Embed Size (px)
DESCRIPTION
Citation preview

CHRONIC MYELOID LEUKEMIA
Dr.A.MEENAKSHI
PROF.S.TITO’S UNIT.
M4

Definition• Chronic myelogenous leukemia is a pluripotent
stem cell disease characterized by anaemia,extreme blood granulocytosis with immaturity ,basophilia,thrombocytosis and splenomegaly.
• The haemtopoietic cell contain a reciprocal translocation between chromosome 9 and 22 .known as the philadelphia chromosome.
• Occurs more often in men.• Disease of firsts.• High doses of ionising radiation can increase the
occurrence of CML.


Pathophysiology• Genetic hallmark of CML is the presence of
BCR-ABLfusion gene product.• The fusion protein is a result of reciprocal
translocation between the abelson oncogene on chromosome 9 and break point cluster region on chromosome 22.
• Fusion genes are generated that encode 190,210,or 230 kda forms of the BCR-ABL tyrosine kinase.
Other genetic abnormalities• Trisomy 8,p53 loss.• Interleukin 1 b involved in the progression of
CML to the blastic phase.

Clinical presentation Symptoms• Fatigue,malaise• Weight loss• Early satiety • Left upper quadrant pain or mass• Easy bruising ,bleeding• FeverUncommon presentation• Acute gouty arthritis,priapism,myocardial
infarction,venous thrombosis,visual disturbances,sweet syndrome..

Signs• pallor
• Splenomegaly
• Sternal tenderness
• Lymhadenopathy
• Hepatomegaly
• Purpura
• Retinal haemorrhage

Diagnostic approach to CMLPeripheral blood• Granulocytic leukocytosis>50*10p9/l• Predominance of neutrophils and increased %of
myelocytes.• Absolute basophilia.• Platelets are normal or increased in number.Bone marrow• Marrow is hypercellular with granulocytic
predominance.• Megakaryocytes are increased in number with
abnormal morphology.• Increase in reticulin fibrosis.• Blasts less than 5%.

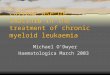
PERIPHERAL SMEAR PICTURE
Band forms

Band forms
promyelocyte
myelocyte
metamyelocyte

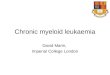
BONE MARROW PICTURE
megakaryocyte

diagnosis of accelarated phase• Blasts 10-20% in peripheral blood and or
bone marrow.
• Basophils >20% in peripheral blood.
• Persistent thrombocytopenia.
• Increasing spleen size and white blood count despite therapy.
• Cytogenetic evidence of clonal evolution.

ACCELERATED PHASE
MYELOBLAST

Blast crisis phase• Blast > 20%
• Extramedullary blast proliferation.
• Large aggregates or clusters of blast in bone marrow.

BLAST CRISIS PHASE
MYELOBLAST

Other abnormalities
There is increase in
• uric acid level
• vitamin B12 level.
• lactate dehydrogenase.
• Increase in the level of angiogenic factors.
• Decrease level of leukocyte alkaline phosphatase.
• Increase in histamine levels.

• Identification of philadelphia chromosome• Can be done by conventional cytogenetic
karyotyping,FISH,RT-PCR.Conventional cytogenetics• Entire chromosomal complement is
evaluated to identify philadelphia chromosome and other abnormalities.
• Can be done on both peripheral blood and bone marrow.
Disadvantage• Presence of cryptic or submicroscopic
BCR-ABL arrangement cannot be identified

Fluorescent insitu hybridisation
Advantage
• Fast results,greater sensitivity than conventional cytogenetics.
• Submicroscopic or cryptic molecular alteration can be detected.
Reverse transciptase-PCR
• Detects different length products corresponding to chimeric BCR-ABL proteins of 190,210 and 230 kda.
• So helps in distinguishing CML from ALL.

Fluorescent insitu hybridisation

Prognostic factorsSokal index• Percentage of circulating blast,spleen
size,platelet count,age and cytogenetic clonal evolution.
• Was developed based on chemotherapy treated patients.
Hassford system• Developed on interferon alpha treated patients.• Includes% of circulating blast,spleen
size,platelet count,age,% of eosinophils and basophils.

Treatment • Drugs • Stem cell transplant.• Leukaphresis and splenectomy.
drugs• Imatinib mesylate,dasatinib,nilotinib• Hydroxyurea• busulphan• Interferon-alpha• Homoharringtonine• Anagrelide.• Cytarabin.

