Embed Size (px)
Citation preview

BACTERIAL AND BACTERIAL-LIKE SEPSIS: DETECTION AND
PREVENTION
Susanna EspositoPediatric Highly Intensive Care Unit
Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano
Milano

Which is the definition of sepsis in children?
1. Proved infection with high fever
2. Systemic inflammatory response
3. Systemic inflammatory response in presence of infection
4. Systemic inflammatory response with cardiovascular dysfunction

DEFINITIONS OF SEPSIS IN CHILDREN (From Goldstein B et al. Pediatr Crit Care Med 2005)

SEPSIS IN CHILDREN: THE BOTTOM LINE
COLD AND WARM SEPTIC SHOCK(From Plunkett A and Tong J, BMJ 2015)

EVENTS LEADING TO DEATH AFTERINFECTION

STANDARDISED CRITERIA FOR ORGAN DYSFUNCTION(From Goldstein B et al., Pediatr Crit Care Med 2005)
Which is the age group at highest risk of sepsis?
1. Infants <1 year
2. Children 1-5 years
3. Children 6-10 years
4. Adolescents
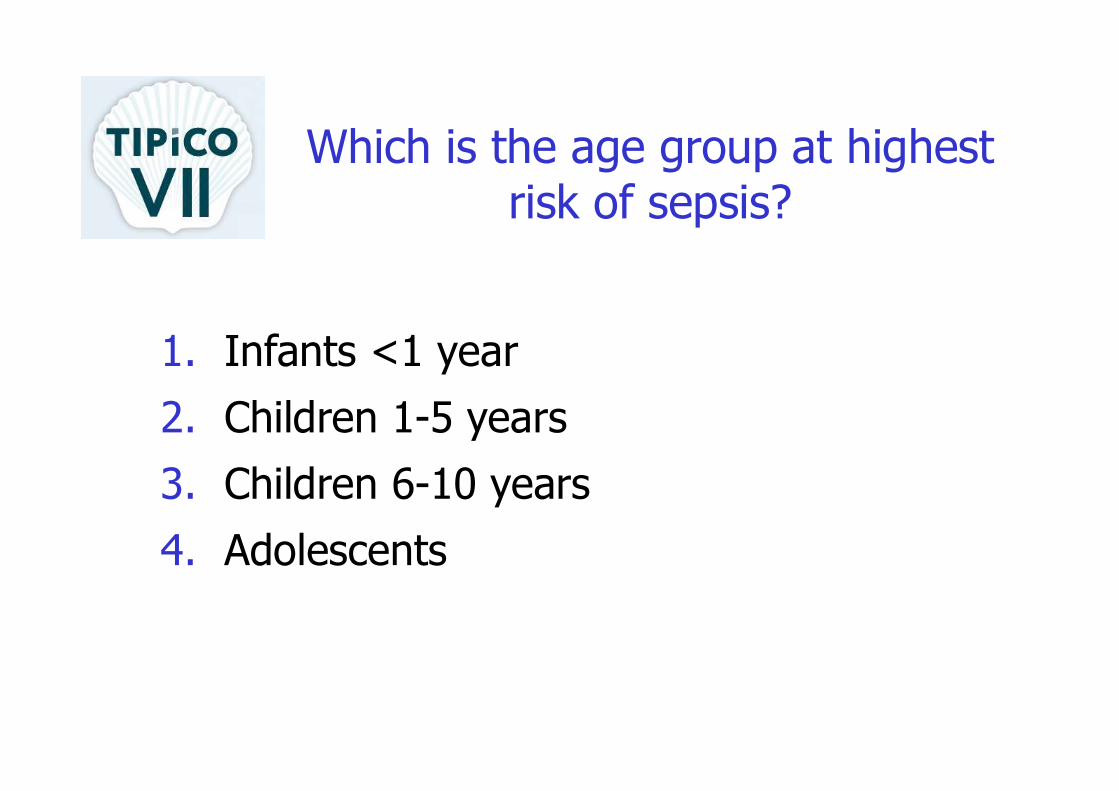
Watson RS et al. The epidemiology of severe sepsis in children in the United States. Am J Respir Crit Care Med 2003;167:695–701
Epidemiology

Epidemiology of severe sepsis in children in USA( Watson RS et al. Am J Respir Crit Care Med 2003;167:695–701)

Number of cases of pediatric severe sepsis diagnosedin the USA from 2004 to 2012
(From Ruth A et al. Pediatr Crit Care Med 2014)

CHARACTERISTICS OF PATIENTS WITH SEVERE SEPSIS
(From Weiss SL et al., Am J Crit Care Med 2015)

