Embed Size (px)
Citation preview

Common FracturesDr Nicola Walsh
Orthopaedic Registrar

ED Senior says ‘Just ring ortho....’
Common things are Common!TraumaPaediatric fracturesUpper LimbLower limbPelvisSpine
What XR’s do I need?Trauma Series2 views of each fractureJoint above and below – why?Special views e.g. scaphoidCTMRI
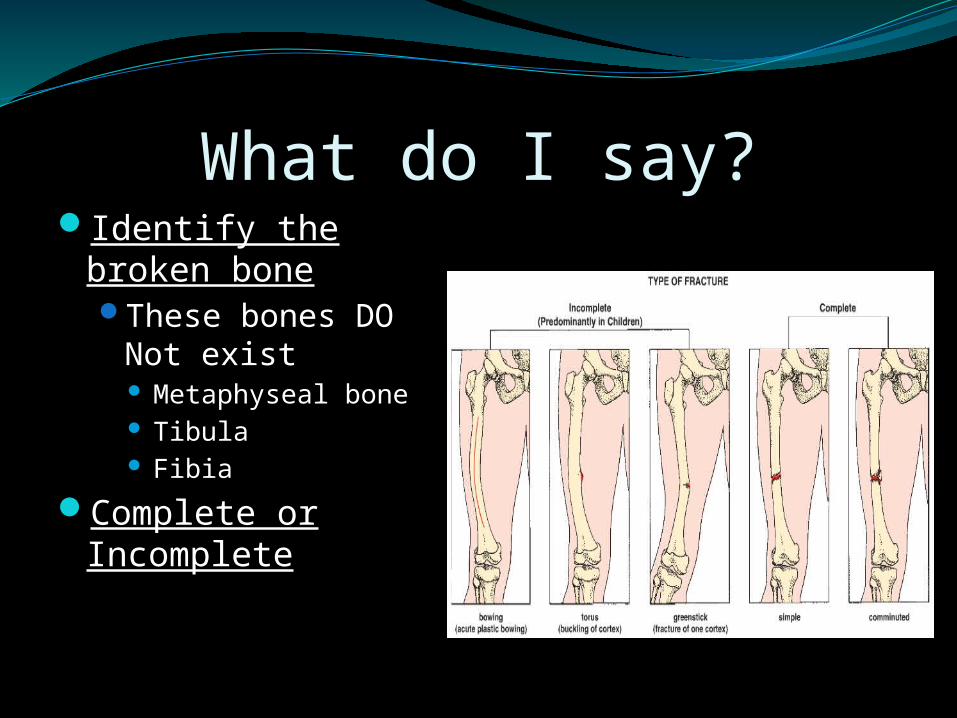
What do I say?Identify the broken
boneThese bones DO Not
exist Metaphyseal bone Tibula Fibia
Complete or Incomplete

Anatomical location in boneProximal, middle or
distal thirdExtent of fracture
Intraarticularsupracondylar

Fragment Alignment
displacement
angulation
rotation
shortening
distraction
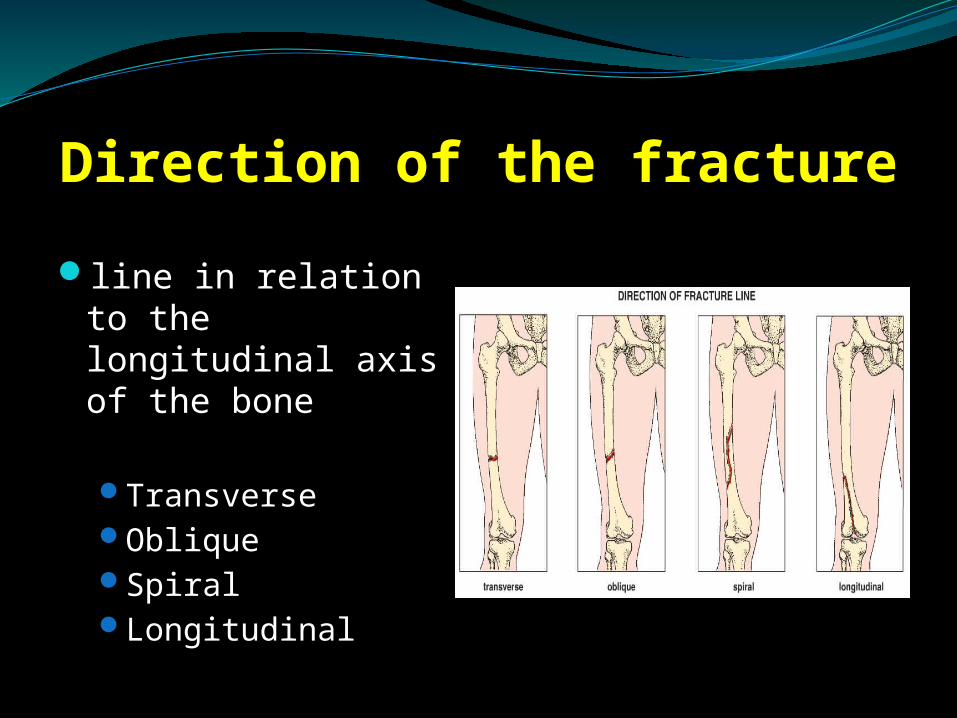
Direction of the fracture
line in relation to the longitudinal axis of the bone
TransverseObliqueSpiralLongitudinal

Fracture PatternsLateral bending produces a transverse
fracture pattern while torsional or twisting forces produce oblique or spiral fracture patterns.
Understanding these patterns and the inherent stability or instability of each type is important in choosing the most appropriate method of fixation
Figure from: Schatzker J, Tile M: The Rationale of Operative Fracture Care. Springer-Verlag, 1987.

