Embed Size (px)
Citation preview
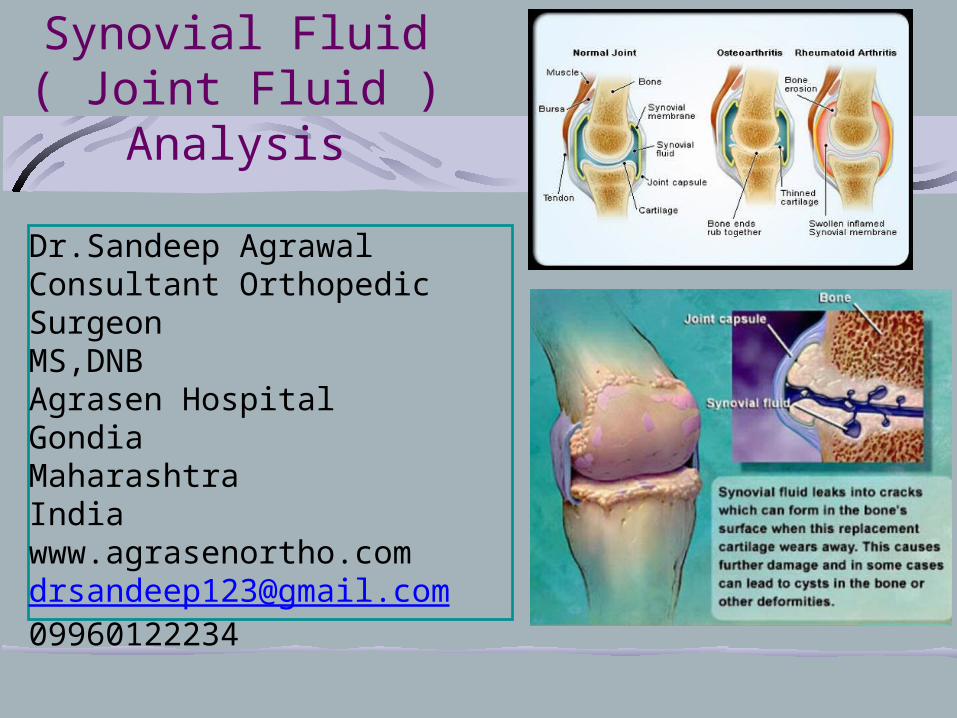
Synovial Fluid ( Joint Fluid )
Analysis
Dr.Sandeep AgrawalConsultant Orthopedic SurgeonMS,DNBAgrasen HospitalGondiaMaharashtraIndiawww.agrasenortho.comdrsandeep123@gmail.com09960122234
Synovial Fluid Synovial
syn(like) + ovia (egg)
“Joint Fluid”
GENERATION AND CLEARANCE OF SYNOVIAL FLUID
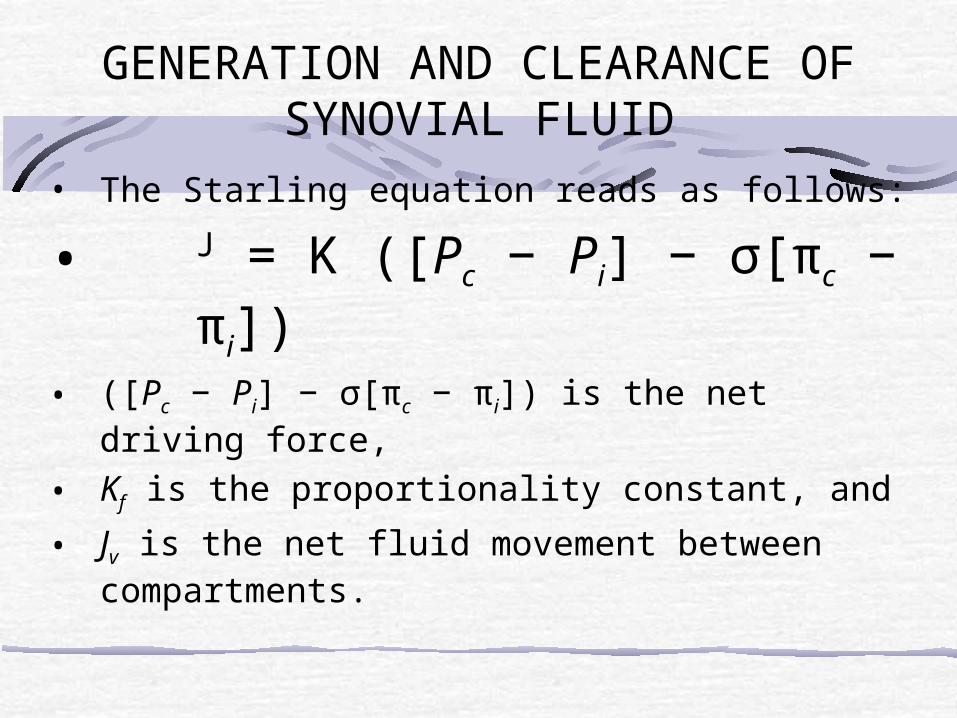
• The Starling equation reads as follows:
• J = K ([Pc − Pi] − σ[πc − πi])• ([Pc − Pi] − σ[πc − πi]) is the net driving force,
• Kf is the proportionality constant, and
• Jv is the net fluid movement between compartments.
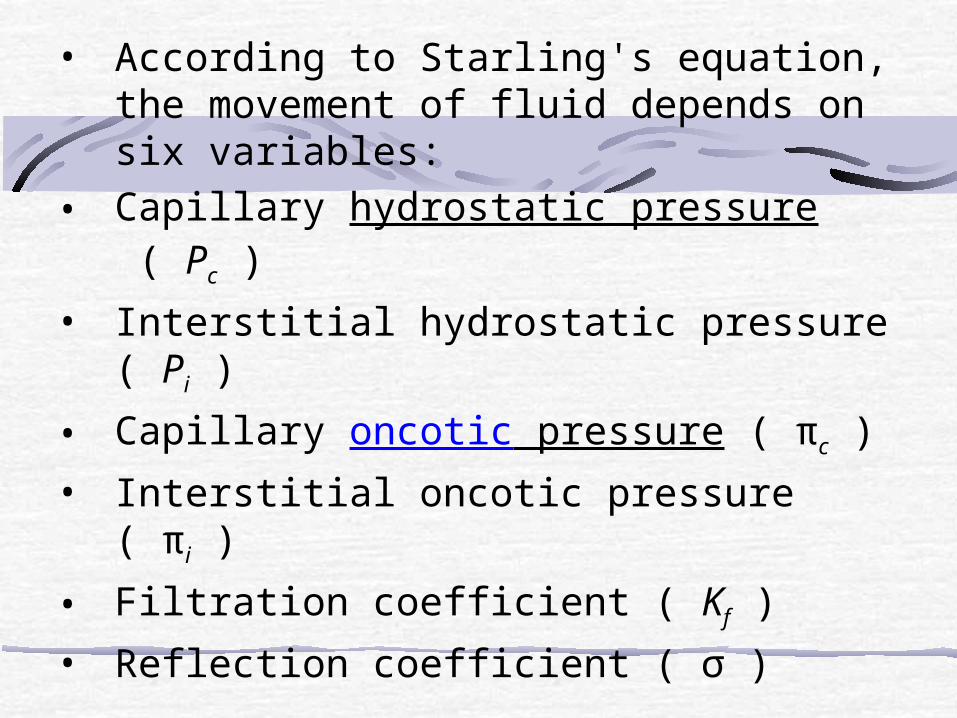
• According to Starling's equation, the movement of fluid depends on six variables:
• Capillary hydrostatic pressure ( Pc )
• Interstitial hydrostatic pressure ( Pi )
• Capillary oncotic pressure ( πc )
• Interstitial oncotic pressure ( πi )
• Filtration coefficient ( Kf )
• Reflection coefficient ( σ )