SITE OF INFECTIONIN SEVERE SEPSIS OF CHILDREN
(From Weiss SL et al., Am J Crit Care Med 2015)

Differential diagnosisof severe sepsis in children
(From Plunkett A and Tong J, BMJ 2015)
Which is the most frequent etiologic pathogen in pediatric
sepsis?
1. Streptococcus pneumoniae2. Neisseria meningitidis3. Staphylococcus aureus4. Haemophilus influenzae

Typical or important pathogensin pediatric sepsis
(From Plunkett A and Tong J, BMJ 2015)

Early recognition of sepsis and septic shock in children
Recognize signs of poor perfusion (0-5 min)• Decreased mental status • Cold extremities• Delayed capillary refill • Weak pulses, differential central and peripheral pulses
• Low urine output • Hypotension or low BP: minimum systolicBP by age, < 1mo 60 mmHg; 1mo to 10y: 70 + (2 × age in years); ≥10y: 90 mmHg

Treatment of sepsis and septic shock in children (I)
Assess ABCs (0-5 min)
• Provide 100% oxygen at high flow rate (15 L)
• Early intubation may be necessary in neonates and infants
• Breathing assistance as necessary, including mechanical ventilation

Treatment of sepsis and septic shock in children (II)
Establish IV access and place on monitor (0-5 min)• 2 large-bore peripheral IVs (PIVs) preferred: ifdifficult IV, place IO access per PALS guidelines; 1 PIV may be sufficient unlessvasoactive drugs needed
• Consider labs on IV placement: blood gas, lactate, glucose, ionized calcium, CBC, cultures(glucose check through finger stick preferredfor rapid result)

Treatment of sepsis and septic shock in children (III)
Fluid and electrolyte resuscitation (5-15min)Fluids:
• Push 20 mL/kg fluid (isotonic crystalloid) IV/IO over 5-20min or faster if needed (reassessfor signs of shock; see Step No. 11, below)
• Repeat 20 mL/kg bolus push of fluid (up to 60 mL/kg) until clinical symptoms improve or patient develops respiratory distress/rales/ hepatomegaly
• May continue to require additional fluid above 60 mL/kg (fluid refractory) (see Step No. 6, below)
• Fluid needs may approach 200 mL/kg in warm septic shock (warm extremities, flash capillaryrefill)
Correct hypoglycemia:
• Glucose levels in hypoglycemia: Neonates < 45 mg/dL; infants/children < 60 mg/dL
• Glucose dosage: 0.5-1 g/kg IV/IO (max that can be administered through a peripheral vein is25% dextrose in water) (see alternative treatments immediately below)
• Treatment options to provide 0.5-1 g/kg glucose: For infant/child: dextrose 25% in water: 2-4 mL/kg IV/IO; dextrose 10% in water: 5-10 mL/kg IV/IO; for neonate: dextrose 10% in water: 2-4 mL IV/IO; consider maintenance fluid containing dextrose
Correct hypocalcemia for low ionized calcium:
• Calcium gluconate 100 mg/kg IV/IO (max 2g) PRN
• Calcium chloride 20 mg/kg IV/IO PRN ( Note: central line administration preferred over 60 min in nonarrest situation)

Treatment of sepsis and septic shockin children (IV)
Infection control (5-60min)Immediate considerations:• Administer antibiotics immediately after cultures obtained(blood, urine, +/- CSF/ sputum)
• Do not delay antibiotics because of delay in obtaining cultures; initial antibiotics should be given within 1h
General treatment recommendations:• Empiric therapy should be used for unknown etiology of sepsis; • Tailoring of therapy to address suspected pathogens or to achieve adequate drug penetration may be necessary;
• Broader initial coverage may be needed for initial stabilization• Dosing varies by age and weight (consult institution pharmacistand primary medication references for your institution practiceand for preterm infants and neonates <2kg)

Which is the recommended antibiotic treatment in a 12-month-
old child with suspected sepsis?
1. Ampicillin + gentamycin
2. Ceftriaxone
3. Ceftriaxone + vancomycin
4. Cefepime + vancomycin

