylar fracture to maintain condylar position, ensure proper
healing, and minimize the occurrence of mandibular growth disturbances and limitation of
motion.
Temporomandibular Joint Dysfunction(Internal Derangement). A great deal of attention
has been direction toward the relationship of the meniscus and the condyle and the other
components of the TMJ in the development of internal derangement and dysfunction of the
joint. As discussed in detail by Goldman, a wide variety of injuries can result in the
development of internal derangements. Seemingly benign microtrauma and obvious
macrotrauma can lead to abnormal relationship of the components of the joint and symptoms
of pain and joint noise.
It is interesting that despite the current thinking that abnormal condyle –disk –fossa
relationships are responsible for a notable number of TMJ symptoms, a majority of patients
with condylar fracture and joint disruption are able to return to normal function with minimal
pain. Walker et al have explored this idea and suggest that if the relationship of the meniscus
is indeed important in preventing joint dysfunction, an effort should be made at the time of
open reduction of dislocated condylar fractures to repair the disk and reposition it into its
anatomically correct position. No long-term data exist, however, to support this procedure as
routine practice.

95
Internal derangement following condylar fracture may result from direct trauma to the
joint, with disturbance of the normal anatomic positioning of the bony fragments and the
meniscus. Damage to the fractured condyle may also lead to derangement of the contralateral
joint secondary to overloading of the uninjured joint, hypermobility, and eventual disk
displacement. This has been coined “condylar post fracture syndrome.”
Ankylosis. Ankylosis of the TMJ is one of the most serious complications of condylar
fracture. Trauma is the leading cause of ankylosis (31% to 98%), followed by systemic or
local infection (10% to 49%) and systemic diseases, such as rheumatoid arthritis, ankylosing
spondylitis, and psoriasis (10%). Ankylosis can be classified on the basis of degree of
limitation (partial or complete), location of the union (intracapsular versus extracapsular), and
type of tissue involved (fibrous, osseous, or fibroosseous). These factors may influence the
approach to management of the lesion. The end result is severe limitation in the range of
mandibular motion, which may interfere with speech, oral hygiene, and proper preparation of
a food bolus for digestion and maintenance of nutrition.
Factors that contribute to the formation of ankylosis include the age of the patient at the
time of injury, site and type of fracture, length of immobilization, and damage to the
meniscus.
A greater predisposition toward ankylosis of the TMJ exists in younger individuals,
especially those injured before the age of 10 years. Children have a greater propensity toward
falls, with forces transmitted to the condyles along their axes. This tendency, combined with
the relative thickness of the condylar neck and thin cortical bone at the condylar head, results
in a bursting and comminution of the condylar head. In the adult, the thicker cortical bone
and thin condylar neck make the neck the more likely site of fracture. The condylar head in
the child is highly vascular and contains an abundance of osteogenic cells. Thus the
shattering of the head within the joint capsule is followed by hemarthrosis and the release of
bone fragments rich in osteogenic potential, which greatly increases the risk of ankylosis.
This physiologic setting has been difficult to produce experimentally, however. Surgical
induction of intracapsular fractures with extended immobilization in the TMJ of primates, the
injection of autologous blood into the knee joints of dogs, and surgical comminution of the
condylar head in monkeys all failed to produce ankylosis. Therefore although the factors
mentioned earlier may play contributory roles in the development of ankylosis, none appears
to be singularly causative.

96
The site and type of fracture may also play a role in ankylosis development.
Intracapsular fractures have a higher incidence of ankylosis than those occurring outside the
joint capsule. This tendency could be explained in part by the resulting close proximity of the
bony fragments when the fracture occurs within the capsule. Also hemarthrosis development
following intracapsular fracture may lead to inflammatory changes, adhesions, and eventual
fibrous and bony union of the joint. Again, animal data do not seem to correlate when these
variables are examined alone. One study examined the arthroscopic findings following
condylar fracture and suggested that routine examination of the joint, combined with the
obligatory joint irrigation, may evacuate much of the hemorrhage, products of clot
breakdown, and inflammatory mediators, which may contribute to the formation of ankylosis.
Further investigation into this potentially beneficial aspect of treatment requires evaluation
before the procedure becomes routine practice.
Finally the meniscus may play a central role in the prevention of ankylosis. Some
authors think that close approximation of the condylar or ramus stump to the glenoid fossa is
requisite for ankylosis development. If properly positioned within the joint space, the
meniscus would act as a barrier to this approximation and prevent union of the stump and the
fossa.
This hypothesis is supported in theory by the fact that in most cases of ankylosis that are
surgically repaired, no meniscus is found in the area of union, although an intact disk may be
displaced to the periphery of the bony or fibrous union.
A more controversial parameter in ankylosis development is the length of
immobilization. Animal studies have not been able to consistently reproduce ankylosis with
periods of immobilization far in excess of those typically used in the management of condylar
fractures. It has, however, been shown that a shorter period of fixation than previously used
has no detrimental effect on healing.
Clinically the unilaterally ankylosed joint shows deviation toward the affected side during
function. The maximum interincisal distance is greatly reduced, and this reduction is usually
progressive over a number of months or years following injury. Bilateral cases may display
an anterior open bite, and the range of opening is almost nil. Depending on the age of the
patient at the time of injury, a notable disturbance in growth and symmetry of the mandible
may be seen. The affected side is foreshortened, and the chin is usually deviated toward the
abnormal side. As mentioned previously, the normally developed inferior border appears