• Synovial fluid is a mixture of a protein-rich ultrafiltrate of plasma and hyaluronan synthesized by synoviocytes.
• Generation of this ultrafiltrate depends on the difference between intracapillary and intra-articular hydrostatic pressures and between colloid osmotic pressures of capillary plasma and synovial tissue fluid

Synovial Fluid Viscous fluid found in
the cavities of movable joints
Synovial membrane Inner membrane of
synovial joints Secretes synovial fluid
into the joint cavity Contain specialized
cells (synoviocytes)
Synovial fluid….Dialysate of plasma Normal synovial fluid..clear pale or straw coloured , viscous & does not clotContains 0.2 – 0.5% Hyluronan synthesised by type-B synoviocytesIt polymerises to form large molecular weight complexes causing high viscosityRelatively acellular & has a WBC content of <100x106/L :70% mono cytes; 30% lymphocytes
SYNOVIAL FLUID

• In normal joints, intra-articular pressures are slightly subatmospheric at rest (0 to -5 )
• During exercise, hydrostatic pressure in the normal joint may decrease further
• Resting intra-articular pressures in rheumatoid joints are around 20 mm Hg, whereas during isometric exercise, they may increase to greater than 100 mm Hg, well above capillary perfusion pressure and, at times, above arterial pressure

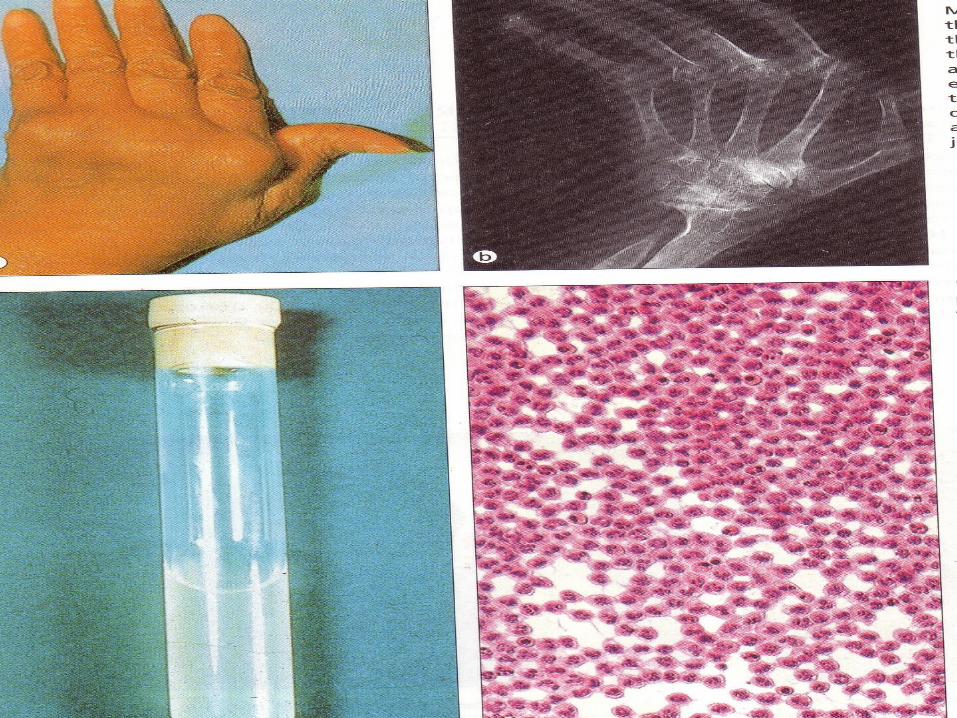
Bulge testThe Bulge test is used to determine if there is an abnormal amount of fluid surrounding a joint
Bulge test of joint for the detection of synovial effusion

Synovial fluid
Physical : viscosity,clarity, colour.Cytology: WBC count, smear for Gram stain, AFB stain,Bacteriology: culture & sensitivityImmunology: immune profile , R.A.
Laboratory Testing Macroscopic Evaluation Chemical Examination Microscopic Examination

Specimen Collection
Arthrocentesis
Placement of needle in arthrocentesis of (A) elbow and(B) knee joints.

