Embed Size (px)
Citation preview

Classification of Fractures&
Management of Compound Fractures
By Kevin J Ambadan

CLASSIFICATION
• Based on Relationship with the Environment• Based on Displacement• Based on Fracture Pattern • Based on Etiology

Classification Based on Relationship with Environment
1. CLOSED {Simple}2. OPEN {Compound}

Open Fractures
• A break in the skin and underlying soft tissue leading to a communicating fracture hematoma
Gustilo Classification
• The Gustillo classification is used to classify open fractures.
• Three grades that try to quantify the amount of soft tissue damage associated with the fracture
Grade 1 — <1cm wound, min soft t/s injury Grade 2 — >1cm wound, mod soft t/s inury Grade 3 — >10cm wound, severe muscle devitalization Subgrades A,B,C
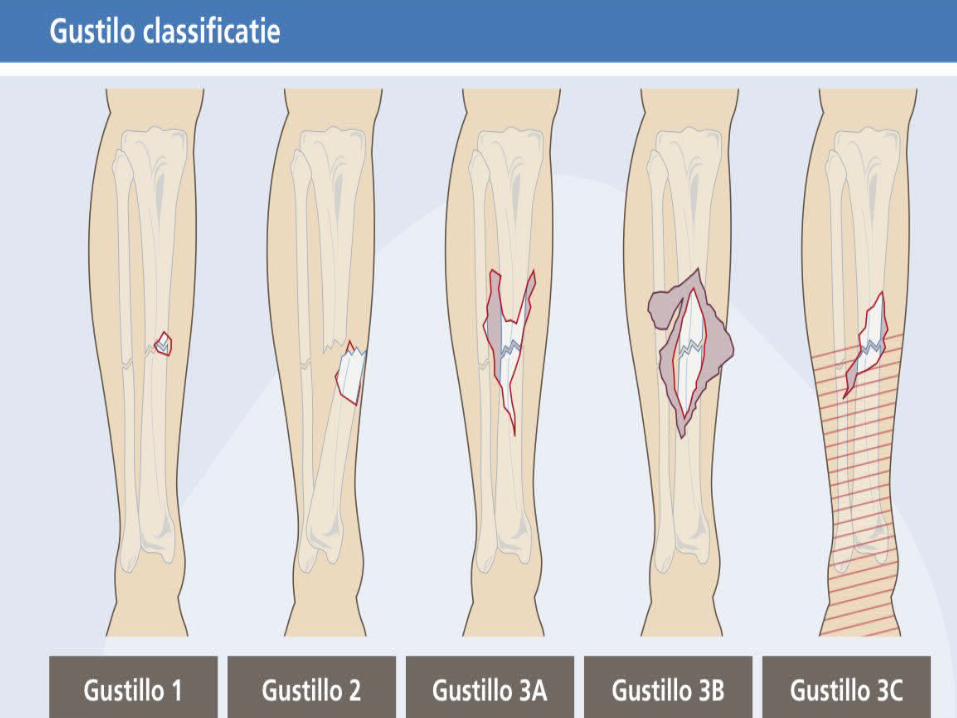

Grade 3A
• Limited stripping of periosteum and soft tissue from bone.
• Adequate soft tissue coverage for bone, tendons and neurovascular bundle.

Type 3B• Extensive stripping of soft tissue and
periosteum from bone. • Requires a local flap or free tissue transfer
Type 3C
• A major vascular injury requiring repair

Muller’s (AO/OTA) Classification• Each long bone has 3 segments
Proximal, Diaphyseal and Distal
• Diaphyseal Fractures:– Simple– Wedge– Complex
• Proximal & Distal– Extra-Articular– Partial Articular– Complete Articular

