Embed Size (px)
Citation preview

Colon Cancer UpdatesData from ASCO GI - 2016
Mohamed Abdulla M.D.Prof. of Clinical Oncology
Cairo University
MERCK – Symposium NEMROCK 24/04/2016

Adopted from Keynote Presentation by
David Cunningham ASCO GI 2016

Member of Advisory Board, Consultant, and Speaker for:• Amgen, Astellas, AstraZeneca, Hoffman la Roche, Janssen Cilag,
Merck Serono, Novartis, Pfizer, Mundipharma• The content of this presentation does not relate to any product of a
commercial interest
Speaker Disclosures:

Basic Facts:
• 2nd & 3rd most common cancer in females & males.• 1.4 million new case and 694000 deaths.• Males > Females.• Lowest rates in Africa & South Central Asia.• Low SES 30% increased risk.• Rising incidence < 50 years Left sided colon &
rectal, symptomatic & advanced Poor outcome.• Sporadic > Hereditary.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin 2016; 66:7. Ahnen DJ, Wade SW, Jones WF, et al. The increasing incidence of young-onset colorectal cancer: a call to action. Mayo Clin Proc 2014; 89:216.

Aspirin Colon Cancer Prevention:
• Aspirin reduces adenoma and CRC in General Population and HNPCC.
• Prevents recurrence in mutated PIK3CA patients.
Liao et al, n engl j med 367;17 nejm.org october 25, 2012

Adjuvant Chemotherapy for Stage III Colon Cancer

Adjuvant Chemotherapy for Stage II Colorectal Cancer

Assessing risk/ benefit in stage II patients

Follow up for stage II/III disease following curative treatment

Systemic Therapy for Advanced Disease:
• No predictive biomarker for chemotherapy.• Monotherapy for less fit/elderly patients.• Doublets & Triplets for higher response rates.• FOLFOX, CAPEOX, FOLFIRI Similar Efficacy.• All RAS Wild Tumors (50%) benefit from EGFR inhibition. • No biomarker to select for inhibition of angiogenesis.• Triplets may be the best option for BRAF mutated tumors.• Duration of therapy is usually 6 months or induction for 3-4
months followed by maintenance or de-escalation of doses.• Maximum Exposure or Sequence of Administration?

Choice of Systemic Therapy:
5-Fu/LV
Capecitabine
OxaliplatinIrinotecan
Bevacizumab
CetuximabPanitumumab
AfliberceptRegrafinib
TAS 102
Survival Improvement
Treatment Lines &
Combinations

Daily Treatment Scenarios:
Maximum Exposure:• Advancing Cancer Chronic
Disease.• Survival All Active Agents.• Sequence isn’t important
Sequence:• Predictive Markers • Upfront Massive Attack.• Late still wining cards
• Survival Improvement is modest in 2n & 3rd Lines.• Losing an Active Agent Out of Upfront Treatment.
Khattak et al. Clinical Colorectal Cancer, Vol. 14, No. 2, 81-90 a 2015

Predictive Markers:
OPUS, COIN, CRYSTAL, PRIME, 20050181, PICCOLO, 20020408, FIRE -3, PEAK

KRAS WT: Impact of All RAS Testing:1. PFS
Sorich et al. Annals of Oncology 26: 13–21, 2015

KRAS WT: Impact of All RAS Testing:2. OAS
Sorich et al. Annals of Oncology 26: 13–21, 2015

KRAS WT: Impact of All RAS Testing:
• Panitumumab and Cetuximab are EQUIVALENT in OAS and PFS in All RAS WT.
• EUIVALENCE regardless the backbone of chemotherapy.
• Anti-EGFR mAb third-line mono- therapy was estimated to have significantly greater benefit than first-/second-line anti-EGFR mAb therapy in combination with chemotherapy with respect to PFS (P = 0.002), but not OS (P = 0.66)
Sorich et al. Annals of Oncology 26: 13–21, 2015

CRYS
TAL5
COIN
3
PRIM
E4
NO
RDIC
VII2
CO.1
79
4088
N01
471
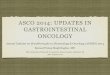
PFS for EGFR inhibitors improves across lines of therapy in KRAS wild-type patients:
Haza
rd ra
tio
1. Alberts, et al. JAMA 2012; 2. Tveit, et al. JCO 2012; 3. Maughan, et al. Lancet 2011 4. Douillard, et al. ASCO 2011; 5. Van Cutsem, et al. JCO 2011; 6. Langer, et al. ESMO 2008
7. Sobrero, et al. ASCO GI 2012; 8. Amado, et al. JCO 2008; 9. Karapetis, et al. NEJM 2008
First line Second line Salvage (single agent)
Adjuvant
1.2
1.0
0.8
0.6
0.4
0.2
0
Stud
y 18
17
EPIC
6
Albert Sobrero , WCGIC 2012

