Embed Size (px)
Citation preview

الرحمالرحماللهاللهبسمبسمالرحيمالرحيمنن
الرحمالرحماللهاللهبسمبسمالرحيمالرحيمنن
علما” “ زدنى رب علما” “وقل زدنى رب وقل

BILIARY BILIARY STRICTURESSTRICTURES
ByBy DR. Ayman AbdAllaDR. Ayman AbdAlla
ProfessorProfessorof of
General and laparoscopic SurgeryGeneral and laparoscopic SurgeryThe Surgical DepartmentThe Surgical Department
Ain Shams UniversityAin Shams University

Types
• Malignant biliary strictures• Benign biliary strictures

Benign biliary strictures
• Difficult t o manage problems• In contrast to malignant biliary
obstructions, in which short-term palliation is often the goal of therapy, benign strictures requires durable repair
• Many of these strictures occur in young age

Causes of BBS
• I- Congenital Strictures• II- Bile Duct Injuries “BDI” A. Post Operative strictures B. Strictures after Blunt or Penetrating Trauma C. Strictures after Endoscopic or Percutaneous Biliary Intubation

Causes of BBS(cont’d)
• III- Inflamatory Strictures A. Cholelithiasis or choledecolithiasis B. Chronic pancreatitis C. Chronic D.U. D. Abscess or Inflammation of Liver or Subphrenic space E. Parasitic Infections F. Recurrent Pyogenic Cholangitis “Oriental Cholangiohepatitis”

Causes of BBS(cont’d)
• IV- Primary Sclerosing Cholangitis”PSC”
• V- Radiation Induced Strictures• VI- Papillary Stenosis

BDI
• Post operative Strictures1) Cholecystectomy or CBD Exploration2) Biliary – enteric anastomosis3) Hepatic resections4) Portocaval shunt5) Pancreatic surgery6) Gastrectomy7) Liver transplantation


Laparoscopic cholecystectomy Laparoscopic cholecystectomy (LC)(LC)
• Late 1980sLate 1980s• Gold standard for management of benign gallbladder diseaseGold standard for management of benign gallbladder disease• Compared with laparotomy Compared with laparotomy
• Less post-op painLess post-op pain• Shorter hospital stayShorter hospital stay• Earlier return to normal activityEarlier return to normal activity• Better cosmesisBetter cosmesis• Iatrogenic bile duct injury rate Iatrogenic bile duct injury rate
» 0.1% to 0.2% (open) vs 0.4% to 0.6% (lap)0.1% to 0.2% (open) vs 0.4% to 0.6% (lap)

LC has been associated with a higher incidence of IA bile duct injuries LC—0.4 to 0.8% Traditional OC—0.1-0.3%
Association: Increased mortality and morbidity Reduced long-term survival Reduced quality of life
Infrequent—but among the leading sources of malpractice claims against surgeons.
Between 34% and 49% of surgeons are expected to cause such an injury during their career.
Awareness and preventative methods are of clinical importance to surgeons.

• Risk Factors– Anatomical
◦ Anatomical variations (biliary and vasculature)◦ Bleeding, scarring, obesity
– Laparoscopic◦ Lack of Depth Perception, Tactile Feedback, Full Manual
Maneuverability
– Improper surgical approach ◦ Improper Lateral retraction (insufficient or excessive)◦ 0 degree scope◦ Approach plane too deep
– Lack of conversion to OC during difficult cases

– Initially…Surgeon’s Learning Curve –Steady
– Anatomical Misidentification: excision, incision, or transection of biliary anatomy
◦ Injuries: common bile duct, common hepatic duct, right and left hepatic ducts, right hepatic artery, ducts draining hepatic segments
◦ Anatomical variations (biliary and vasculature)
– Electrocautery, thermal injury: stricture of CBD or hepatic ducts, bile leak
– Mechanical trauma: stricture of the biliary ducts, bile leaks
– Improper surgical approach

• Reverse Trendelenburg (30 degrees) with left arm out at 90 degrees relative to the body’s axis
• Titled left 15 degrees after optical trocar placement

Epigastric region, below XP
Mid-A, between 12th rib and ilium
Subcostal, Mid-Clavicular Umbilical
region

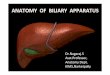
AnatomyAnatomy
• Calot’s triangle – Calot’s triangle – between inferior surface between inferior surface of liver, Cystic duct & of liver, Cystic duct & CHDCHD
• Contents – Cystic artery, Contents – Cystic artery, RHA, Cystic lymph nodeRHA, Cystic lymph node