Treatment of sepsis and septic shock in children (V)
Neonates >2kg:• Ampicillin plus gentamicin: Ampicillin for 0-7d: 50 mg/kg IV/IM/IO q8h;
ampicillin >7d: 50 mg/kg IV/IM/IO q6h plus gentamicin (dosing institutiondependent): 4mg/kg IV/IO/IM q24h (alternative for 0-7d: 2.5 mg/kg IV/IO/IM q12h; alternative for >7d: 2.5 mg/kg IV/IO/IM q8h) or
• Ampicillin plus cefotaxime: Ampicillin for 0-7d: 50 mg/kg IV/IM/IO q8h; ampicillin >7d: 50 mg/kg IV/IM/IO q6h plus cefotaxime 50 mg/kg IV/IO q8h
Infants (>1mo) and children:• Ceftriaxone 75 mg/kg (max 2g) IV/IO/IM q24h plus vancomycin 15mg/kg
(max 1g) IV/IO q8h Immunosuppressed patients:• Vancomycin 15 mg/kg IV/IO (max 1 g/dose) q8h plus cefepime 50 mg/kg
IV/IO (max 2g/dose) q8h; consider antifungal therapyDuration of therapy:• Determined by ultimate source of infection; 7-10d is typically sufficient• Above regimens may be empiric therapy for 48-72h• If culture-negative sepsis, antibiotic choice and duration determined by
severity of presentation and most likely pathogen

Treatment of sepsis and septic shock in children (VI)
Fluid-refractory shock (persisting after 60 mL/kg fluid; 15-60 min)• Continue fluid resuscitation and initiate vasopressortherapy to correct hypotension/poor perfusion
• Central line placement and arterial monitoring if notalready established; vasopressors should not be delayedfor line placements
• Normotensive shock (impaired perfusion but normal bloodpressure): dopamine 2-20 mcg/kg/min IV/IO, titrate to desired effect; if continued poor perfusion, considerdobutamine infusion 2-20 mcg/kg/min IV/IO, titrate to desired effect (may cause hypotension, tachycardia)
• Warm shock (warm extremities, flash capillary refill): Norepinephrine 0.1-2 mcg/kg/min IV/IO infusion, titrateto desired effect
• Cold shock (cool extremities, delayed capillary refill): Epinephrine 0.1-1 mcg/kg/min IV/IO infusion, titrate to desired effect

Treatment of sepsis and septic shock in children (VII)
Shock persists following vasopressor initiation (60 min)• Continued fluid replacement; obtain CVP measurement to guide • SvO2 < 70% (cold shock): transfuse Hgb >10 g/dL; optimize arterial
saturation through oxygen therapy, ventilation; epinephrine 0.1-1 mcg/kg/min IV/IO infusion, titrate to desired effect
• SvO2 < 70% (normal BP but impaired perfusion): transfuse Hgb >10 g/dL; optimize arterial saturation through oxygen therapy, ventilation; consider addition of milrinone 0.25-0.75 mcg/kg/minIV/IO (titrate to desired effect) or nitroprusside 0.3-5 mcg/kg/minIV/IO (titrate to desired effect)
• SvO2 >70% (warm shock): norepinephrine 0.1-2 mcg/kg/min IV/IO infusion

Therapy of sepsis and septic shockin children (VIII)
Fluid refractory and vasopressor-dependent shock) (60 min)• Consider adrenal insufficiency• Hydrocortisone 2 mg/kg (max 100mg) IV/IO bolus; obtain baseline cortisol level; if unsure, considerACTH stimulation test; duration depends on response, laboratory evaluation
Continued shock• Consider cardiac output measurement to directfurther therapy
• Consider extracorporeal membrane oxygenation(ECMO)

Therapy of sepsis and septic shock in children (IX)
Supplemental therapies• Blood transfusion considered for Hgb < 10 g/dL(ideal threshold for transfusion unknown)
• Sedation/analgesia while ventilated• Optimize oxygenation through ventilation• IV immunoglobulin can be considered (unknownbenefit)

THERAPEUTIC ENDPOINTS
Clinical• Heart Rate normalized for age• Capillary refill < 2sec • Normal pulse quality• No difference in central and peripheral pulses• Warm extremities• Blood pressure normal for age• Urine output >1 mL/kg/h • Normal mental status • CVP >8 mmHgLaboratory• Decreasing lactate• SvO2 >70%

Which is the mortality rate in children with sepsis in absence of
comorbidities?
1. 5-10%
2. 10-20%
3. 20-30%
4. 30-40%

Mortality for pediatric sepsis according to age and presence of at least one comorbidity
(Weiss SL et al., Am J Crit Care Med 2015)

Outcomes of pediatric sepsis according to age
(Weiss SL et al., Am J Crit Care Med 2015)
Which is the best way to reduce the burden of pediatric sepsis?
1. Correct diet and life-stype
2. Large use of antibiotics
3. No vaccination
4. Universal vaccination against Hib, pneumo and meningo