Classification: Based on Displacement
1. UNDISPLACED2. DISPLACED
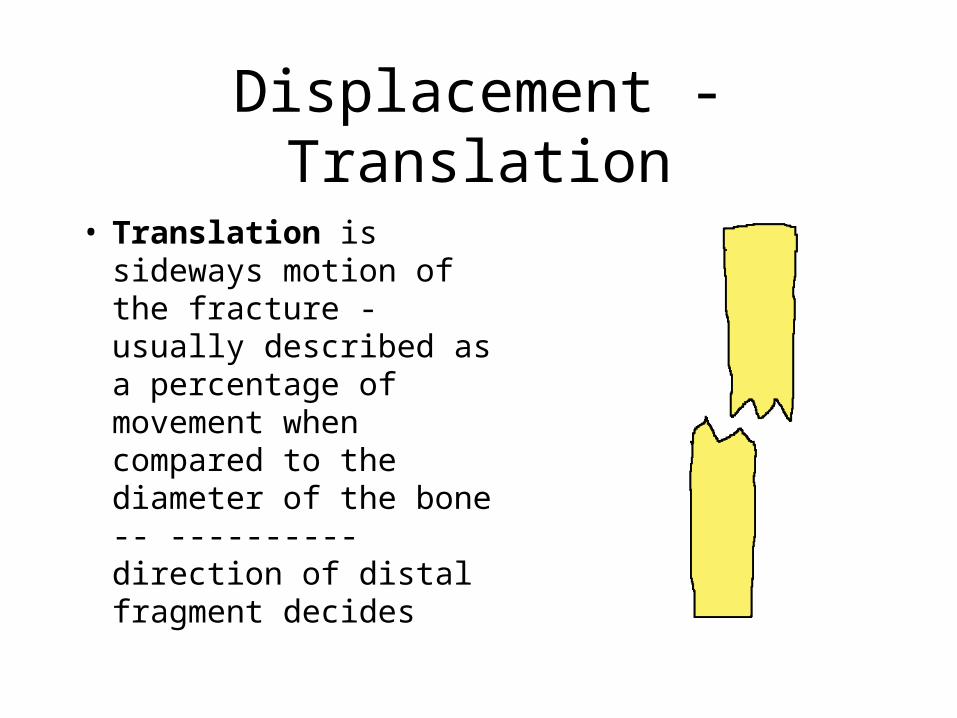
Displacement - Translation
• Translation is sideways motion of the fracture - usually described as a percentage of movement when compared to the diameter of the bone -- ----------direction of distal fragment decides

Displacement - Angulation
• Angulation is the amount of bend at a fracture described in degrees. Described with respect to the apex of the angle .
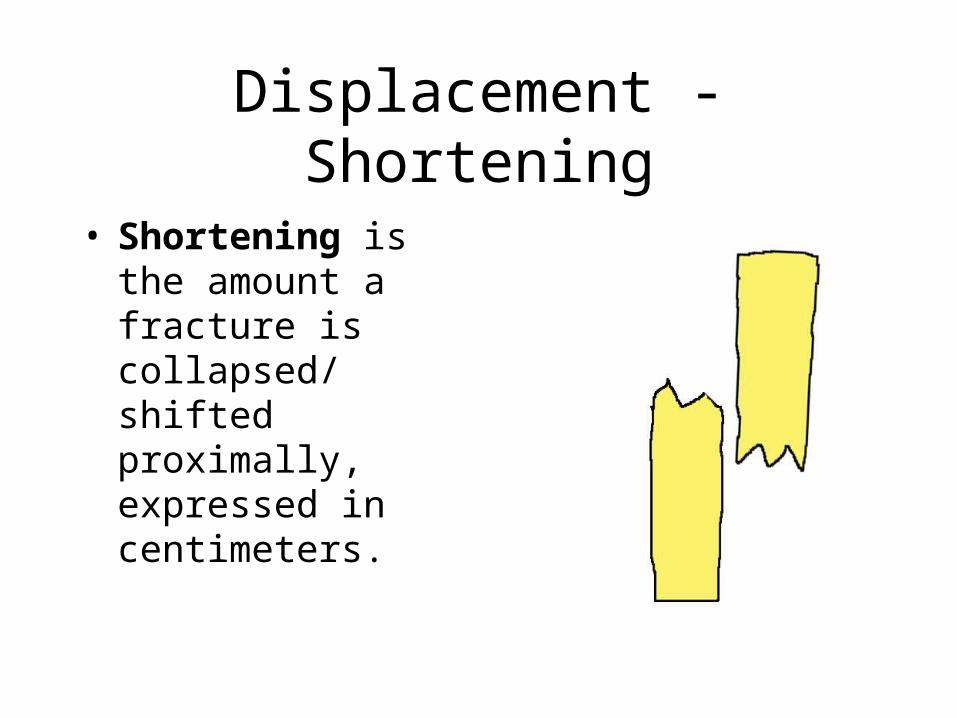
Displacement - Shortening
• Shortening is the amount a fracture is collapsed/ shifted proximally, expressed in centimeters.