Special Fractures
Fracture secondary toAbnormal stress
in Normal bone
Normal stress in abnormal bone ie weakened by a pathological process

Periosteal and Endosteal Reaction
Fracture line may not be visible
Periosteal reaction may be first sign
Delayed diagnosisStress fracturesPaediatric
‘Toddler’s’ fracture
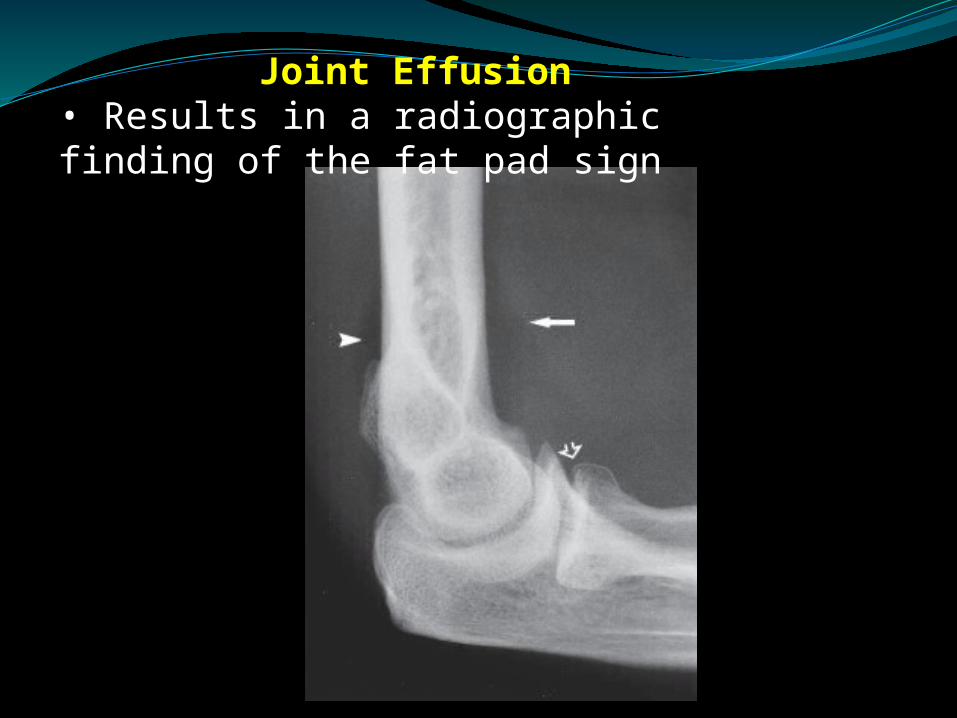
Joint Effusion• Results in a radiographic finding of the fat pad sign

Subtle Intraarticular fracture

Paediatric FracturesSalter Harris ClassificationForearmWristFemurAnkle

Salter Harris Classification
S = SlipA = AboveL = beLowT = Through

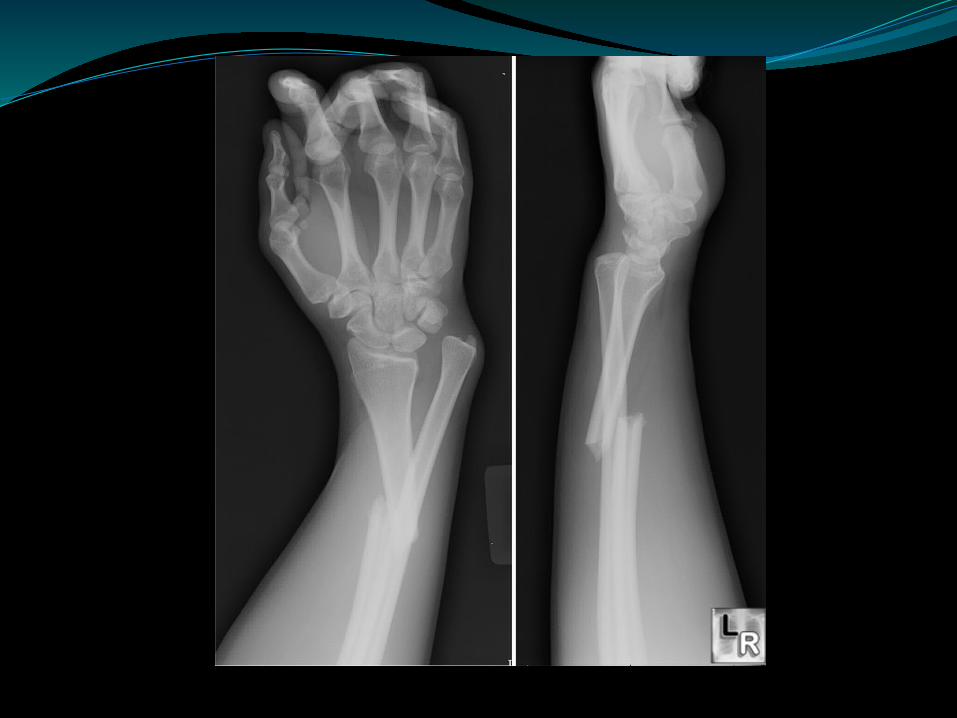
WristHistory of fall onto outstretched handSwollen, tender, deformedCheck Neurovascular statusCheck hand and elbowAP and Lateral Xrays of wrist and forearm to
elbowCan accept up to 30 degrees if >5 years growth
remaining, 5 degrees less for each year.Cannot accept rotational deformityMay need CR +/- K wiresWill need POP

Forearm FracturesFall onto hand or forearmTrampolines/Monkey bars/Slippery dipInclude wrist and elbow on XraysExamine the humerusNV statusSplintAccept 10 degrees of angulation < 10 years
but don’t accept a crooked arm.No rotational deformity



Monteggia FracturesFracture of the ulna with radial head dislocationCheck Radial nerve (PIN)Check rest of neurovascular statusIs the skin at risk?Do not accept xrays which don’t show the elbow and wristGaleazzi fracture (# Radius with distal ulna dislocation)


TreatmentSplintAnalgesiaKeep fastedCall ortho reg
Supracondylar fractures HumerusFall, Occ twisting injuryObvious deformityCheck NV Status!!!!!!!!!!! 10-20% injuryHand Cold?Open or closed?Splint/NBM/analgesiaCall ortho reg


Supracondylar fracturesRelative orthopaedic emergencyGartland Classification:
I: Non-displaced, crack in anterior cortex, cast 3/52
II: Displaced but hinged posteriorly. Most get CRIII: Completely displaced, all get CR +/- Wires
Radial pulse, vascular status of handSplint/NBM/Call ortho Reg/send Xrays to
theatre.Post Fat pad sign.......70% have a fracture
ClavicleUsually sling and ortho Follow upCheck sternoclavicular joint for dislocation