Collection Three samples are collected.
NoteIf the specimen cannot be examined immediately, fluid should be frozen and stored at -
70°C until examined
Macroscopic Laboratory Testing Volume Color and Clarity Inclusions Viscosity Clotting Mucin Clot

Macroscopic Analysis: Inclusions
Rice bodies. Free-floating aggregates of tissue appear
as rice bodies. rheumatoid arthritis (RA) Degenarated synovium enriched with
fibrin
Ochronotic shards debris from joint prosthesis look like ground pepper
A =ochronotic shards B =rice bodies
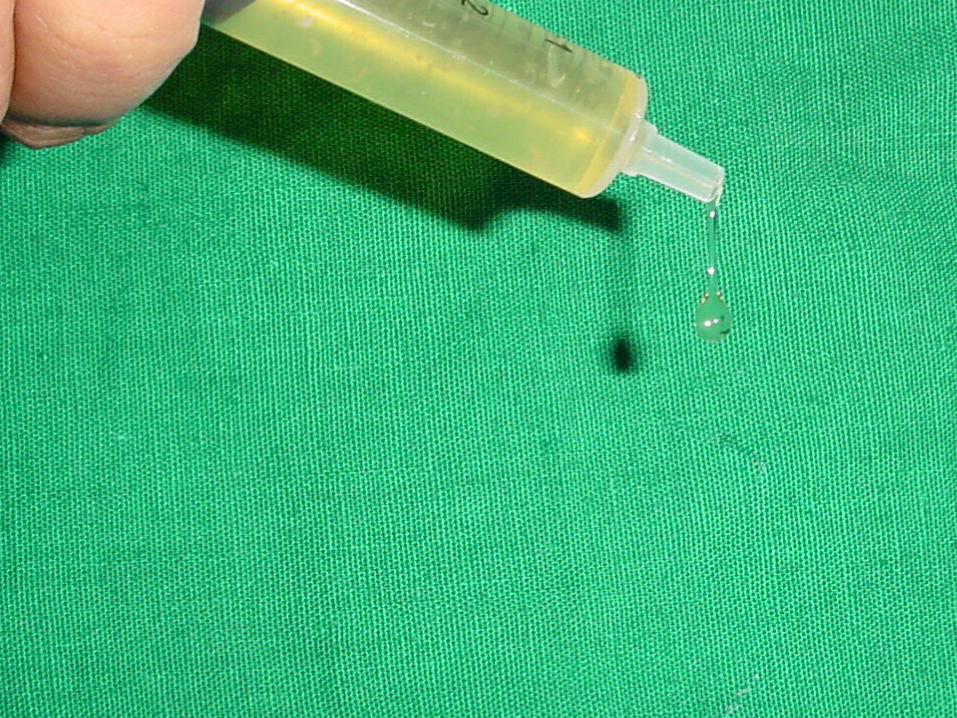
viscosityNon- inflammatory conditions : Normal vis.Inflammatory : low viscosity due to reduced content of hyaluronan & reduced polymerisation (low molecular wt.)String test: synovial fluid dripping from pippette in the form of long string(10-15cm)Inflammatory : fluid falling as free droplets
Colour & clarityDeep yellow In active R.A. slight greenish tingeUniformly blood stained : PVNSLoss of clarity : crystals, increased cellularity, infective, cartilage debrisCorporae oryzae ( rice bodies):T.B., R.A.
WBC COUNTT.C. INFLAMMATORY >2000 x 106/LD.C.polymorphs, lymphocytosis, synoviocytes, chondrocytesClumping of cells can be prevented by collecting in EDTA bottles, or heparin
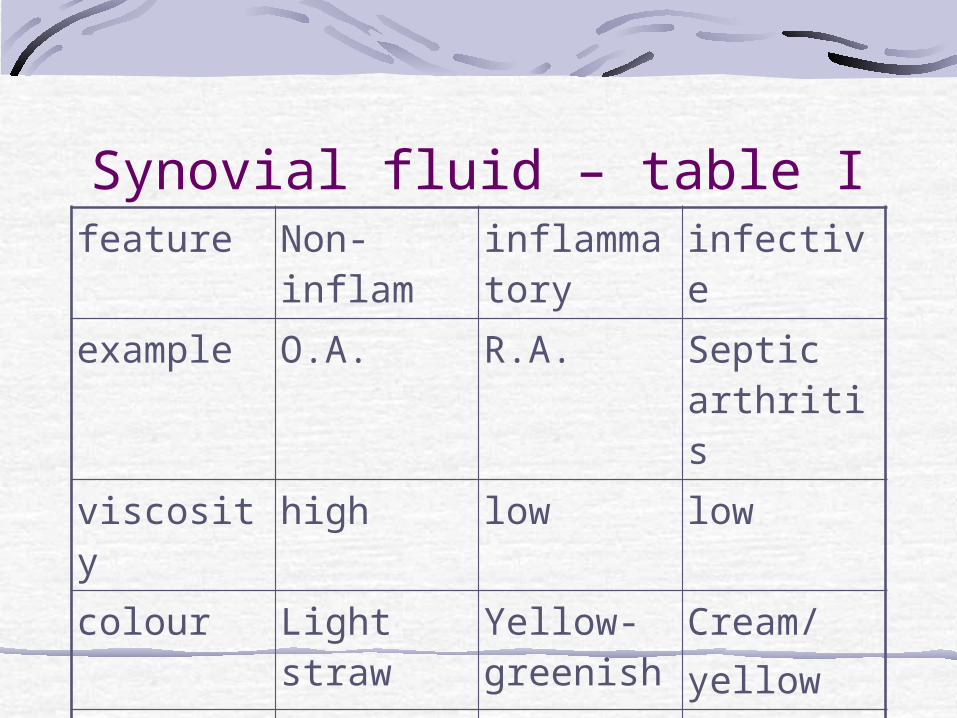
Synovial fluid – table Ifeature Non-
inflaminflammatory
infective
example O.A. R.A. Septic arthritis
viscosity high low low
colour Light straw
Yellow-greenish
Cream/yellow
clarity clear Mild turbid
opaque
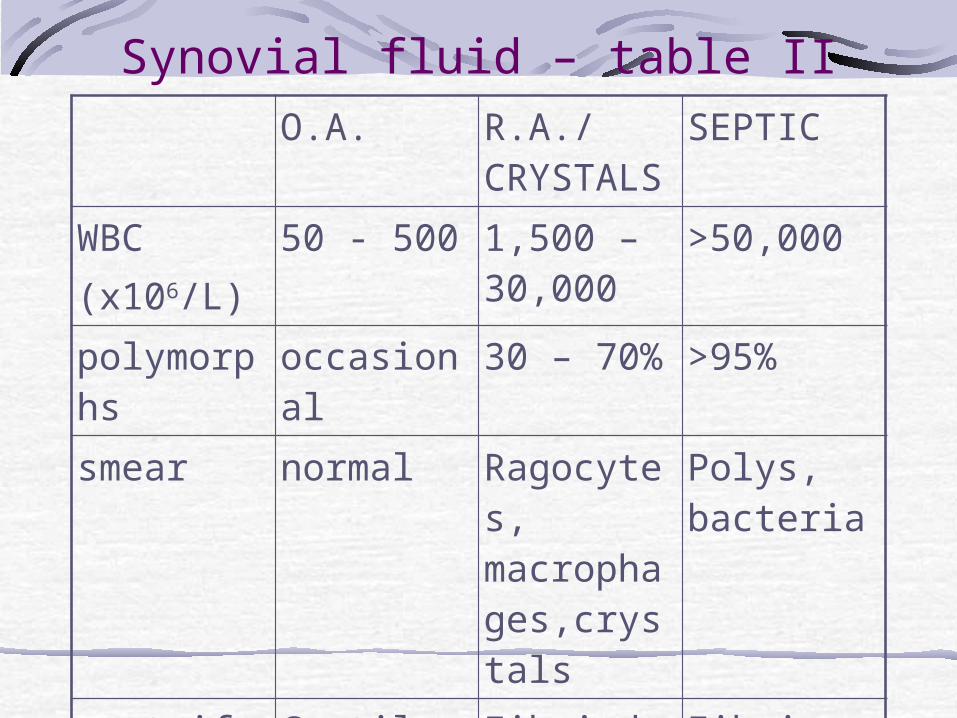
Synovial fluid – table IIO.A. R.A./
CRYSTALSSEPTIC
WBC(x106/L)
50 - 500 1,500 – 30,000
>50,000
polymorphs
occasional
30 – 70% >95%
smear normal Ragocytes, macrophages,crystals
Polys, bacteria
centrifugate
Cartilage & fibrin debris
Fibrindebris/crystals
Fibrin debris, bacteria
R.A. -ve +ve -ve