Classification: Based on Pattern
1. Transverse2. Oblique3. Spiral4. Comminuted5. Segmental6. Stellate

Transverse Fracture A fracture in which the # line is perpendicular to the long axis of the bone .
Oblique Fracture A fracture in which the # line is at oblique angle to the long axis of the bone.
According to the Path of the # Line

Spiral Fracture A severe form of oblique fracture in which the # plane rotates along the long axis of the bone. These #s occur secondary to rotational force.
According to the Path of the # Line
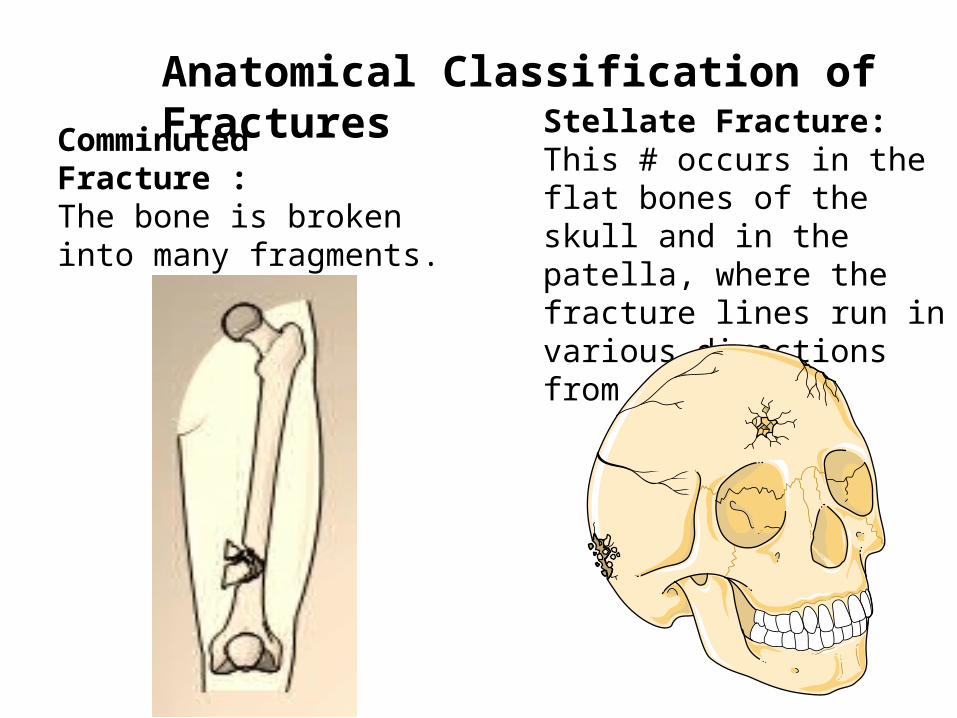
Anatomical Classification of Fractures
Comminuted Fracture : The bone is broken into many fragments.
Stellate Fracture: This # occurs in the flat bones of the skull and in the patella, where the fracture lines run in various directions from one point.