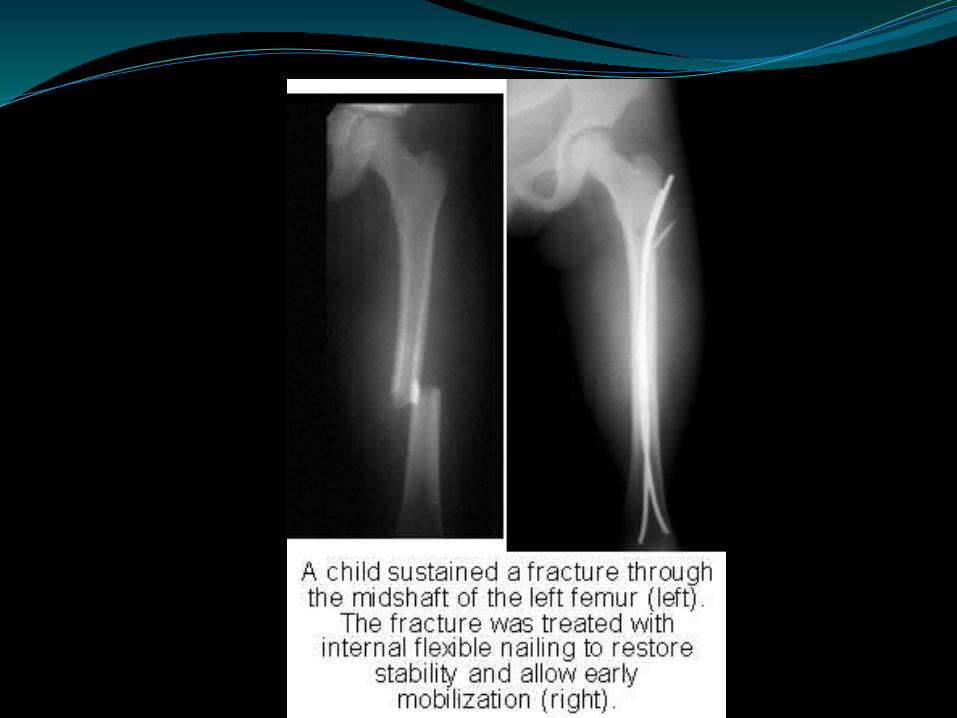
Femoral fractures in childrenFemoral neck – orthopaedic emergency.....call
regFemoral shaft – NV status
Consider abuse if child not walkingUsually some form of tractionGive analgesia and splintDistal femoral fractures – Usually SH IISplint and call ortho

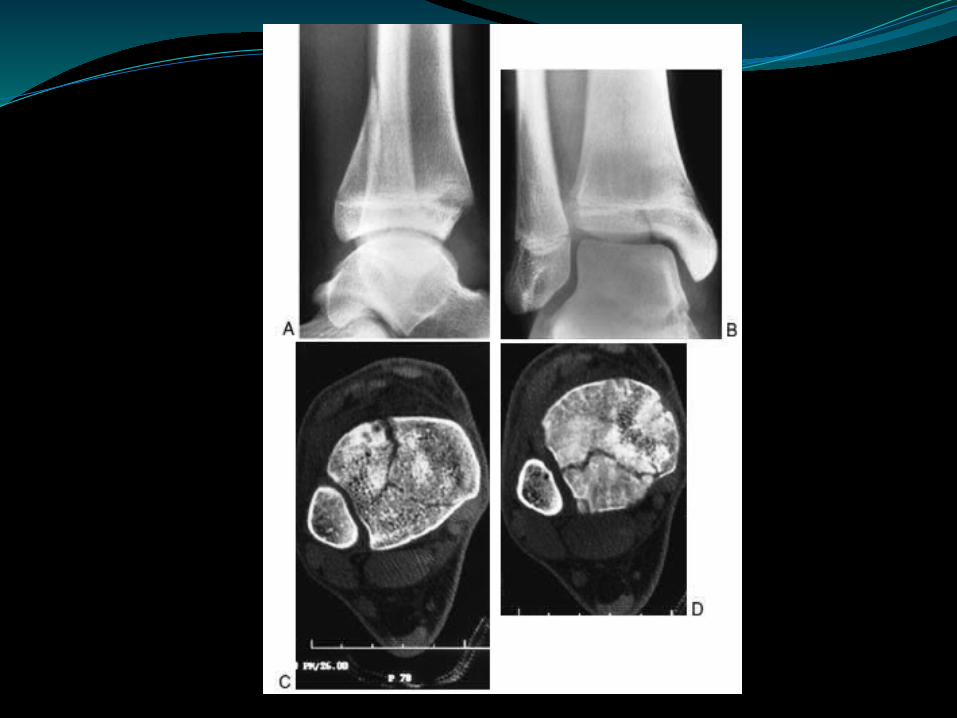
Ankle FracturesInversion injuryCheck NV statusSwollen, deformed ankleFeel for tenderness medially and laterallyNeed AP, Lateral, MORTISE views of ankle and
tibia/fibula xraysBackslab/elevate/analgesia/NBM


Adults – Distal radius FracturesFall onto outstretched handDeformityNV statusCheck elbow and humerusSplintNot every fracture is a Colles fracture!!!!!
Colles FractureElderly, osteoporotic fractureExtra-articularDorsal tiltRadial deviationRadial shortening


Distal radius fractures – tell usAgeMechanism of injuryOpen/closedNeurovascular statusIntra/extra articularDorsal/volar displacementUlnar dislocated?Any other injury?