Imatinib• It is an ABL specific tyrosine kinase
inhibitor.• Imatinib induces apoptosis in cells
expressing BCR/ABL.• Dose is 400mg/day.• It should achieve cytogenetic remission
by 6months and molecular remission by 18 months.
• Side effects-edema,pleural and pericardial effusion,nausea,vomiting,diarrhoea,muscle cramps,skin rash,bone pain and arthralgia.myelosuppression.


Criteria for Extent of Imatinib Treatment Hematologic response -White cell count
<10x109(platelet count <450 x 109/L, no immature myeloid cells in the blood, and disappearance of all signs and symptoms related to leukemia (including palpable splenomegaly) lasting for at least 4 weeks.
• Major cytogenetic response-Less than 35% of cells containing the Ph chromosome by cytogenetic analysis of marrow cells.
• Complete cytogenetic response-No cells containing the Ph chromosome by cytogenetic analysis of marrow cells.
• Major molecular response-Blood cell BCR-ABL ratio <0.05% (3-log reduction in PCR signal from mean pretreatment baseline value)
• .Complete molecular response-Blood cell BCR-ABL levels undetectable (usually by nested RT-PCR method).

Guidelines for response to imatinib treatment
Time of observation
unsatisfactory
Suboptimal response
Optimal response
3 NoHR pHR CHR
6 No mcyR mcyR McyR
12 noMCYR McyR CcyR
18 noCcyR CcyR MMR






Newer tyrosine kinase inhibitorsDasatinib• Structurally unrelated to imatinib binds to
the ABL kinase domain.• Side effect-myelosuppression,pleural
effusion,prolongation of QT interval.Nilotinib• Structural derivative of imatinib binds to
ABL kinase domain.• Side effects-rashes,transient elevation of
indirect bilirubin levels and myelosuppression.

Hydroxy urea
• Inhibitor of ribonucleotide reductase.
• Lower the blood counts in 1-2 days.
• Dose is 500-3000 mg/day.
• Side effect-nausea and skin rash.
• Given for patients intolerant to imatinib.
Busulphan
• Gradually lowers the blood counts.
• Dose-6-10 mg/day.
• Should not be used in patients expected to undergo bonemarrow transplantation.

Interferon alpha
• Causes complete haemotologic response in >70% of patients.
• Dose is 5 million units daily by subcutaneous administration.
• Hasford score was developed to predict the survival of patients treated with interferon alpha.
Homoharringtonine
• it is a plant alkaloid causes cytogenetic response in patients in late chronic phase.

Anagrelide
• It is used for treating elevated platelet count in CML.especially in presence of thrombosis and bleeding
Leukapheresis
• Control CMLonly temporarily.
• Used in hyperleucocytic patients where rapid cytoreduction can reverse the symptoms.
• Pregnant patient with CML can be controlled by leukaphresis.

Allogenic stem cell transplant• Outcome depends on patients age,phaseof
disease,type of donor,preparative regimen,graft vs host disease,post transplantation treatment.
• Patients age should be less than 70 years.transplantation from donor should be HLA matched.
• Peripheral blood can be used a source of haemotopoietic progenitor cells.preoperative regimen like cyclophosphamideplus total body irradiationis used.
• Complications-graft vs host disease.

Differential diagnosis
• Chronic myelomonocytic leukemia
• Juvenile myelomonocytic leukemia
• Chronic neutophilic leukemia
• Atypical CML
• Diseases associated with hypereosinophilia.

Chronic myelomonocytic leukemia• Anemia, monocytosis >1000/l; blood blasts <10%;
increased plasma and urine lysozyme; BCR rearrangement absent; uncommon cases with PDGFR- mutation respond to imatinib.
• Chronic eosinophilic leukemia• Blood eosinophil count >1500/l; cardiac and neurologic
manifestations common; a proportion of cases have PDGFR- mutations and are responsive to imatinib mesylate.
Chronic monocytic leukemia• Proportion of monocytes elevated; very rare form of
leukemia.Juvenile myelomonocytic leukemia• Infants and children <4 years; eczematoid or
maculopapular rash; anemia and thrombocytopenia; increased HgF in 70% of cases; neurofibromatosis in 10% of cases; BCR rearrangement absent .