eosinophilsOccasionally seen in normal syn.fluidIncreased in haemarthrosisFollowing arthrography – contrast inducedParasytic – Lyme arthritis

Microscopic Analysis: Differential LE cells
Neutrophils that have engulfed a nucleus of a lymphocyte
Tart cells Monocytes that
have engulfed nuclear material

Microscopic Analysis: Differential Reiter cells
Vacuolated macrophages with ingested neutrophils
RA cells “Ragocytes” Neutrophils with small,
dark, cytoplasmic granules that consist of precipitated rheumatoid factor

Microscopic Analysis: Differential Hemosiderin
Seen in Pigmented Villonodular Synovitis
Inclusions within clusters of synovial cells
Rice bodies Macroscopically
resemble polished rice Microscopically show
collagen and fibrin

Laboratory Testing: Microbiology Staining
Smears prepared by centrifugation or cytocentrifugation
Saline dilution reduces clustering of cells Gram’s stain most common
Culture
Set up with positive or negative stain results
Aerobic anaerobic

• Proteins are present in synovial fluid at concentrations inversely proportional to molecular size, with synovial fluid albumin concentrations being about 45% of those in plasma
• Synovial fluid is cleared through lymphatics in the synovium, assisted by joint movement
Chemical Analysis: Protein All proteins found in plasma
Exception: various high–molecular weight proteins which may be present in very small amount
Fibrinogen
beta 2 macroglobulin
alpha 2 macroglobulin
Use common serum protein procedures

Synovial fluid analysisRecommended as a routine procedure in the diagnosis of joint disorders by Ropes & Bauer
Hollander introduced the term synovianalysis Hollander & McCarty introduced polarised light microscopy of synovial fluid for identification of crystals of monosodium monourate & calcium pyrophosphateBiochemical analysis for glucose,protein,or lactic acid are not useful

Synovial fluid analysisShmerling (1994) concluded : Two major uses of synovial fluid analysis were to identify or rule out bacterial infection or identification of crystals A total of 6,556 papers were published during 1980 – 2001 on synovial fluid analysis
Infective arthritis
Difficult to differentiate infective arthritis from acute crystal synovitis on clinical examination alone in monoarticular disease
Infection can co-exist with crystal induced or rheumatoid inflammatory arthritis alsoSynovial fluid analysis...Extremely useful to identify crystals & bacteria and culture studies