Ankle FracturesTwisting injury/FallSwollen, deformed, unable to weight bearAP, Lateral, Mortise views and Tib/fib viewsElevate/splint/NBM
Weber ClassificationA – Below syndesmosis, usually backslab,
NWB 6/52B- Level of syndesmosis. IS there medial
tenderness? Is there talar shift? Is there a medial mallelous #?
C – Above syndesmosis. Usually talar shift and medial tenderness
If isolated Medial malleolus fracture – check for fibular tenderness and xray whole of fibula (Maisonneurve fracture)




FRACTURES OF THE FEMORAL NECK
Intracapsular vs ExtracapsularBlood supplyDifferent treatmentYoung patients <60 years + intracapsular =
orthopaedic emergencyGarden classification for intracapsularExtracapsular comprise basicervical,
intertrochanteric (pertrochanteric), subtrochanteric
Intracapsular FracturesFemoral neck commonest site of fractures in
the elderlyCaucasian women in 70’s and 80’sAssociated with osteoporosis, osteomalacia,
diabetes, CVA (disuse), Alcoholism, chronic debilitating disorders
Weak muscles and increased tendency to fall

Blood supply to the femoral headA) Intramedullary vessels in the femoral neck
- always interrupted by the fractureB) Ascending cervical branches of the medial
and lateral circumflex anastomosis - may be kinked or torn if the fracture is displaced
C) Vessels of the ligamentum teres - meagre, 20% non-existent

Poor capacity for healing 1) Tearing of the capsular vessels deprives
the head of its main blood supply2) Intraarticular bone has a flimsy
periosteum and no contact with soft tissues which could promote callus formation
3) Synovial fluid prevents clotting of fracture haematoma


Garden Classification1. Nondisplaced
a) Incomplete Valgus Impactedb) Complete Fracture
2. Displaceda) Displacement < 50%b) Severely displaced

Clinical FeaturesHistory of a fall followed by pain in the hipIf displaced, Patient lies with the affected
limb shortened and in external rotationImpacted fracture, patient may still walkMentally handicapped patients may not
complain at all
Young Patient <50yearsDisplaced fracture is surgical emergencyAnatomic reduction essentialOpen reduction necessary if closed reduction
not possibleInternal fixation with cancellous screwsIncreased risk of osteonecrosis and nonunion
Older Patient >50yearsNondisplaced fracture - internal fixationDisplaced fracture - internal fixation vs
prosthetic replacement is controversialDecreased perioperative morbidity but
increased risk of secondary surgery with internal fixation
Prosthetic replacement in debilitated patient
XRAYIs there a fracture?Is it displaced?Bony outlines and trabecular lines in the
femoral head and supra-acetabular part of the pelvis
Impacted or undisplaced fractures do well after internal fixation, displaced fractures have a high rate of nonunion and osteonecrosis
Diagnosis1. Stress fractures, elderly patient with
unexplained pain in the hip should be treated as a fracture until proven otherwise. Xray may be normal but bone scan or CT will show #
2. Undisplaced fractures, impacted fractures may be difficult to see on Xray
3. Painless # in bed-ridden patients4. Multiple #’s - shaft# may have a NOF also

TreatmentBased on physiological age of patient and
degree of displacementFix undisplaced fractures to prevent
displacement.Parallel screws or sliding hip screw with anti-
rotation screwProsthetic replacement - Hemiarthroplasty vs
THR
TreatmentPain ReliefTractionFemoral Nerve blockOperation
Displaced # will not unite without OTImpacted # may unite but risk of displacement6-8 weeks in bed in traction unacceptable
alternative

Complications1. Osteonecrosis
occurs in 10 - 45%Increased risk with displacement and time to
reductionBlood supply of Femoral head
Complications2. Nonunion
a) Young patient with no osteonecrosis or < 50% head involvement
ComplicationsMortality is 20% after 2-4months, 50% at 1
yearDVTPEPneumoniaBed soresDisorders present before # which lead to
death in a substantial proportion of cases
ComplicationsAmong survivors over 80 years less than half
resume independent walkingAVN 10% undisplaced, 30% displacedNonunion 30% higher in displaced #Osteoarthritis

Intertrochanteric FracturesExtracapsularElderly osteoporotic patientsUnite easilySeldom cause AVN
Pathological anatomyStable and unstable fracture typesUnstable - poor contact between the fracture
fragments or weight-bearing forces tend to displace the fragments further

Clinical FeaturesOld or Unfit patientUnable to stand following a fallLeg shorter and more externally rotatedPatient unable to lift the leg
XRayCrack along intertrochanteric lineUsually displacedIf lesser trochanter separated and medial
cortex shattered weight bearing should be delayed
TreatmentEarly fixation - to achieve best possible
reduction and get the patient up and walking asap.
Day 1 exercises, Patient up and weight-bearing asap
DHS95 degree or intramedullary device with
reverse oblique type.