Anatomical Classification of Fractures
Impacted Fracture: This # where a vertical force drives the distal fragment of the fracture into the proximal fragment.
Depressed Fracture: This # occurs in the skull where a segment of bone gets depressed into the cranium.
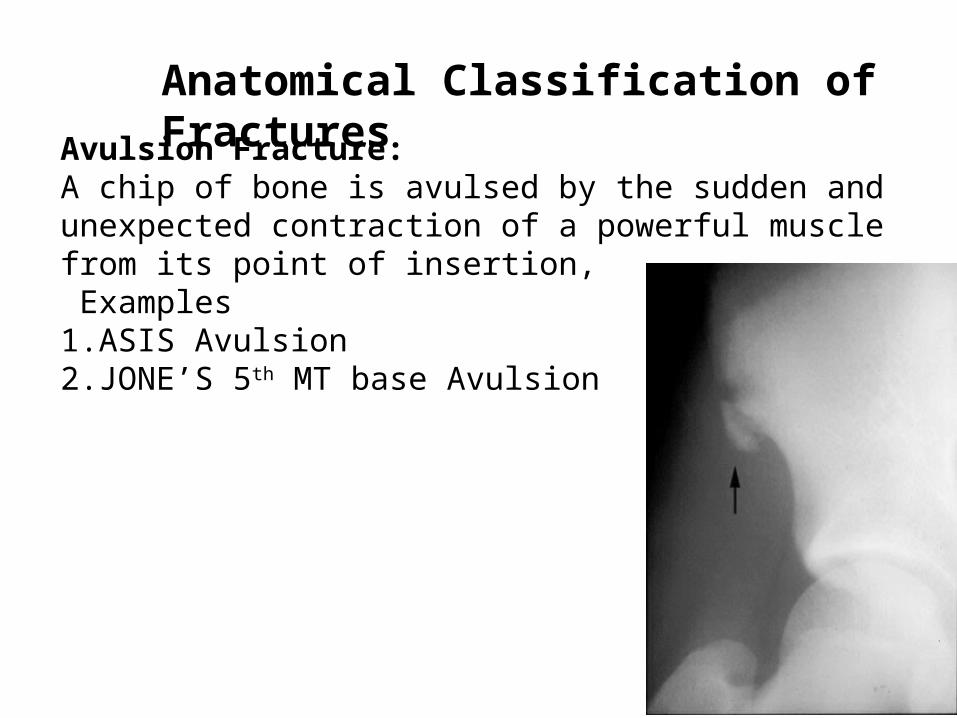
Avulsion Fracture: A chip of bone is avulsed by the sudden and unexpected contraction of a powerful muscle from its point of insertion, Examples1. ASIS Avulsion2. JONE’S 5th MT base Avulsion
Anatomical Classification of Fractures

Stress Fracture : • It is a fracture occurring at a site in the bone subject to
repeated minor stresses over a period of time.
Birth Fracture: • It is a fracture in the new born children due to injury during birth
Anatomical Classification of Fractures

Classification: Based on Etiology
1. TRAUMATIC2. PATHOLOGICAL – Tumors– Bone cysts– Osteomyelitis– Osteoporosis– Osteogenesis imperfecta– Rickets

Salter-Harris Classification• Only used for pediatric fractures that involve
the growth plate (physis)

Salter-Harris type I fracture
• Type I fracture is when there is a fracture across the physis with no metaphysial or epiphysial injury

Salter-Harris type II fracture
• Type II fracture is when there is a fracture across the physis which extends into the metaphysis

Salter-Harris type III fracture
• Type III fracture is when there is a fracture across the physis which extends into the epiphysis