Crystal induced arthritisImportant cause of acute mono arthritis Gout affects peripheral joints mostly and pseudo-gout or CPPD mainly affects knee jointThe converse is also truePain, swelling redness, sudden onset, and fever mimic infective arthritisIdentification of crystals in syn.fluid is diagnostic
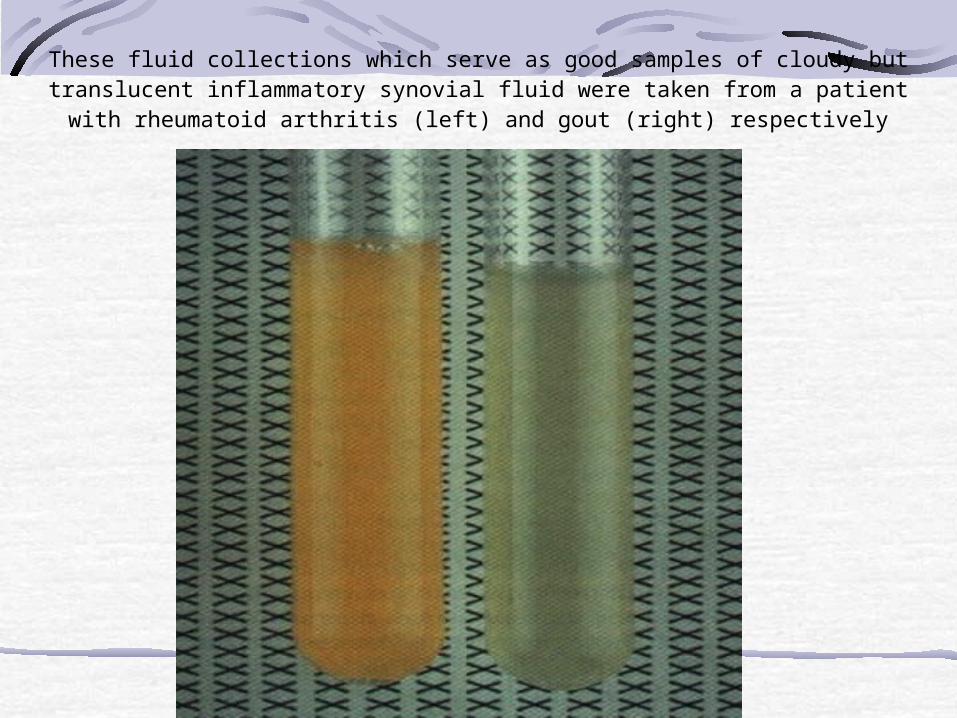
These fluid collections which serve as good samples of cloudy but translucent inflammatory synovial fluid were taken from a patient with rheumatoid
arthritis (left) and gout (right) respectively
Traumatic arthritisFollowing meniscal tears, ligament injuries, haemarthrosis, osteochondral fractures, acute or episodic synovitis of monoarticular nature is common. Syn. Fluid analysis along with arthroscopy can establish the diagnosis and help in treatment
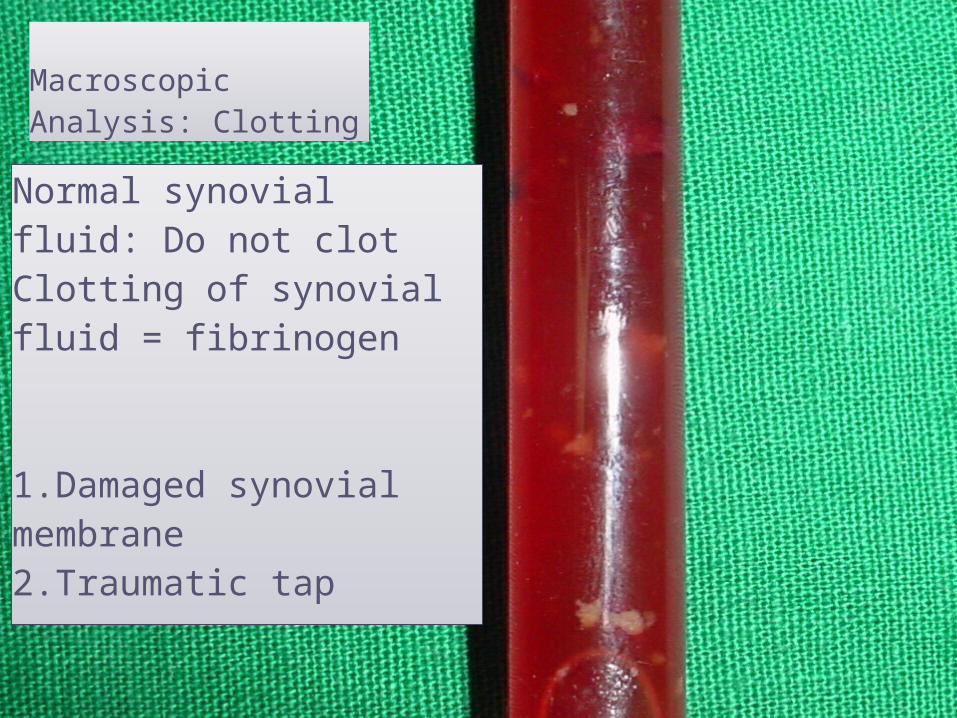
Normal synovial fluid: Do not clotClotting of synovial fluid = fibrinogen
1.Damaged synovial membrane 2.Traumatic tap
Macroscopic Analysis: Clotting
Osteoarthritis
Acute on chronic monoarticular swelling is quite common in degenerative arthritis due to cartilage debris , avascular necrosis, steroid usage, haemoglobinopathies, sickle cell disease , alcoholism and diabetesTumour associated monoarthritis can present without any evidence of underlying pathology . SF analysis helps
Infective arthritisIn a large study(n=242) Weston etal reported that SF Gram staining was +ve in 50% of cases onlySF culture was +ve in 67% of casesBlood culture was +ve when SF gram staining & SF culture were -ve

Syn.fluid analysisShmerling studied sensitivity and specificity of SF analysis critically He concluded that SF analysis was specific in 90% of infective arthritis and sensitivity of gram staining was 50 – 75% and that of SF culture 75 – 95%Freemont etal estimated that in patients on antibiotic therapy SF cultures were +ve in 30 – 80% only and that usage of blood culture bottles for SF culture and using large amount of Syn.fluid improved pick-up rate