NorvegiaVT-IPDd
100%(<2 anni)
DanimarcaVT-IPDd
84%(<2 anni)
GermaniaVT-IPDc
83%(<2 anni)
SpagnaVT-IPDd
84%(<15 anni)
NicaraguaPolmonitea
33%(<1 anno)
USAPolmoniteb
27%(<2 anni)
UKVT-IPDc
89%(<2 anni)
USAVT-IPDb
93%(<5 anni)
IsraeleVT-IPDb
79%(<5 anni)
IsraeleOM pneumococcica
66%(<2 anni)
FranciaVT-IPDd
84%(<2 anni)
FranciaVT-Polmonitec
74%(<16 anni)
Impact of PCV13 on IPD
a Ospedalizzazioni per polmoniteb 5 sierotipi addizionali per IPD: 1, 3, 5, 7F e19Ac 6 sierotipi addizionali per IPD/CAP: 1, 3, 5, 6A, 7F e 19Ad Tutti i sierotipi inclusi in PCV13
IPD
Polmonite
Otite Media

Impact of Synflorix™ on IPD
Quebec (Canada)IPD
COMPASPanama
Colombia Argentina
CAP, NP carriage, AOM
ChileIPD, CAPClinical trial
Impact / effectiveness
FinIP (Finland)IPD, Antibiotics, CAP,
Antibiotic use, NP carriage
FinlandIPD
2+1After PCV7
3+1No PCV7
3+1No PCV7
3+0No PCV7
2+1No PCV7
3+1 & 2+1No PCV7
The NetherlandsIPD, AOM
3+1After PCV7
New ZealandIPD, AOM
3+1After PCV7
IcelandIPD, meningitis, CAP, AOM, antibiotic use
BangladeshIPD, pneumonia
3+0NoPCV7
3+1No PCV7
BrazilIPD, meningitis, CAP,
carriage
3+1No PCV7
Kilifi (Kenya)IPD, carriage