97
flattened, and the ankylosed side shows an exaggerated antegonial notch. The developing
dentition is able to compensate for the underdevelopment of the ankylosed joint with the
development of a posterior crossbite on the affected side and angulation of the long axes of
the anterior teeth.
Before any treatment is rendered, and even before treatment planning, adequate
radiographic evaluation –including plain films and CT scan –should be obtained. This
information allows the surgeon to determine the type of tissue involved and the extent of
pathologic tissue proliferation and to evaluate the pertinent local anatomy. Only after this
preliminary planning should a surgical plan be developed.
Repair of the ankylosed joint has been approached by a number of techniques, including
attempts to release the ankylosis and still maintain the joint architecture, gap arthroplasty,
resection of the diseased segment with and without interpositional grafts, and total joint
prostheses. None of the methods have met with overwhelming success, and reankylosis is not
uncommon. Kaban et al have presented an approach to management of the ankylosed joint
that includes complete resection of the abnormal bony segments with aggressive
debridement, especially at the anteromedial aspect of the fossa, where remnants are typically
missed. This procedure is followed by ipsilateral and possibly contralateral coronoidectomy,
depending on the degree of mobility attained after resection. The joint is reconstructed with
autologous costochondral graft rigidly fixed to the lateral ramus and the interposition
placement of a temporal muscle flap. Intermaxillary fixation is used for a short period,
followed by a closely monitored and aggressive regimen of physiotherapy over a 1-year
period. Retrospective examination showed that the asymmetries treated had remained
corrected throughout the follow-up period, and at the 1-year evaluation. The maximum
opening had increased an average of 292% more than preoperative values (16.5mm versus
37.5 mm).

98
CONCLUSION
Click herewww.faceart-clinic.com
Fractures of the mandibular condyles constitute a notable portion of mandibular fractures.
A number of clinical signs and symptoms should alert the clinician to the possibility of such

99
injuries. The use of plain radiographs in multiple views usually discloses most condylar
fractures, although the advent of the CT scan has made a more definitive and detailed
evaluation and description of these injuries possible. A number of classification systems have
been devised to group condylar fractures, but in most instances these systems have little
utility in the clinical management of these injuries.
With regard to treatment, most of the published data before the advent of rigid fixation
on both animals and humans support the use of conservative therapy for the management of
condylar fractures except in a specific subset of fractures in which movement is limited,
adequate occlusion cannot be obtained, or intermaxillary fixation is contraindicated.
However, recently there has been a resurgence in literature supporting open reduction and
internal fixation of condylar fractures, citing improved condylar stability and occlusal results,
earlier return of joint function, and improved cosmesis. Knowledge of regional anatomy and
improved techniques for surgical access to the TMJ have greatly reduced complication rates.
There are a number of surgical approaches to the condylar fracture and an equal number of
different methods of reduction and fixation of the fracture segments. The simplest method
with the least complications based on the specifics of the fracture (location, type of fracture,
displacement of segments, age of the patients, and concomitant medical conditions) should be
used. Children present a unique group with a remarkable potential for healing and
regeneration of a functional and morphologically “normal” condyle.
In general complications following condylar trauma are uncommon. Perhaps the most
serious are ankylosis and growth disturbance. Other complications include malocclusion,
damage to neurovascular structures, and TMJ dysfunction.
Little doubt exists that the subject of temporomandibular injuries and their
management will continue to spark controversy in the oral and maxillofacial surgery
community. Many new ideas and older ones require further investigation and clinical
research to continually advance our understanding of this complex and relevant area.

100
BIBLIOGRAPHY
1. Kreutziger K:Surgery of the temporomandibular joint. I: surgical anatomy and
surgical incisions, Oral Surg Oral Med Oral Pathol 58:637, 1984.
2. Krenkel C: Biomechanics and osteosynthesis of condylar neck fractures of the
mandible, Chicago, 1994, Quintessence.

