Embed Size (px)
DESCRIPTION
pathology of breast cancer ductal carcinoma , lobular carcinoma In situ , Invasiv , vannusclassification paget disease inflammatory cancer local , lymphatic , blood spreading & metastasis
Citation preview

BY :
ABDULLHA TASKIN ABDULBARI
4TH YEAR MEDICAL STUDENT – SULAIMAN ALRAJHEE COLLGES

NORMAL HISTOLOGY OF THE BREAST 2 cell types :–
line ducts lobules.
1. Contractile MYOEPITHELIAL CELLS lie on the BM assist in milk ejection during lactation & provides structural support to the lobules
2. EPITHELIAL CELLS Luminal –produce milk.
Epithelial & Myoepithelial cells lie on the basement membrane.

Breast cancer may arise from the epithelium of the duct system
• anywhere from the nipple end of the major lactiferous ducts to the terminal duct unit, which is in the breast lobule.
• The disease may be • in situ
• Or : invasive cancer.
• The degree of differentiation of the tumour is usually described using three grades:
• well differentiated,
• moderately differentiated or
• poorly differentiated.




• Ductal carcinoma is the most : common variant with lobular carcinoma
• occurring in up to 15 per cent of cases.
• There are sub- types of lobular cancer including:
• the classical type : which carries a better prognosis than
• the pleomorphic type.
• Occasionally, the picture may be mixed with both ductal and lobular features.
• immunohistochemical : analysis using the e-cadherin antibody, which reacts positively in lobular cancer, will help in diagnosis.

RARER HISTOLOGICAL VARIANTS
• colloid or mucinous carcinoma:
• whose cells produce abundant mucin,
• medullary carcinoma,
• with solid sheets of large cells often associated with a marked lymphocytic reaction,
• tubular carcinoma.
• Invasive lobular carcinoma is commonly multifocal and/or bilateral, hence the increasing use of MRI for assessment.
•

• Inflammatory carcinoma
• Rare
• highly aggressive cancer
• presents as a :
• painful, swollen breast, which is warm with cutaneous oedema.
• This is the result of :
• blockage of the subdermal lymphatics with carcinoma cells.
• Inflammatory cancer : usually involves at least one-third of the breast and may mimic a breast abscess.
• A biopsy : will confirm the diagnosis and show undifferentiated carcinoma cells.

In situ carcinoma :
• is prei-nvasive cancer that has
• not breached the epithelial basement membrane.
• usually : asymptomatic, finding in breast biopsy specimens
• > 20 % of cancers detected by screening in the UK.
• In situ carcinoma may be:
• ductal (DCIS) or
• lobular (LCIS), the latter often being multi-focal and bilateral.
• Both are markers for the later development of invasive cancer,
• which will develop in at least 20 per cent of patients.
• mastectomy : is curative !!

DCIS may be classified using, the Van Nuys system
• which combines the patient’s :
• age, type of DCIS and presence of microcalcifica-tion, extent of resection margin and size of disease.
• Patients with a high score : benefit from radiotherapy after excision,
• low grade : whose tumour is completely excised, need no further treatment.

Staining for oestrogen and progesterone receptors :
• now considered routine,
• their presence :
• Rx : adjuvant hormonal therapy with tamoxifen or an aromatase inhibitor
Staining for c-erbB2 (also known as HER-2/neu) :
• positive > Rx > : monoclonal antibody trastuzumab (Herceptin®),

Paget’s disease of the nipple :
• is a superficial manifestation of an underlying breast carcinoma.
• It presents as :
• an eczema-like condition of the nipple and areola, which persists despite local treatment.
• The nipple is eroded slowly and eventually disappears.
• If left, : the underlying carcinoma will sooner or later become clinically evident
• nipple eczema : should be biopsied if there is any doubt about its cause.

• Microscopically:
• characterised by : the presence of :
• large, ovoid cells with abundant, clear, palstaining cytoplasm
• in the Malpighian layer of the epidermis.


The spread of breast cancer :
•Local
•Lymphatic
•Blood stream

Local spread :
• The tumour increases in size
• and invades other portions of the breast.
• It tends to involve : skin , pectoral muscles and chest wall.
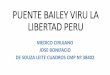
Lymphatic metastasis :
• primarily : to the axillary and the internal mammary lymph nodes.
• Tumours in the posterior one-third of the breast are to drain to :
• the internal mammary nodes.
• It represents :
• the spread of the carcinoma .
• marker for the metastatic potential of that tumour.

LYMPHATIC DRAINAGE
OF BREAST

Spread by the bloodstream :
• It is by this route that skeletal metastases occur :
• the lumbar vertebrae, femur, thoracic vertebrae, rib and skull are affected
• these deposits are generally osteolytic.
• Metastases may also commonly occur in :
• the liver, lungs and brain and, the adrenal glands and ovaries.