INCIDENCE OF SEROGROUP C DISEASE IN COUNTRIES THAT HAVE INTRODUCED PUBLIC
MCC VACCINATION PROGRAMMES
Trotter & Ramsay, FEMS Microbiol Rev 2007
36 MEN-BEX-P-S-573-152012
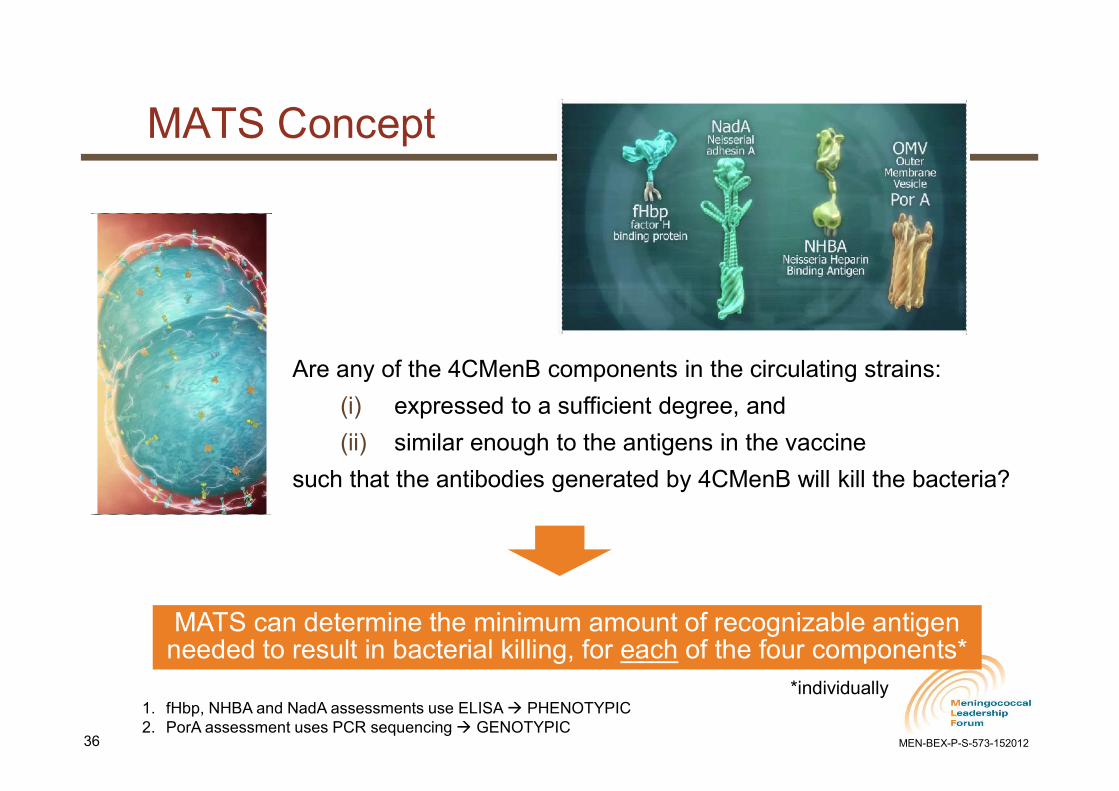
MATS Concept
Are any of the 4CMenB components in the circulating strains:
(i) expressed to a sufficient degree, and
(ii) similar enough to the antigens in the vaccine
such that the antibodies generated by 4CMenB will kill the bacteria?
MATS can determine the minimum amount of recognizable antigen needed to result in bacterial killing, for each of the four components*
1. fHbp, NHBA and NadA assessments use ELISA PHENOTYPIC2. PorA assessment uses PCR sequencing GENOTYPIC
*individually
37 MEN-BEX-P-S-573-152012
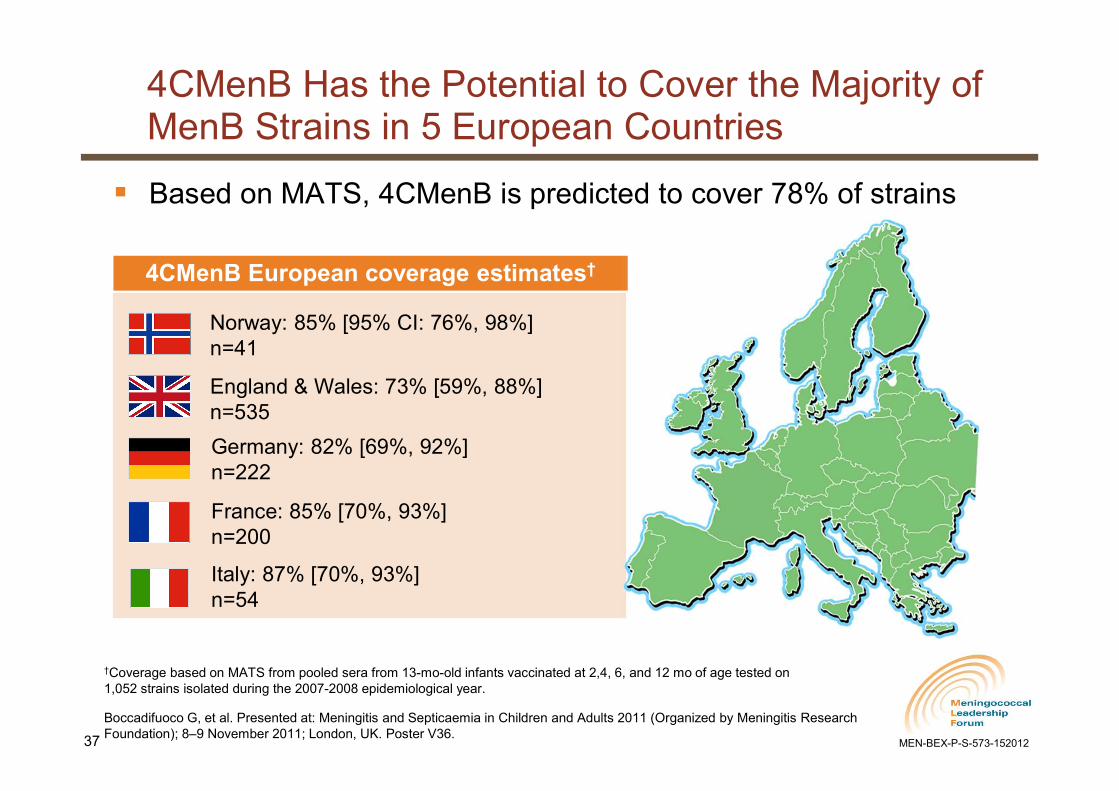
Based on MATS, 4CMenB is predicted to cover 78% of strains
†Coverage based on MATS from pooled sera from 13-mo-old infants vaccinated at 2,4, 6, and 12 mo of age tested on 1,052 strains isolated during the 2007-2008 epidemiological year.
Boccadifuoco G, et al. Presented at: Meningitis and Septicaemia in Children and Adults 2011 (Organized by Meningitis Research Foundation); 8–9 November 2011; London, UK. Poster V36.
Norway: 85% [95% CI: 76%, 98%]n=41
France: 85% [70%, 93%]n=200
Germany: 82% [69%, 92%]n=222
Italy: 87% [70%, 93%]n=54
England & Wales: 73% [59%, 88%]n=535
4CMenB European coverage estimates†
4CMenB Has the Potential to Cover the Majority of MenB Strains in 5 European Countries


Gràçie[in zeineise]