Infective arthritisFreemont etal concluded that when parameters like increased polymorph cellcount >2000/cc and usage of special culture media (BACTEC plus Anaerobic /F medium) improved diagnostic sensitivityIn granulomatous lesions with little aspiratable Syn.fluid, syn . tissue can be used for culture purpose

Crystals in Syn.fluidAbsence of crystals in SF does not ruleout crystal induced arthritisMonosodium monourate crystals are needle shaped, negatively bi-refrengent and soluble in waterCrystals must be intra cellular (phagocytosed) to diagnose goutExtracellular cellular crystals in SF donot produce gout
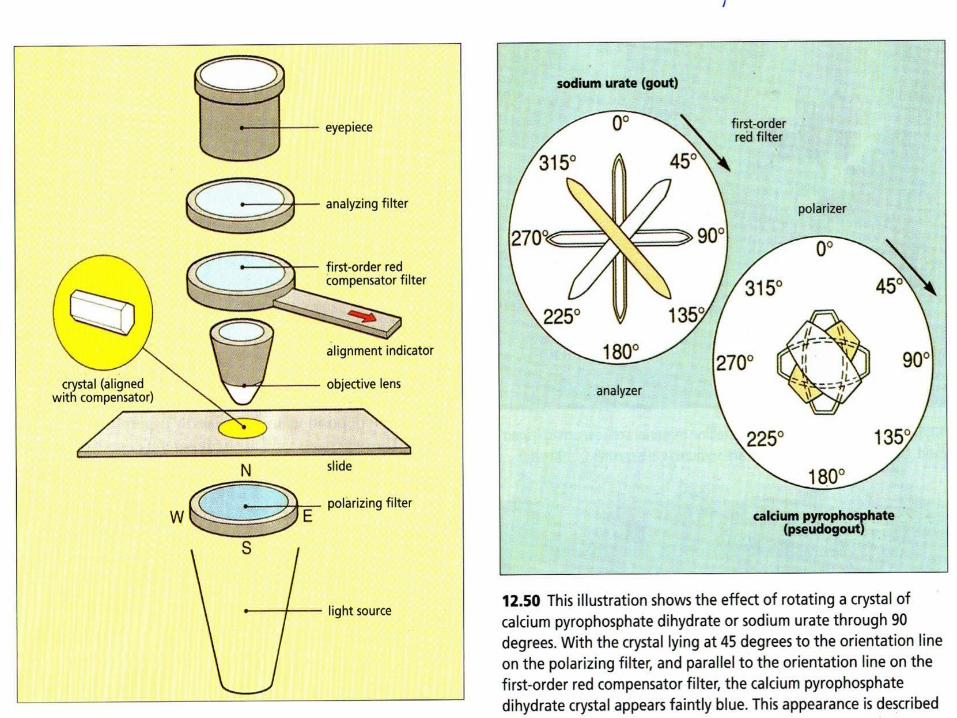

Monosodium urate (MSU)
Calcium pyrophosphate (CPPD)
Crystal Identification
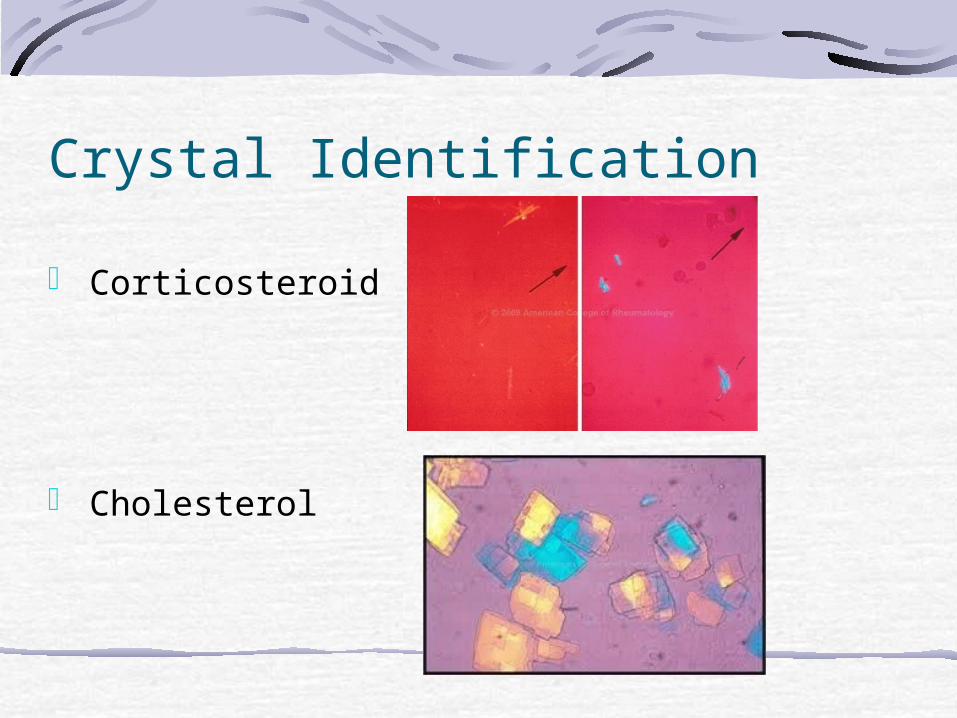
Corticosteroid
Cholesterol
Crystal Identification
Intercritical goutPascual and Jovani studied 101 samples of syn.fluid from asymptomatic gout Results showed 43 out of 43 patients not on treatment for gout had SF +ve for uric acid crystals 34 out of 48 patients receiving treatment for gout had uric acid crystals in SF

Crystals in Syn.fluidCPPD crystals : these are associated with pseudogoutRhomboid in shape and +vely bi-refrengentThey also must be intra-cellular to produce pseudo goutMere presence of these crystals in SF is not diagnostic