--Mistaking the common bile duct for the cystic duct

Classical LC BDI

• Inappropriate use of electrocautery near biliary ducts
• May lead to stricture and/or bile leaks
• Mechanical trauma can have similar effects
Lahey Clinic, Burlington, MA.1994

Bile duct injuryclassification
(Bismuth, 1982 Vs. Strasberg, 1992)

Strasberg classification “1995”Strasberg classification “1995”Type Criteria
A Leak from Cystic duct or small ducts in liver bedB Occlusion of an aberrant RHDC Transection without ligation of an aberrant RHDD Lateral injury to a major bile ductE1 Transection >2 cm from the hilumE2 Transection <2 cm from the hilumE3 Transection in the hilumE4 Separation of major ducts in the hilumE5 Type C injury plus injury in the hilum

• Type A Cystic duct leaks or leaks from small ducts in the liver bed
• Type B Occlusion of a part of the biliary tree, almost invariably the
• aberrant right hepatic ducts• Type C Transection without
ligation of the aberrant right hepatic
• ducts• Type D Lateral injuries to major
bile ducts• Type E Subdivided as per
Bismuth classification into E1 to E5

E: injury to main duct (Bismuth, 1982) E1: Transection >2cm from
confluence E2: Transection <2cm from
confluence E3: Transection in hilum E4: Seperation of major
ducts in hilum E5: Type C plus injury in
hilum

• Type 1 Leaks from cystic duct stump or small ducts in liver bed• Type 2 Partial CBD/CHD wall injuries without (2A) or with
(2B) tissue loss• Type 3 CBD/CHD transection without (3A) or with (3B) tissue
loss• Type 4 Right/Left hepatic duct or sectoral duct injuries without
(4A) or with (4B) tissue loss• Type 5 Bile duct injuries associated with vascular injuries
CBD, common bile duct; CHD, common hepatic duct.

Diagnosis

Timing of Identification
• Intra-op
• unexpected ductal structures seen• bile leak into field from lacerated or transected duct
• Post-op
• depends on continuity of bile duct & • presence or absence of bile leak

• Only 25-33% of injures are recognized intraoperatively
• If experienced, convert to Open Procedure and perform Cholangiography (determine extent of injury)
• If not experienced, perform the cholangiogram laparoscopically with intent of referring patient (placement of drains)
• Consult an experienced hepatobiliary surgeon
Quicker the repair, the better the outcome!!!

Clinical Presentation (post-op)• Obstruction
• Clip ligation or resection of CBD obstructive jaundice, cholangitis
• Bile Leak• Bile from intra-op drain or• More commonly, localized biloma or free bile ascites /
peritonitis, if no drain• Diffuse abdominal pain & persistent ileus several days
post-op high index of suspicion possible unrecognized BDI

Intraoperative repair
Conversion! Some Centres do laparoscopic repair, though it is not so simple.
There is no ‘Tissue Lost’, primary repair over T-tube???stricture rate is high!!!
There is ‘Tissue Lost’, biliodigestive anastomosis:choledocoduodenostomy / hepaticojejunostomy

Intraoperative repair

Intraoperative repair
How long you should keep the T-tube?
Previously it was 6 months to 1 year.
Now, after 2 or 3 week, do ERCP and place plastic stents (if possible more than one).

Post-operative diagnosed injury
First control the leak (percutaneous catheter placement, re-laparoscopic drainage, open surgery, nasobiliary drainage etc.) and treat the peritonitis (or even sepsis).
If the fistula is under control, give time for inflammation.
Then try to diagnose the type of injury (MRCP, fistulography, ERCP, PTC)

Post-op diagnosisPost-op diagnosis• Lab investigations• Ultrasound & CT scanUltrasound & CT scan
• intraabdominal collections or ascites, if bile leakintraabdominal collections or ascites, if bile leak• dilatation of biliary tree, if bile duct obstructiondilatation of biliary tree, if bile duct obstruction
• MRCPMRCP• ERCPERCP• PTC PTC • HIDA scan HIDA scan

MRCP / CT cholangiographyMRCP / CT cholangiography• Noninvasive • May avoid invasive procedures like ERCP or PTC• CT cholangiography – not adequate for evaluation of bile
duct
• Do not allow intervention• Interpretatation in presence of bile collection difficult• Potentially delays treatment

CholangiographyCholangiography (ERCP (ERCP ++ PTC) PTC)
• Percutaneous transhepatic cholangiography (PTC)Percutaneous transhepatic cholangiography (PTC)
• defines proximal anatomydefines proximal anatomy
• allows placement of percutaneous transhepatic allows placement of percutaneous transhepatic biliary catheters to decompress biliary tree biliary catheters to decompress biliary tree treats or prevents cholangitis & controls bile leaktreats or prevents cholangitis & controls bile leak

Post-operative diagnosed injury
Biliary leak OR obstruction (type of injury)
Physical examination
There is bilioma / sepsis or not accompanying injury?