First Head-to-Head Comparisons of First-Line Bevacizumab Versus EGFR Inhibitors in KRAS WT mCRC
1. Schwartzberg LS, et al. J Clin Oncol. 2014;32(21):2240-2247. 2. Heinemann V, et al. Lancet Oncol. 2014;15(10):1065-1075. 3. Venook A, et al. J Clin Oncol. 2014;32(Suppl): Abstract LBA3.
PEAK1
Phase II
Untreated – Unresectable mCRC
N = 285
Bevacizumab + mFOLFOX6
Panitumumab + mFOLFOX6
FIRE-32
Phase IIIUntreated mCRC
N = 592
Bevacizumab + FOLFIRI
Cetuximab + FOLFIRI
CALGB-804053
Phase IIIUntreated mCRC
N = 1200
Bevacizumab + FOLFIRI or FOLFOX
Cetuximab + FOLFIRI or FOLFOX
No Hypothesis
OAS
ORR
DP

FIRE-3 Trial: FOLFIRI + Either Cetuximab or Bevacizumab in KRAS WT mCRC
Heinemann V, et al. Lancet Oncol. 2014;15(10):1065-1075.
HR 0.77P .011
Parameter Chemo + CET Chemo + Bev P
ORR (%) 62 58 .183
PFS (ms) 10 10.3 .547

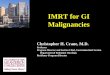
CALGB/SWOG 80405: Overall Survival
Arm N (Events)OS (m)Median
95% CI
Chemo + Cetux 578 (375) 29.9 27.0-32.9
Chemo + Bev 559 (371) 29.0 25.7-31.2
P=0.34HR 0.925 (0.78-1.09)

CALGB/SWOG 80405: Progression-Free Survival(Investigator Determined)
Arm N (Events)PFS (m)Median 95% CI
Chemo + Bev 559 (498) 10.8 9.7-11.4
Chemo + Cetux 578 (499) 10.4 9.6-11.3
P=0.55 HR 1.04 (0.91 -1.17)

100 –
90 –80 –
70 –
60 –
50 –
40 –
30 –20 –
10 –
0 –
CALGB/SWOG 80405: Quality of Life and Symptoms
Venook A, et al. J Clin Oncol. 2014;32(Suppl): Abstract LBA3.
Baseline Week 6 Month 3 Month 6 Month 9
Scor
e(0
-100
sca
le; h
ighe
r sco
res
repr
esen
t be
tter Q
OL)
P = .0546
EORTC global QoL DSQL skin satisfaction100 –
90 –
80 –70 –
60 –
50 –
40 –
30 –20 –
10 –
0 –Baseline Week 6 Month 3 Month 6 Month 9
P<.0001
BevacizumabCetuximab
Chemo/bevacizumab Chemo/cetuximab

Sequence:

Sequence: All RAS WT:
1st Line Chemo + Anti-VEGF
2nd Line Chemo + Anti-VEGF
3rd Line Chemo + Anti-EGFR
Khattak et al. Clinical Colorectal Cancer, Vol. 14, No. 2, 81-90 a 2015

Sequence versus Exposure:
Modest et al. J Clin Oncol 33. © 2015 by American Society of Clinical Oncology

Sequence versus Exposure:
Bevacizumab47.1%
Cetuximab or Panitumumab
52.2%
Modest et al. J Clin Oncol 33. © 2015 by American Society of Clinical Oncology

Sequence versus Exposure:
Modest et al. J Clin Oncol 33. © 2015 by American Society of Clinical Oncology
Sequence may be more important than Exposure.

The Art of Today:
• Significant improvement of OAS among patients with mCRC over time.
• Predictive Factors if available are mandatory (All RAS).• Although all treatment options are valid, Sequence of
administration might be more important than exposure (RAS WT).
• Anti-EGFR is a reasonable and more appealing alternative to Anti-VEGF in 1st line treatment of RAS WT.
• Still more research is awaited for better insight.

Is systemic therapy always the best option?

Oligo-metastatic disease at presentation

Treatment options for Oligo-metastases

Slide 24

Progression in our understanding of CRC subtypes

Liquid Biopsy: circulating tumour DNA (ctDNA)

Taking ctDNA into the adjuvant setting

Conclusions

Thank You