ComplicationsEarly - as in subcapital #Late - Failed fixation - screws may cut out of
osteoporotic bone, delayed union implant may break
Malunion - varus and ER deformities common. Rarely interfere with function
Non union - seldom fail to unite. If healing delayed >6months # unlikely to heal.
Pathological #Metastatic disease or myelomausually terminally illFracture fixation to ensure an adequate
quality of life for their remaining years
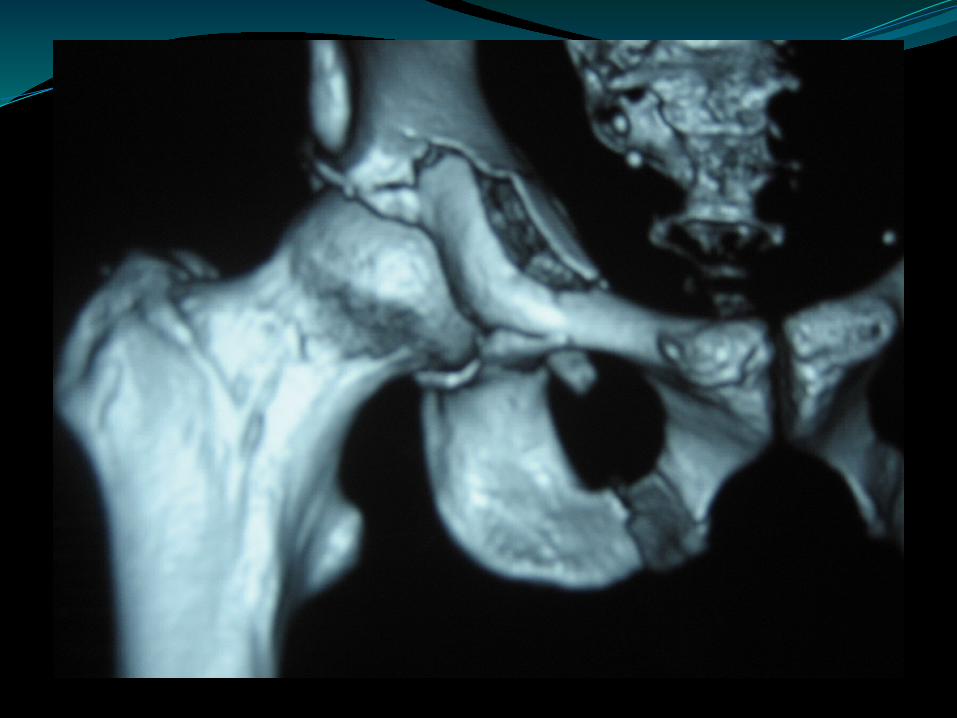
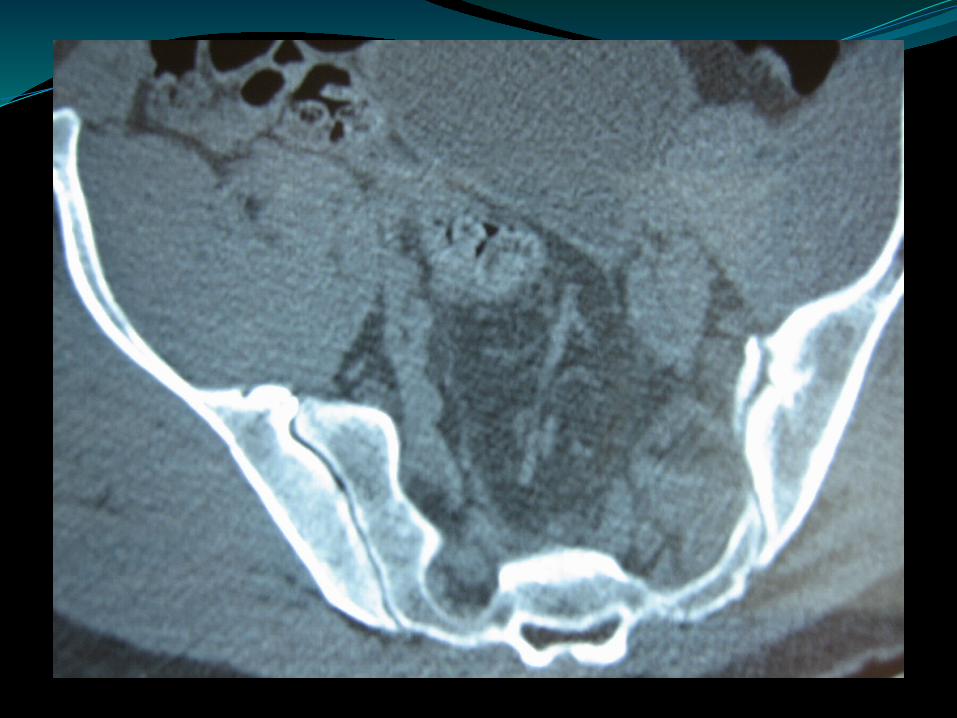
Pelvic/acetabular fracturesElderly – can be expected after a fallUsually non-operative treatmentYoung patient......NOT WITHOUT MAJOR
TRAUMAPlease assess
ATLS Incl trauma series (C spine/CXR/Pelvis)Full spine examination including PRXrays and CT scanIDCXmatch