Crystals in SFHydroxyapatite crystals are found in syn. Fluid in Milwakee arthritisThese cannot be seen under polarising light microscopyOnly electron microscopy can demonstrate these crystals(TEM)These crystals stain with Alizarin red

Crystals in SFCrystals of other substances like steroids injected can be seen in SFBeclomethasone crystals are needle shaped, but vary in size and shapeCalcium oxalate crystals are particularly seen in SF in renal failure patientsCholesterol crystals can be seen in SF but are of no diagnostic value

Rheumatoid arthritisRheumatoid factor titres in syn.fluid raise much before seropositivityIn the presence of inflammatory SF presence of RAF in SF is diagnostic even if blood RAF is –veRAF in SF is not only derived from blood but also produced by synoviocytes in joint

Laboratory Testing: Rheumatoid Factor RF is an antibody to immunoglobulins.
Present in rheumatoid arthritis:
Serum – most cases
Synovial fluid - 50%
Rarely elevated only in synovial fluid and not serum
False positives in other chronic inflammatory diseases.

Synovial fluid analysisMucin clot test: reflects de-polymarization Of hyaluronic acid and can be demonstrated by precipitation of hyaluronate with acetic acid to form a clot of mucin. One part of syn.fluid is added to 4 parts of 2% acetic acid and briskly stirred.Its quality is interpreted

Macroscopic Analysis: Viscosity “Ropes” or “Mucin
Clot Test” Normal = 4-6 cm
When 2-5% acetic acid is added, normal synovial fluid will form a clot surrounded by clear fluid

Mucin clot testgrade clot solution
good Tight ropy mass
clear
fair Softer,shreddy
Clear/hazy
poor shreddy turbid

“Ropes test” Estimation of hyaluronic
acid–protein complex integrity
The adding of acetic acid to normal synovial fluid, which causes clot formation.
Criteria: Compactness of the clot Clarity of the supernatant fluid
Macroscopic Analysis: Mucin Clot


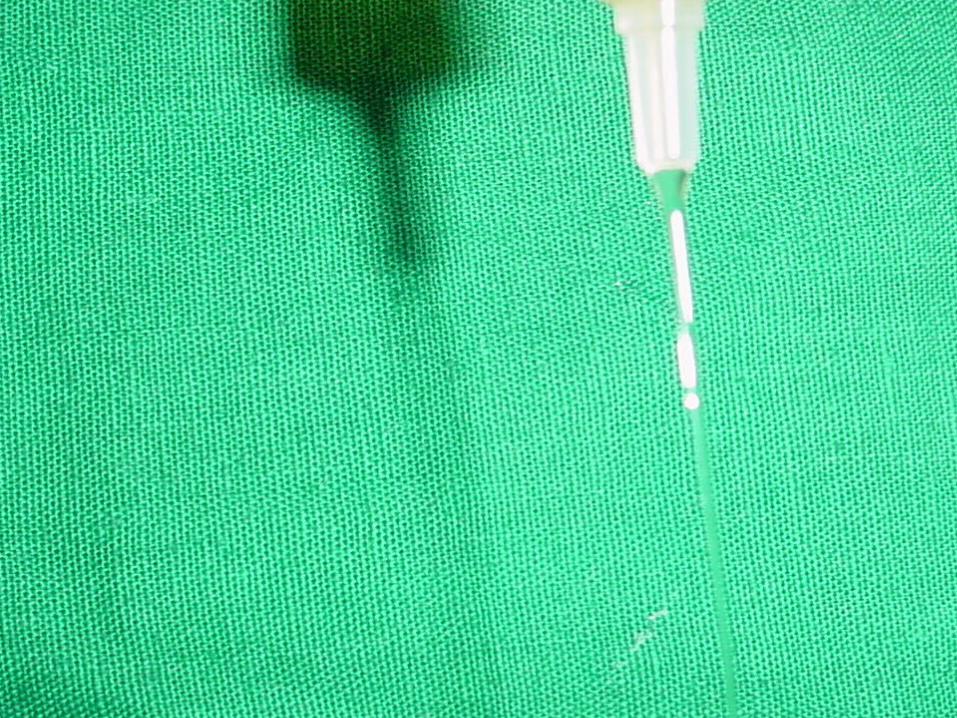
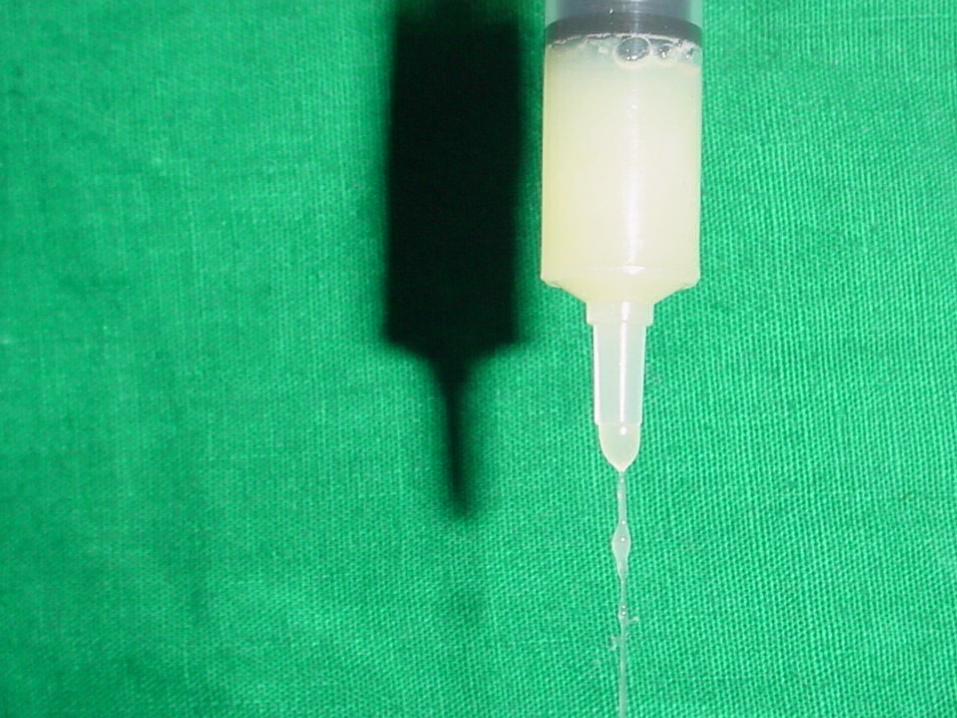
String testSyn.fluid is allowed to fall from the pippetteLength of string is noted Normal: 4 – 6 cm. String (5cm. average)Abnormal : less than 3 cm. String indicates low viscosity or inflammatory effusion