101
3. Al-Kayat A, Bramley P:A modified pre-auricular approach to the temporomandibular
joint and malar arch, Br J Oral Maxillofac Surg 17:91, 1997.
4. Dingman R, Grabb W:Surgical anatomy of the mandibular ramus of the facial nerve
based on the dissection of 100 facial halves, Plast ReconstrSurg 29:266, 1962.
5. Chalmers J:Fractures involoving the mandibular condyle: a post-treatment survey of
120 cases, J oral surg 5:1947,1947
6. Kromer H: The closed and open reduction of condylar fractures, Dent Rec 569,1953.
7. Ekholm A : A clinical, pantomographic and electromyographic study, Suomen
Hammaslaakeriseuran Toimituksia 579,1961.
8. Schuchardt K, Metz H:Injuries of the facial skeleton, Mod Trends Plast Surg 2:62,
1966.
9. Rowe N Killey H: Fractures of the facial skeleton, ed 2, Edinburgh, 1968, Churchhill
Livingstone.
10. Tasanin A, Lamberg MA: transosseous wiring in the treatment of condylar fractures
of the mandible, J Maxillofac Surg 4:200, 1976.
11. Larsen O, Nielson A: Mandibular fractures. I: an analysis of their etiology and
location in 286 patients, Scand J Plast Surg 10:213, 1976.
12. Van Hoof R, Merkx C, Stekelenburg E: The different patterns of fractures of the
facial skeleton in four European countries, Int J Oral Surg 6:3, 1977.
13. Olson R et al: Fractures of the mandible: a review of 580 cases, J Oral Maxillofac
Surg 40:1, 1982.
14. Hill C et al: Facial fractures: the results of a prospective four-year study, J Maxillofac
Surg 12:267, 1984.
15. Andersson L et al : Jaw fractures in the county of Stockholm(1978-1980). I:general
survey, Int J Oral Surg 13:194,1984.
16. Ellis EI,Moos K, El-Attar A: Ten years of mandibular fractures: an analysis of 2137
cases, J Oral Surg 59:120, 1985.
17. Haug R, Prather J, Indresano A: An epidemiologic survey of facial fractures and
concomitant injuries, J Oral Maxillofac Surg 48:926, 1990.
18. Silvennnoinen U et al: Different patterns of condylar fractures: an analysis of 382
patients in a 3 year period, J Oral Maxillofac Surg 50:1032, 1992.
19. Marker P, Nielsen A, Bastian H:Fractures of the mandibular condyle. Part 1: patterns
of distribution of types and causes of fractures in 348 patients, Br J Oral Maxillofac
Surg 38:417-421,2000.

102
20. Haug R, Foss J: Maxillofacial injuries in the pediatric patient, Oral Surg Oral Med
Oral Pathol 90:126-134,2000.
21. Bradley PF: Injuries of the condylar and coronoid process. In Rowe NL, Williams JL,
editors: Maxillofacial injuries, Edinburgh, 1985, Churchill Livingstone.
22. James R, Fredrickson C, Kent J: Prospective study of mandibular fractures, J Oral
Surg 39:275, 1981.
23. Amaratunga Nad: The relation of age to the immobilization period required for
healing of mandibular fractures, J Oral Maxillofac Surg 45:111,1987.
24. Carroll MJ, Hill CM, Mason DA: Facial fractures in children, Br Dent J 163:23, 1987.
25. Sheikh Z, Worrall S: Epidemiology of facial trauma in a sample of patients aged 1-18
years, Injury 33:669-671, 2002.
26. Posnick J: Management of facial fractures in children and adolescents, Ann Plast Surg
33:442-457,1994.
27. Boyne PJ: osseous repair and mandibular growth after subcondylar fractures, J Oral
Surg 25:300, 1967.
28. Ellis Er, Schneiderman E, Carlson D: Growth of the mandible after replacement of the
mandibular condyle: an experimental investigation in Macaca mulatta, J Oral
Maxillofac Surg 60:1461-1470,2002.
29. Goldman J: Temporomandibular disorder: diagnosis and treatment. In Kaplan AS,
Assael LA, editors: Philadelphia, 1991, WB Saunders.
30. Wilkes CH: Surgical treatment of internal derangements of the temporomandibular
joint. A long term study Arch Otolaryngol 117(1):64-72,1991.
31. Lindahl L: Condylar fractures of the mandible. I: classification and relation to age,
occlusion, and concomitant injuries of the teeth and teeth-supporting structures, and
fractures of the mandibular body, Int J Oral Surg 6:12,1977.
32. Fonseca RJ: Experimental study on fractures of the mandibular condylar process, Int J
Oral Surg 3:89,1974.
33. MacLennan W: Fractures of the mandibular condylar process, Br J Oral Surg
7:31,1969.
34. Lindahl L:Condylar fractures of the mandible. III: positional changes of the chin, Int J
Oral Surg 6:166,1977.
35. Archer W.H. : Oral and Maxillofacial surgery 5th edition, 1975.
36. Becker A.B. : Open reduction of condylar fractures. report of cases O.S., O.M, O.P.,
Vol. 5:1282, 1952.

103
37. Kromer H. : Closed and open reduction of condylar fractures, Dent. Records,
Vol.13(1953), pg.569.
38. Kruger : Text Book of oral surgery, C.V.Mosby & Co. 1968.
39. Khosla V.M & Boren W.: Mandibular fracture in children and their management,
JOS. Vol. 29,1971.

104
Thank youClick here
www.faceart-clinic.com