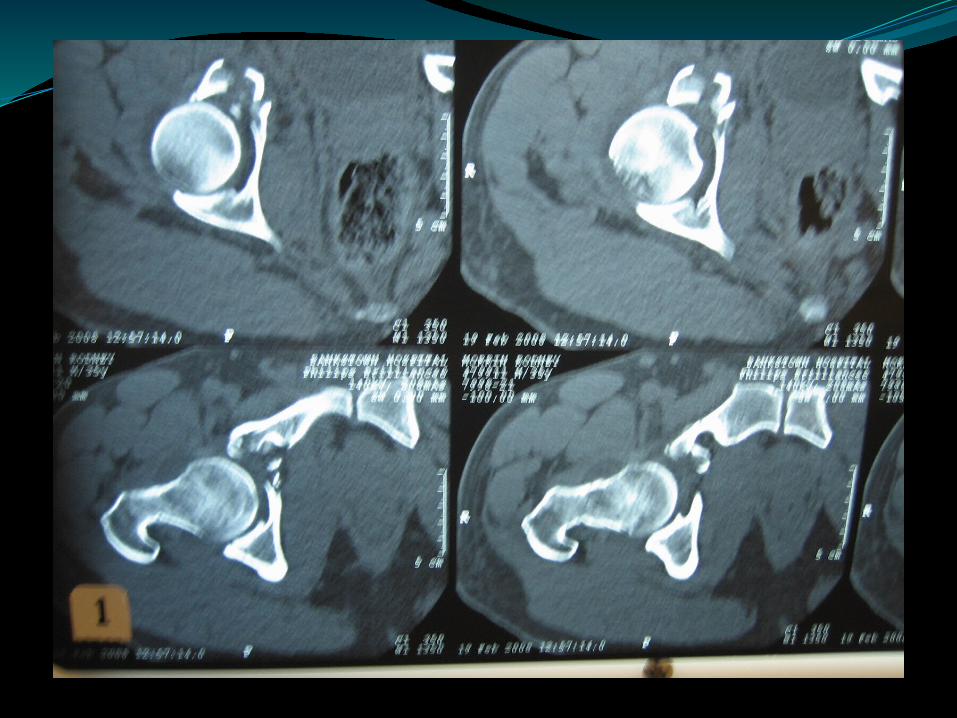


















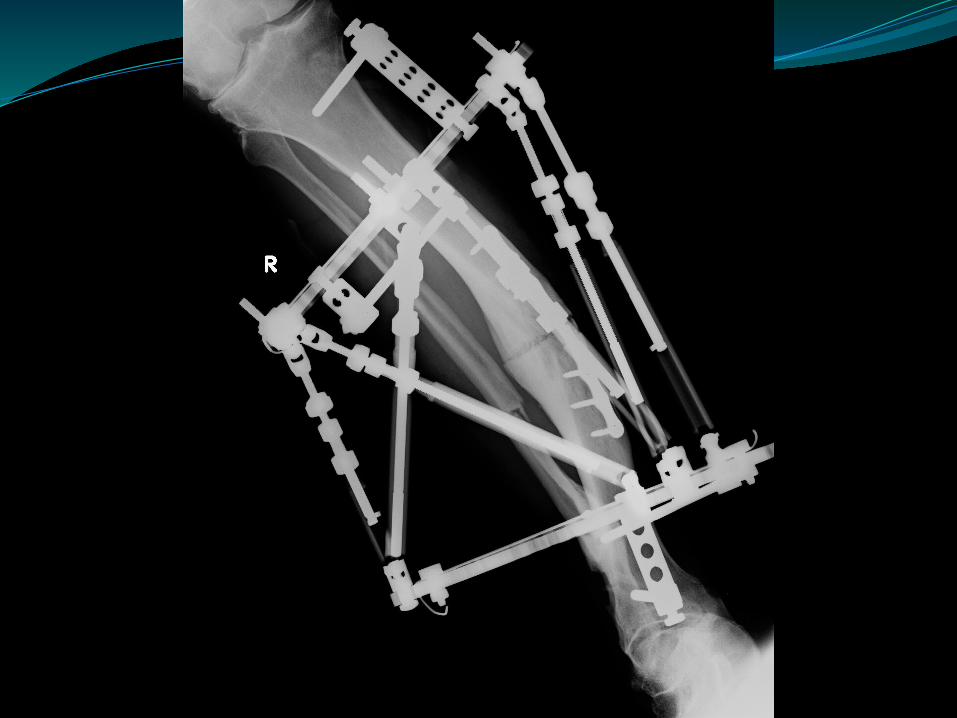

TF
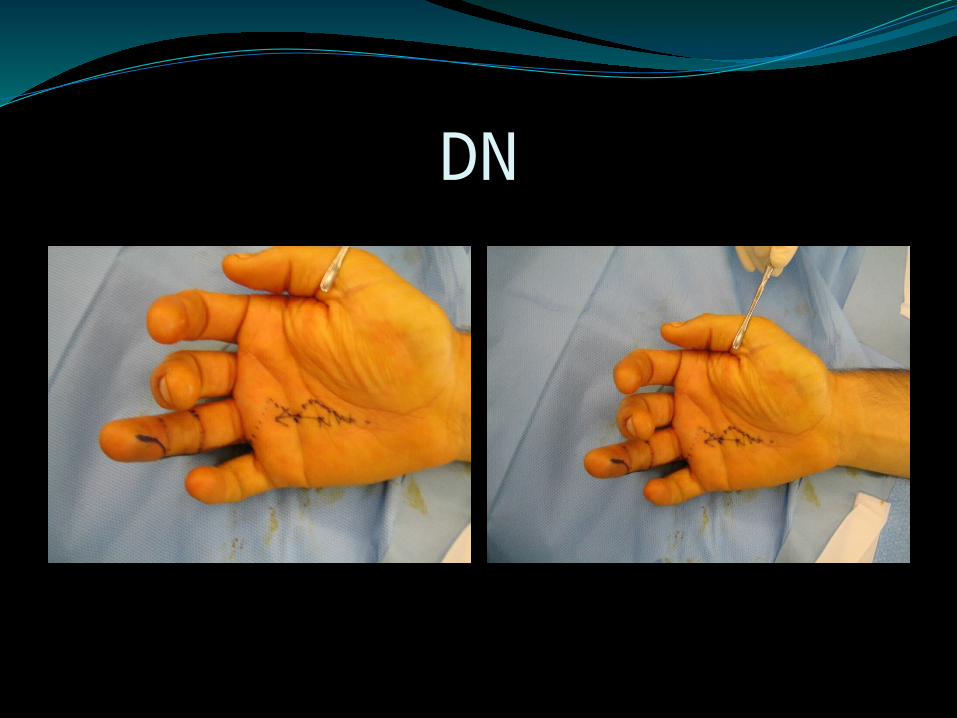
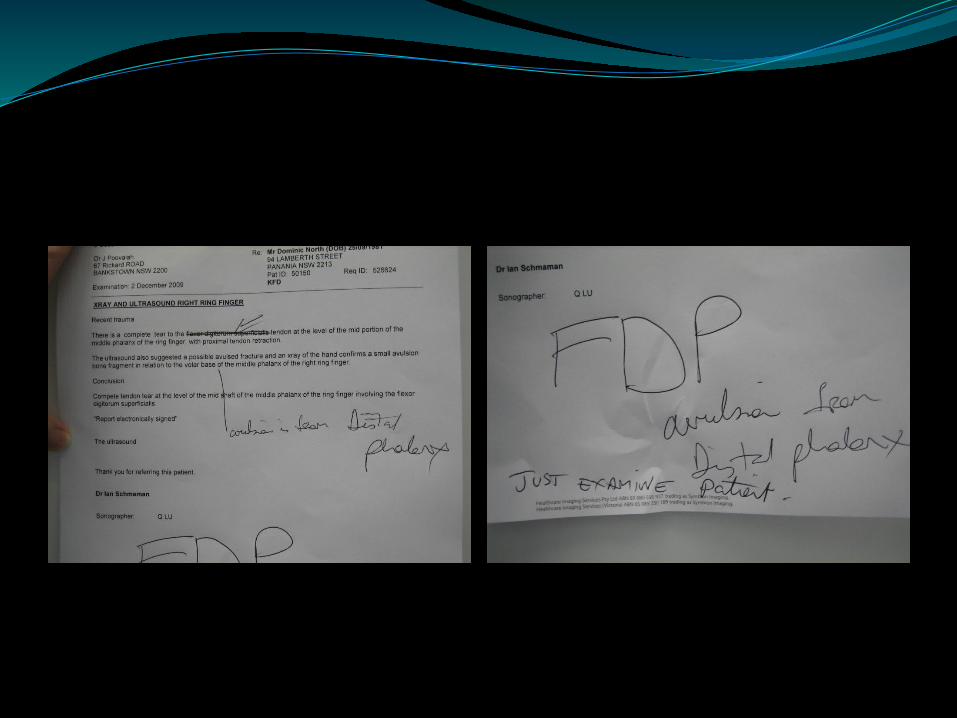
DN