SF analysis vs Syn.biopsyJohnson and Freemont (2000) published a 10 year retrospective study of the diagnostic usefulness of SF analysis and syn. Biopsy103 cases in which both SF analysis and Syn.biopsy were performed were studiedBiopsy gave more information in 29% of cases and SF analysis provided more information in 18% of casesIn cases where syn. Biopsy was more informative, than syn. Fluid analysis 65% were inflammatory arthropathies and 35% were non-inflammatory
SF analysis vs syn.biopsyIn cases where SF analysis was more informative, than syn. Biopsy, 86% were inflammatory and 14% were non-inflammatory

Tuberculous arthritisWallace etal showed that AFB +ve rate depended upon the stage of disease.20% of SF in Tuberculous joints showed AFB +ve on smear80% of SF cultures for AFB were positive in tuberculous joints
Recent advancesBiochemical analysis of SF for glucose, proteins and chloride is of little relevanceMMP3 levels in Syn.fluid reflect the degree of inflammation of a joint and it also correlates with TNF alpha which is a potent inducer of of MMP-3 (matrix metallo protease –3) in synovial fibroblasts, but also of IL- 6 which in turn increases levels of IL -1
Rheumatoid arthritisIL-1 stimulates production of MMP3 MMP3 levels in SF correlate well with SF IL1 levels aswell as with those of its receptors sTNF-RI and sTNF-RII thus corresponding to erosive rheumatoid disease conversely low SF levels of MMP3 correlate with non-erosive rheumatoid disease Detection of MMP3 thus indicates local inflammatory reaction in the joint and it is easy to detect because its concentration is 1000times higher than that of IL-6

Rheumatoid arthritisMeasurement of IL6 remains difficult because of its short half life, presence of blocking factors , and its circadian rhythmThough MMP3 is a synovium derived indicator of inflammatory process, it can also be measured in serum and correlate well with levels of IL-6 and erosive rheumatoid disease – positive predictive value
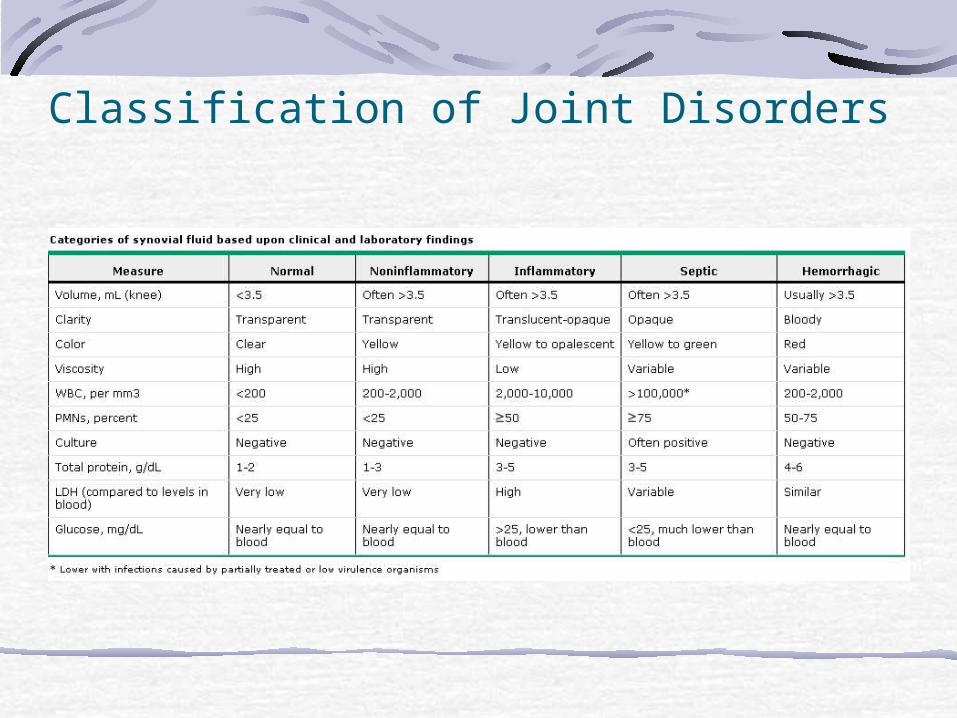
Classification of Joint Disorders



To have a fulfilling life, you should find your life purpose and follow it faithfully. Find whatmatters to you and build the courage to follow it. Having a one-liner will help you internalize and communicate with your mission.
Happiness will never come tothose who fail to appreciatewhat they already have.- Unknown
The more passions and desiresone has, the more ways one
has of being happy.-Charlotte-Catherine

This presentation is for doctors and students in general.. Graphics,Images and jpeg files are taken from Google and yahoo Image to heighten the specific points in this presentation. • If there is any objection/or copyright violation, please inform [email protected] for prompt deletion. • It is intended for use only by the doctors of orthopaedic surgery.. Views expressed in this presentation are personal. • .For any confusion please contact the sole author for clarification. • Every body is allowed to copy or download and use the material best suited to him. There is no financial involvement. • For any correction or suggestion please contact [email protected].





