ERC – ERC – clips across CBD • CBD transection CBD transection normal- normal-
sized distal CBD upto site of sized distal CBD upto site of transectiontransection
• Percutaneous transhepatic Percutaneous transhepatic cholangiography (PTCcholangiography (PTC) ) necessarynecessary
• SurgerySurgery

Diagnose

Diagnose
Leak from ductus cysticus
(Strasberg A)

Diagnose and treatment
Leak from ductus cysticus (Strasberg A)
Nasobiliary drainage

Diagnose
ERCP
Complete obstruction

Diagnose
PTC (Strasberg E2)

Diagnose
MRCP
(Strasberg E3)

• Controlling sepsis, establish biliary drainage, postulate diagnosis, type and extent of the bile duct injury.
• Broad-spectrum antibiotics• No need for an urgent laparotomy. Biliary reconstruction
in the presence of peritonitis results a statistically worse outcome in patients.
• No need for urgent with reconstruction of the biliary tree. The inflammation, scar formation and development of fibrosis take several weeks to subside.
• Reconstruction of the biliary tract is best performed electively after an interval of at least 6 to 8 weeks.

Definitive management• Goal
• reestablishment of bile flow into proximal GIT• in a manner that prevents cholangitis, sludge or
stone formation, restricturing & progressive liver injury
• Bile duct intact & simply narrowed percutaneous or endoscopic dilatation

Treatment summaryTreatment summary• Strasberg Type A – ERCP + sphincterotomy + stent
• Type B & C – traditional surgical hepaticojejunostomy
• Type D – primary repair over an adjacently placed T-tube (if no evidence of significant ischemia or cautery damage at site of injury)
• More extensive type D & E injuries – Roux an-Y
hepaticojejunostomy over a 5-F pediatric feeding tube to serve as a biliary stent

Indications For Biliary Stenting
Indications for stent insertion include:•Ampullary Stenosis•Bile duct injury•Benign or malignant biliary obstruction•Prevention of obstruction where stone
extraction is not possible at that time•Pancreatic duct strictures, stones and
sphincter of Oddi dysfunction

Stent Placement -Endoscopic Approach
• A catheter is inserted through the endoscope into the ostium of the common bile duct.
• While maintaining the endoscope position in the duodenum, a wire is inserted through the catheter into the bile duct.
• The stent delivery system is then inserted over the wire to the site of obstruction, where the stent is deployed.

Stent Placement – Endoscopic Approach
Success rate of ERCP 90-95%
Complication rate of approximately 3-5%.
Complications:• Pancreatitis• Bleeding• Perforation• Infection• Cardiopulmonary depression from conscious
sedation.

Biliary Stent - Percutaneous transhepatic approach PTC
For biliary stent placement using a percutaneous approach:•A fine needle is inserted between the 4th and 5th rib on the patient’s right side•The puncture is through the liver•The needle is inserted into an intrahepatic duct under image guidance.
Photo on file at Medtronic

Biliary Stent - Percutaneous Approach
Success rate 95% when ducts are dilated• 5-10% rate of major complications which include:•Sepsis•Bile leak•Intraperitoneal haemorrhage, Haemobilia•Hepatic and perihepatic abscess, Pneumothorax•Skin infection and granuloma at the catheter entry site
• Contraindicated in patients with bleeding diatheses and significant ascites.

Surgical repairCholedocho-choledochostomy


Surgical repair Choledocho-duodenostomy

Surgical repair Hepatico-jejunostomy (Roux-en-Y)


Surgical repair Double lumen hepatico-jejunostomy (Roux-en-Y)

Surgical repair Formation of one anastomosis


Surgical repair left hepatic duct anastomosis
(Hepp-Couinaud)


Surgical repair Intrahepatic cholanjio-jejunostomy (Longmire)

Surgical repair Permanent access hepatico-jejunostomy