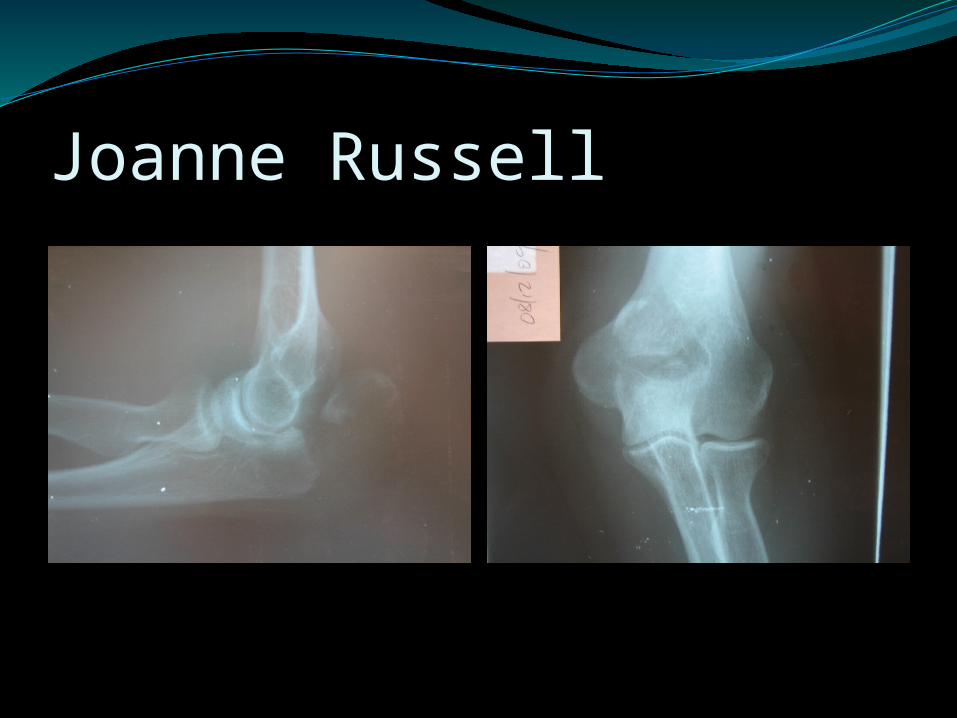
Joanne Russell

Mrs GC, 65y female (AL)Tripped at family party, Left Hip pain
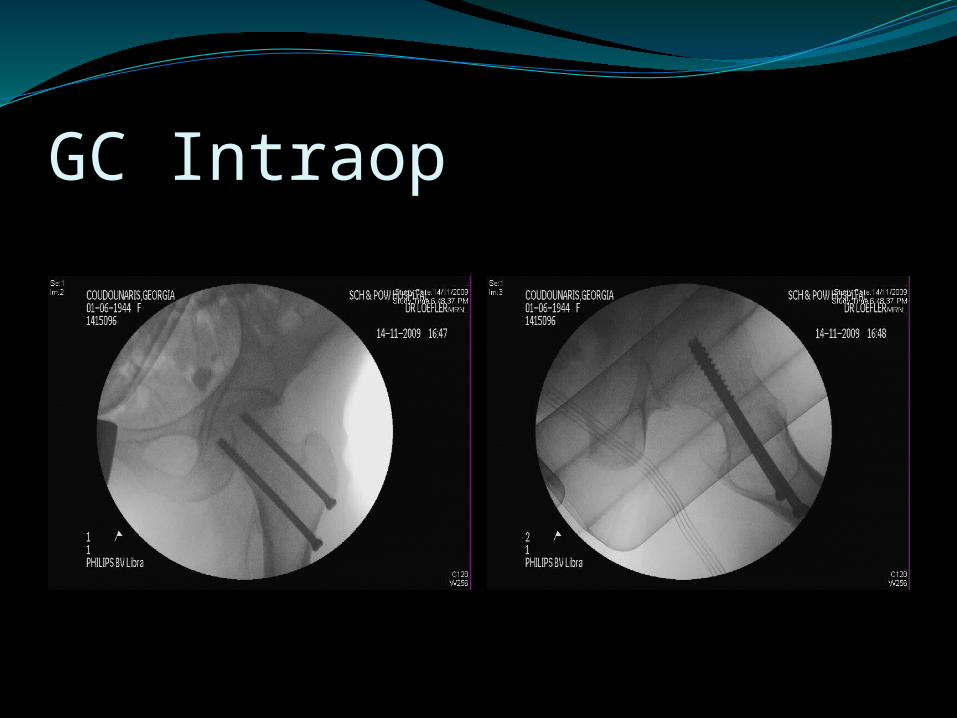
GC Intraop