Salter-Harris type IV fracture
• Type IV fracture is when there is a fracture through metaphysis, physis, and epiphysis
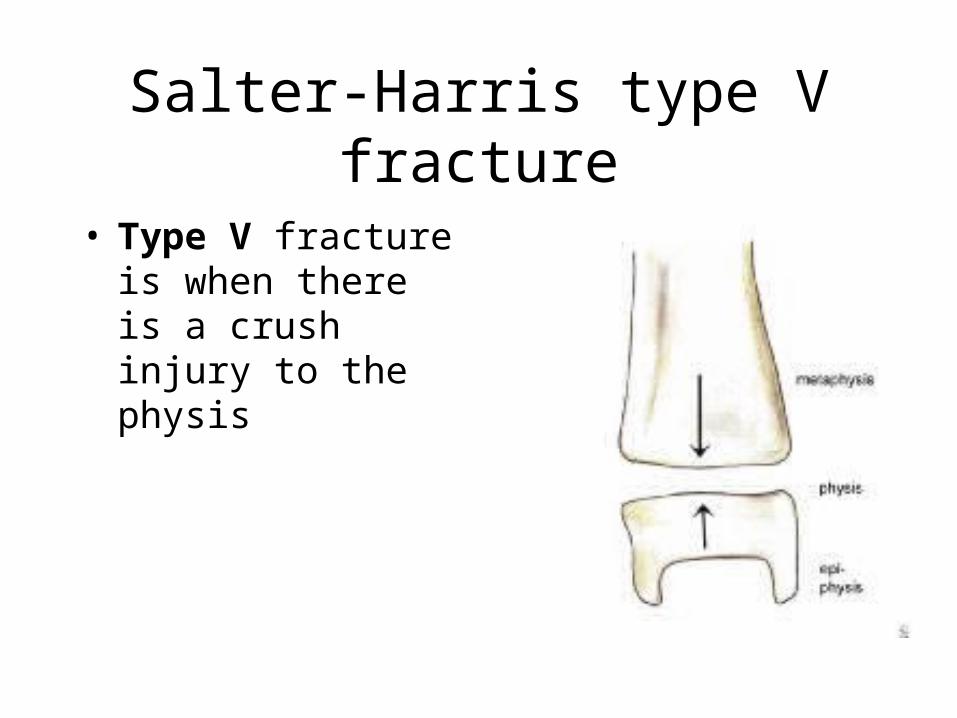
Salter-Harris type V fracture
• Type V fracture is when there is a crush injury to the physis

Treatment of Compound Fracture
Aim• To convert contaminated wound into clean wound • To convert the open # into a closed one.• To establish a union in a good position• To prevent pyogenic and clostridial infection.
Order of Priority• Patient• Limb• Wound• Fracture

4 Essentials of Treatment
• Antibiotic Prophylaxis• Urgent Wound and Fracture Debridement• Stabilization of the Fracture• Early Debridement Wound Cover

Sterility and Antibiotic Cover
• In most cases, Co-amoxiclav or Cefuroxime (or Clindamycin in case of penicillin allergy) is given ASAP
• At time of debridement, Gentamycin is added to a second dose of the 1st antibiotic given
• Wounds of Gustilo Grade 1 fractures can be closed at time of debridement; Antibiotic prophylaxis for up to 24hrs

• Grade 2 and 3A fractures, delayed closure after ‘second look’ is sometimes preferred
• Grade 3B & C, delayed cover is usually practiced.
• Total period of antibiotics is up to 72hrs.
Debridement
• Thorough irrigation of wound with copious amounts of NS to remove all foreign material in wound, followed by excision of dead tissue
• Tourniquet may be used to provide bloodless field, but it can cause ischemia and make it difficult to identify devitalized structures
• Principles observed during debridement:– Wound margin excision– Wound extension– Delivery of fracture– Removal of devitalized tissue– Wound cleansing
• Uncontaminated wound in Grade 1 or 2 can be sutured

Fracture Stabilization
• Important in reducing risk of infection and assisting recovery of soft tissues
• Method of fixation depends on– Degree of contamination– Length of time from injury to operation– Extent of soft tissue damage
• If there is no contamination and definitive wound cover can be achieved at time of debridement, all open #s can be treated as closed injury

• Internal or external fixation may be appropriate depending on individual characteristics of fracture and wound.
• If wound cover is delayed, then external fixation is safer; however fixator pins should be inserted away from potential flaps
• Internal fixation can be used at time of definitive wound cover as long as – delay to wound cover is < 7 days– No visible wound contamination– Internal fixation can control the # as well as
external fixator

Stabilization of Open Fractures METHODS
1.PLASTER IMMOBILISATION
2.PINS & PLASTER
3.SKELETAL TRACTION
4.EXTERNAL FIXATION
5.INTERNAL FIXATION
6.HYBRID FIXATION

External FixatorsMethod of choice in most open fractures
Advantages:• Easily applied • Good skeletal & soft tissue stability• Anatomical reduction.• No additional trauma• Risk of infection is comparatively less.• Allows wound inspection & wound dressing.• Assist in restoring the limb to length until definitive fixation• Allows transportation• Better nursing care

Amputation
Indications:
• Vascular injury – no repair possible
• Functional outcome better with prosthesis
• Life saving to arrest bleeding
• Associated diseases (DM)
Thank You





