Mr DC, 53y male (AL)Fall off chair while changing leg dressings, L Hip pain, Chronic infected venous ulcers, ?intellectual impairment
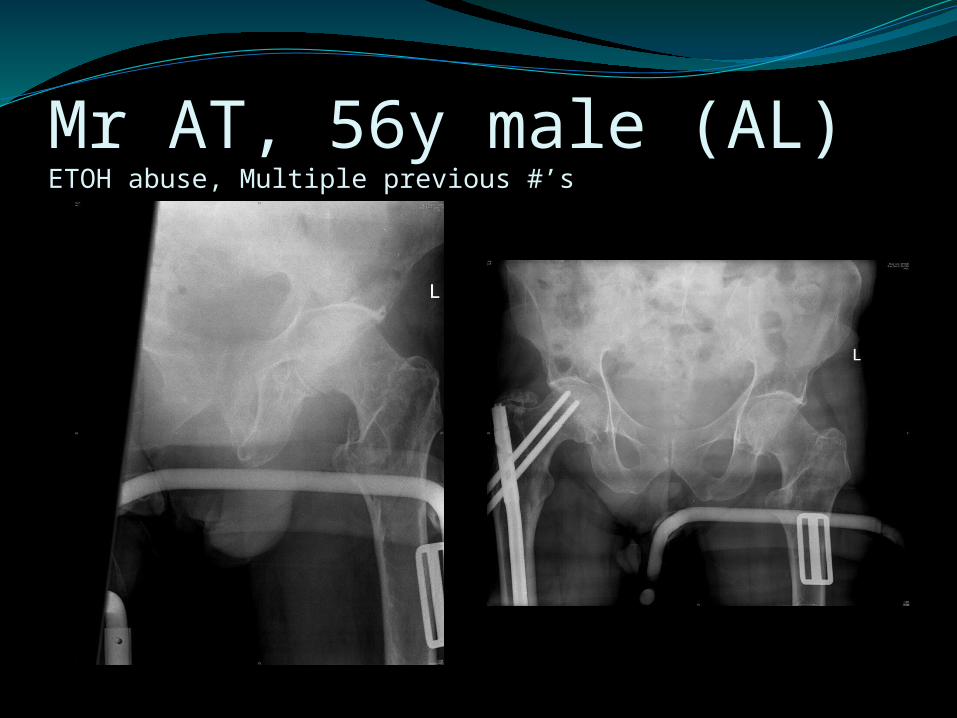
Mr AT, 56y male (AL)ETOH abuse, Multiple previous #’s
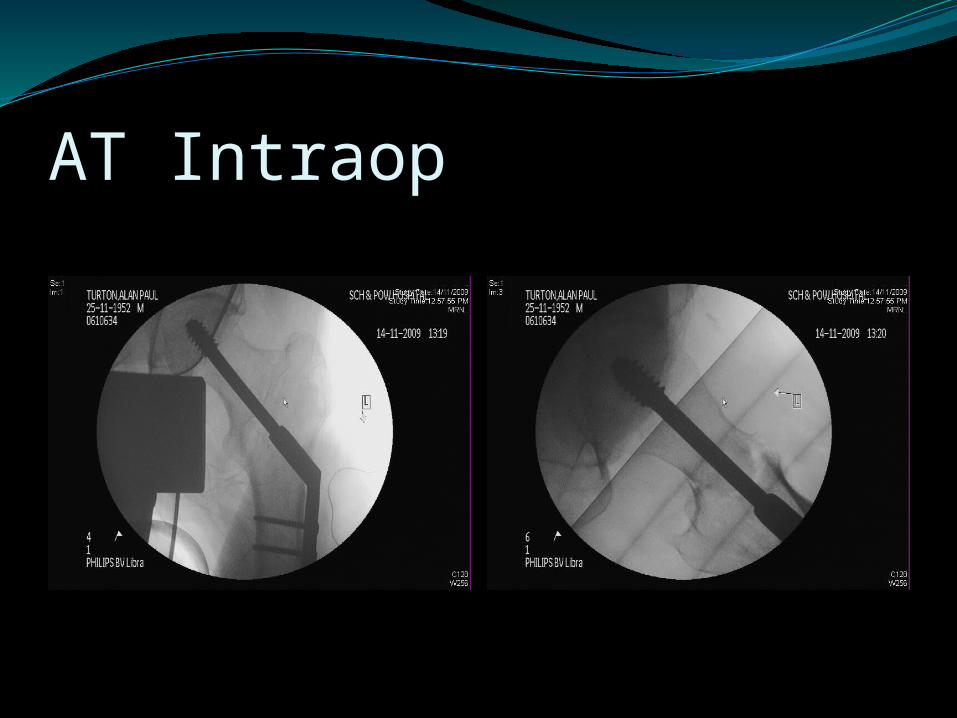
AT Intraop
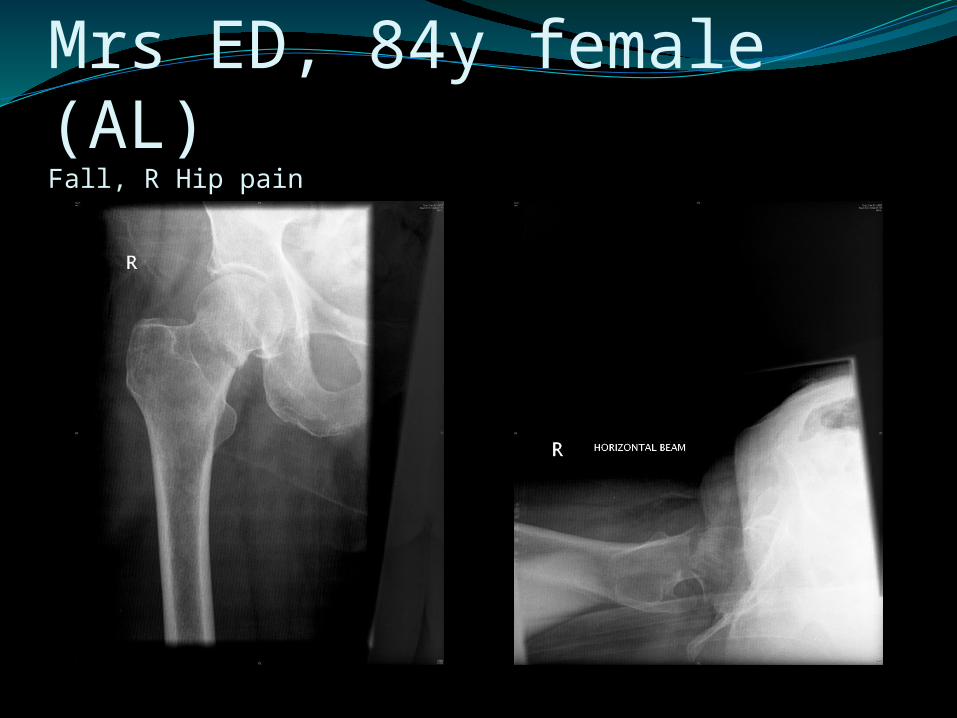
Mrs ED, 84y female (AL)Fall, R Hip pain

ED post op

Mrs MT, 45y female (AL)Fall, CR in ED
Mrs MT 45y female (AL)

Call us for
Most fracturesIf you are concerned or unsurePlease remember – our pagers and phones
are not answered in theatre Same for consults
Wake us up for
Remember we are on call for emergenciesCompartment syndromeOpen fracturesPelvic/acetabular fractures in YOUNG peopleNeurovascular compromise